
National Transportation
Safety Board
Washington, D.C. 20594
OFFICIAL BUSINESS
Penalty for Private Use, $300
PRSRT STD
Postage & Fees Paid
NTSB
Permit No. G-200
In-Flight Engine Failure and Subsequent
Ditching
Air Sunshine, Inc., Flight 527
Cessna 402C, N314AB
About 7.35 Nautical Miles West-Northwest of
Treasure Cay Airport, Great Abaco Island,
Bahamas
July 13, 2003
Aircraft Accident Report
NTSB/AAR-04/03
PB2004-910403
Notation 7671A
National
Transportation
Safety Board
Washington, D.C.
National
Transportation
Safety Board
Washington, D.C.

this page intentionally left blank

Aircraft Accident Report
In-Flight Engine Failure and Subsequent
Ditching
Air Sunshine, Inc., Flight 527
Cessna 402C, N314AB
About 7.35 Nautical Miles West-Northwest of
Treasure Cay Airport, Great Abaco Island,
Bahamas
July 13, 2003
NTSB/AAR-04/03
PB2004-910403 National Transportation Safety Board
Notation 7671A 490 L’Enfant Plaza, S.W.
Adopted October 13, 2004 Washington, D.C. 20594
E
P
L
U
R
I
B
U
S
U
N
U
M
N
A
T
I
O
N
A
L
T
R
A
S
P
O
R
T
A
T
I
O
N
B
O
A
R
D
S
A
F
E
T
Y
N

National Transportation Safety Board. 2005. In-Flight Engine Failure and Subsequent Ditching, Air
Sunshine, Inc., Flight 527, Cessna 402C, N314AB, About 7.35 Nautical Miles West-Northwest of
Treasure Cay Airport, Great Abaco Island, Bahamas, July 13, 2003. Aircraft Accident Report
NTSB/AAR-04/03. Washington, DC.
Abstract: This report explains the accident involving Air Sunshine, Inc., flight 527, a Cessna 402C,
which experienced an in-flight engine failure and was subsequently ditched about 7.35 nautical
miles west-northwest of Treasure Cay Airport, Great Abaco Island, Bahamas. The safety issues
discussed in this report include maintenance record-keeping and practices, pilot proficiency,
Federal Aviation Adminstration (FAA) oversight, and emergency briefings. A safety
recommendation concerning emergency briefings is addressed to the FAA.
The National Transportation Safety Board is an independent Federal agency dedicated to promoting aviation, railroad, highway, marine,
pipeline, and hazardous materials safety. Established in 1967, the agency is mandated by Congress through the Independent Safety Board
Act of 1974 to investigate transportation accidents, determine the probable causes of the accidents, issue safety recommendations, study
transportation safety issues, and evaluate the safety effectiveness of government agencies involved in transportation. The Safety Board
makes public its actions and decisions through accident reports, safety studies, special investigation reports, safety recommendations, and
statistical reviews.
Recent publications are available in their entirety on the Web at <http://www.ntsb.gov>. Other information about available publications also
may be obtained from the Web site or by contacting:
National Transportation Safety Board
Public Inquiries Section, RE-51
490 L’Enfant Plaza, S.W.
Washington, D.C. 20594
(800) 877-6799 or (202) 314-6551
Safety Board publications may be purchased, by individual copy or by subscription, from the National Technical Information Service. To
purchase this publication, order report number PB2004-910403 from:
National Technical Information Service
5285 Port Royal Road
Springfield, Virginia 22161
(800) 553-6847 or (703) 605-6000
The Independent Safety Board Act, as codified at 49 U.S.C. Section 1154(b), precludes the admission into evidence or use of Board reports
related to an incident or accident in a civil action for damages resulting from a matter mentioned in the report.

iii Aircraft Accident Report
Contents
Figures . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .v
Abbreviations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . vi
Executive Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . vii
1. Factual Information . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
1.1 History of Flight . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
1.2 Injuries to Persons. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
1.3 Damage to Airplane . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
1.4 Other Damage . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
1.5 Personnel Information. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
1.5.1 The Pilot . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
1.5.1.1 Flight Check History . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
1.5.2 The Director of Maintenance . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
1.5.3 The Assistant Mechanic . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
1.6 Airplane Information . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
1.6.1 Engines and Propellers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
1.6.1.1 Air Sunshine’s Approved Aircraft Inspection Program. . . . . . . . . . . . . . . . . . . . 10
1.6.1.2 Differential Compression Checks . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
1.6.1.2.1 June 12 to 14, 2003, Differential Compression Checks . . . . . . . . . . . . . . . . 12
1.6.1.3 Time Between Overhauls. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
1.7 Meteorological Information . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
1.8 Aids to Navigation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
1.9 Communications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
1.10 Airport Information. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
1.11 Flight Recorders . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
1.12 Wreckage and Impact Information . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
1.12.1 General . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
1.12.2 Engines and Propellers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
1.13 Medical and Pathological Information . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
1.14 Fire . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
1.15 Survival Aspects . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
1.15.1 General . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
1.15.2 Emergency Briefings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
1.15.3 Personal Flotation Devices. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
1.15.4 Search and Rescue . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
1.16 Tests and Research . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
1.16.1 Cessna Airplane Performance Data . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
1.16.2 Airplane Performance Study . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
1.16.3 Metallurgical Inspections . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
1.16.3.1 Right Engine Cylinder Assemblies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
1.16.3.2 Right Engine Pistons . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
1.16.3.3 Right Engine Crankcase. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27

Contents iv Aircraft Accident Report
1.16.3.4 Right Engine No. 2 Cylinder Hold-Down Studs and Through Bolts . . . . . . . . . 27
1.16.3.5 Cylinder Hold-Down Nuts. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
1.17 Organizational and Management Information . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
1.17.1 Air Sunshine. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
1.17.1.1 Air Sunshine’s In-Flight Engine Failure Procedures. . . . . . . . . . . . . . . . . . . . . . 30
1.17.1.2 Ditching Procedures. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32
1.17.1.3 Company Record-Keeping. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32
1.17.1.3.1 Maintenance Records . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32
1.17.1.3.2 Aircraft Flight Logs. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
1.17.2 Federal Aviation Administration Oversight. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
1.17.2.1 General. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
1.17.2.2 San Juan Flight Standards District Office Preaccident
Oversight of Air Sunshine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
1.17.2.3 Fort Lauderdale Flight Standards District Office
Postaccident Oversight of Air Sunshine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
1.17.2.4 San Juan Flight Standards District Office Postaccident
Oversight of Air Sunshine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
1.17.2.5 Additional Postaccident Actions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35
1.18 Additional Information . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36
1.18.1 Previous Ditching Accidents . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36
2. Analysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37
2.1 General . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37
2.2 Accident Sequence . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37
2.3 Airplane Performance After the Right Engine Failure . . . . . . . . . . . . . . . . . . . . . . . . . . 38
2.4 Right Engine Failure Sequence. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39
2.5 Cause of the Loosened No. 2 Cylinder Hold-down Nuts . . . . . . . . . . . . . . . . . . . . . . . . 40
2.6 Air Sunshine Maintenance Record-Keeping and Practices . . . . . . . . . . . . . . . . . . . . . . 41
2.7 Pilot Proficiency . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43
2.8 Pilot Failure to Use Shoulder Harness . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43
2.9 Emergency Briefings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44
3. Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 46
3.1 Findings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 46
3.2 Probable Cause . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47
4. Recommendation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 48
5. Appendix
A: Investigation and Public Hearing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 49

v Aircraft Accident Report
Figures
1. Interior configuration of the accident airplane. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
2. Cylinder differential compression check form.. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
3. Exterior of the upper outboard engine cowling. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
4. The condition in which the right engine No. 2 cylinder
retention system components were found. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28

vi Aircraft Accident Report
Abbreviations
A&P airframe and powerplant
AAIP Approved Aircraft Inspection Program
ARTCC air route traffic control center
ATP airline transport pilot
CFI certified flight instructor
CFR Code of Federal Regulations
CG center of gravity
CVR cockpit voice recorder
F Fahrenheit
FAA Federal Aviation Administration
FDR flight data recorder
FLL Fort Lauderdale/Hollywood International Airport
fpm feet per minute
FSDO Flight Standards District Office
Hg mercury
KIAS knots indicated airspeed
METAR meteorological aerodrome report
MYAT Treasure Cay Airport
MYGF Grand Bahamas International Airport
PFD personal flotation device
PIC pilot-in-command
PMI principal maintenance inspector
psi pounds per square inch
PTRS Program Tracking and Recording System
SB service bulletin
SJU Luis Munoz Marin International Airport
SRQ Sarasota/Bradenton International Airport
TBO time between overhaul
TCM Teledyne Continental Motors
TSO Technical Standard Order

vii Aircraft Accident Report
Executive Summary
On July 13, 2003, about 1530 eastern daylight time, Air Sunshine, Inc. (doing
business as Tropical Aviation Services, Inc.), flight 527, a Cessna 402C, N314AB, was
ditched in the Atlantic Ocean about 7.35 nautical miles west-northwest of Treasure Cay
Airport (MYAT), Treasure Cay, Great Abaco Island, Bahamas, following the in-flight
failure of the right engine. Four of the nine passengers sustained no injuries, three
passengers and the pilot sustained minor injuries, and one adult and one child passenger
died after they evacuated the airplane. The airplane sustained substantial damage. The
airplane was being operated under the provisions of 14 Code of Federal Regulations
Part 135 as a scheduled international passenger commuter flight from Fort
Lauderdale/Hollywood International Airport, Fort Lauderdale, Florida, to MYAT. Visual
meteorological conditions prevailed for the flight, which operated on a visual flight rules
flight plan.
The National Transportation Safety Board determines that the probable cause of
this accident was the in-flight failure of the right engine and the pilot’s failure to
adequately manage the airplane’s performance after the engine failed. The right engine
failure resulted from inadequate maintenance that was performed by Air Sunshine’s
maintenance personnel during undocumented maintenance. Contributing to the passenger
fatalities was the pilot’s failure to provide an emergency briefing after the right engine
failed.
The safety issues discussed in this report include maintenance record-keeping and
practices, pilot proficiency, Federal Aviation Administration (FAA) oversight, and
emergency briefings. A safety recommendation concerning emergency briefings is
addressed to the FAA.

this page intentionally left blank

1 Aircraft Accident Report
1. Factual Information
1.1 History of Flight
On July 13, 2003, about 1530 eastern daylight time,
1
Air Sunshine, Inc. (doing
business as Tropical Aviation Services, Inc.),
2
flight 527, a Cessna 402C, N314AB, was
ditched in the Atlantic Ocean about 7.35 nautical miles west-northwest of Treasure Cay
Airport (MYAT), Treasure Cay, Great Abaco Island, Bahamas, after the in-flight failure of
the right engine. Two of the nine passengers
3
sustained no injuries, five passengers and the
pilot sustained minor injuries, and one adult and one child passenger died after they
evacuated the airplane.
4
The airplane sustained substantial damage. The airplane was
being operated under the provisions of 14 Code of Federal Regulations (CFR) Part 135 as
a scheduled international passenger commuter flight from FLL to MYAT.
5
Visual
meteorological conditions prevailed for the flight, which operated on a visual flight rules
flight plan.
The accident pilot was scheduled to fly the accident airplane on a 2-day trip
sequence, which began about 0900 on July 12, 2003. The pilot flew five flights, each of
which lasted about 1 hour, on the first day of the trip sequence. The last flight was from
FLL to Sarasota/Bradenton International Airport (SRQ), Sarasota, Florida, and it arrived
at SRQ about 1930. All of the first day’s flights were uneventful, and the pilot reported no
engine- or airframe-related discrepancies for any of the flights.
On July 13, 2003, the pilot arrived at SRQ about 0830 for the second day of the
trip sequence. The pilot was scheduled to conduct five flights, each of which was to last
about 1 hour. The first flight departed SRQ about 0930 and arrived at FLL about 1030.
The second flight departed FLL about 1100 and arrived at MYAT about 1200. The third
1
Unless otherwise indicated, all times in this report are eastern daylight time. The airplane was not
equipped with a cockpit voice recorder (CVR) and was not required to be so equipped. Therefore, all times
referenced in this report are approximations, except for the takeoff time, which was determined by reference
to transcripts of voice recordings obtained from the Fort Lauderdale/Hollywood International Airport (FLL)
air traffic control tower and the Miami Automated International Flight Service Station.
2
Air Sunshine and Tropical Aviation Services are two separate companies owned and operated by the
same people.
3
Four of the nine passengers were children; one of the children was under 2 years of age and was
seated on an adult passenger’s lap during the flight.
4
The search for, and rescue of, the surviving airplane occupants (and recovery of the bodies of the two
other airplane occupants) is discussed in section 1.15.4.
5
Under the provisions of Annex 13 to the Convention on International Civil Aviation, the
investigation of an airplane crash is the responsibility of the state of occurrence (the state or territory in
which an accident or incident occurs, which in this case was the Bahamas). However, the state of occurrence
may delegate all or part of an investigation to another state by mutual arrangement or consent. At the request
of the Bahamian Government, the National Transportation Safety Board assumed full responsibility for the
investigation. The Bahamian Government designated an accredited representative to the investigation.

Factual Information 2 Aircraft Accident Report
flight departed MYAT about 1215 and arrived at FLL about 1330. All of the flights were
reported to be uneventful.
The pilot stated that, before departing on the fourth flight of the day, from FLL to
MYAT, he conducted a preflight inspection of the airplane, which included checking the
oil quantity. The accident flight was cleared for takeoff at 1427:11 and was estimated to
last about 1 hour 10 minutes.
During postaccident interviews, passengers stated that, before starting the engines,
the pilot briefed
6
them on the location of the personal flotation devices (PFD),
7
the exits,
and the safety briefing cards
8
and on the need to keep their lapbelts fastened during the
flight. One of the passengers who accompanied a child noted that the pilot’s briefing did
not include how to handle children during an emergency and added that the briefing was
“short and rushed.”
The pilot and adult passengers stated that the cruise portion of the flight was
uneventful, and the pilot stated that the engine instruments showed no indications of a
mechanical problem. The pilot indicated that the flight’s cruise altitude was about
7,500 feet and that the cruise speed was about 160 knots indicated airspeed (KIAS).
9
The pilot stated that, during the descent into MYAT, he maintained the same power
setting that he used during cruise flight, which was about 2,300 rpm and 27 inches of
mercury (Hg) manifold pressure. The pilot stated that, about 20 to 25 miles from MYAT
(about 45 to 50 minutes into the flight), while descending to about 3,500 feet, he heard a
bang and saw oil coming out of the right engine cowling.
10
The adult passenger in the copilot’s seat (the seat to the right of the pilot seat)
reported seeing a “stream of oil” coming from the right engine and stated that he notified
the pilot of his observation. Several of the other adult passengers reported seeing white
smoke coming from the right engine. These passengers stated that the smoke was followed
6
Title 14 CFR 135.117(a) requires pilots to brief passengers orally before departure.
Section 135.117(a) states that the predeparture briefing should include, in part, information on the use of
safety belts, the location of and instructions for opening the passenger entry door and emergency exits, and
the location of survival equipment.
7
The airplane was equipped with 10 PFDs that were sealed in plastic pouches. Eight of the PFDs were
stowed under the forward edge of each passenger seat. The PFDs for the pilot and copilot positions were
stowed outboard of each pilot seat. For more information, see section 1.15.3.
8
The safety briefing cards were contained in the stowage pockets located on the back of each seat.
9
The airplane was not equipped with a flight data recorder (FDR) and was not required to be so
equipped. Data from the Nassau Air Route Surveillance Radar (about 125 miles south of the accident
site) did not indicate any targets in the Bahamas airspace consistent with the reported route and altitude of
flight 527. Other aircraft were observed at an altitude of about 6,600 feet and above near Grand Bahamas
Island and at an altitude of about 5,100 feet and above near the ditching site. All flight altitudes and speeds
referenced in the report are based on the pilot’s recollections.
10
From June 12 to 14, 2003, Air Sunshine’s Director of Maintenance and an assistant mechanic
performed differential compression checks on the accident airplane’s right engine cylinders during the
airplane’s last recorded engine maintenance. For more information about these checks, see section 1.6.1.2.1.

Factual Information 3 Aircraft Accident Report
by a stream of oil and then the sound of a loud bang. They reported seeing parts falling
from the engine after they heard the loud bang.
The pilot stated that, after he heard the bang, he reduced power to the right engine.
The pilot indicated that, at the time of the event, the airplane’s airspeed was about 135 to
140 KIAS. He added that the airspeed for a normal descent should be about 140 knots.
The pilot stated that he then saw that the engine magnetos had penetrated through the
engine cowling and that the magnetos were hanging from wires. He added that he did not
see any other damage. He stated that he noticed that the right engine oil pressure
indication was decreasing rapidly. He added that the fuel selector was “in the green” (that
is, each engine was being provided fuel from its respective main fuel tank). He stated that
he attempted to feather
11
the right propeller and shut down the engine
12
but that the
propeller continued “wind-milling” (turning) slowly. The passenger in the copilot seat and
the adult passenger in the seat behind the copilot’s seat also reported that the pilot tried to
feather the right propeller but that it continued to turn after the engine failed.
13
The pilot stated that, after he attempted to shut down the right engine, he applied
full power to the left engine and tried to fly the airplane but that he could not maintain
altitude. He stated that he slowed the airplane to “blue line” (single-engine best climb rate)
airspeed, which is about 105 KIAS, and that, at that point, the airplane was at a descent
rate of about 200 to 300 feet per minute (fpm).
The pilot stated that he contacted Air Sunshine’s station manager at MYAT after
trying to shut down the engine. The station manager stated that the pilot told him that the
right engine had failed and that he was at an altitude of about 3,000 feet. The manager
added that the pilot asked him to contact the company’s Director of Operations at FLL,
which the manager did. Air Sunshine’s Director of Operations told the manager to ask the
pilot if the propeller on the failed engine was feathered, and the pilot responded that it
was. The Director of Operations then asked the manager to get the airplane’s distance
from the airport, altitude, and descent rate; the pilot responded that he was about 15 miles
from the airport
14
at an altitude of about 2,000 feet with a descent rate of about 200 fpm.
The Director of Operations instructed the manager to tell the pilot to “keep the good
engine at full power, bank to the good engine and to just stay calm and fly the plane.” The
pilot told the manager that he had already “done all of those things.”
11
Feathering means to rotate the propeller blades so that the blades are parallel to the line of flight to
reduce drag and prevent further damage to an engine that has been shut down.
12
The pilot stated that he did not follow Air Sunshine’s procedures for an in-flight engine failure
because he knew which engine had failed; therefore, he chose to immediately shut down the right engine. He
added that he did not follow the engine failure checklist because he was “too busy flying the airplane.” For
more information about Air Sunshine’s in-flight engine failure procedures, see section 1.17.1.1.
13
The pilot and both passengers reported that the right propeller continued turning until the airplane
contacted the water.
14
The airplane was equipped with a global positioning system, which the pilot used to determine the
airplane’s distance from the airport.

Factual Information 4 Aircraft Accident Report
The station manager stated that he then alerted local agencies about the emergency
and instructed another Air Sunshine pilot, who had just taken off from Marsh Harbor,
Bahamas, for FLL, to divert that flight toward flight 527 and follow the airplane until it
reached the airport. The Air Sunshine pilot transmitted a distress call for flight 527, which
the pilot of a nearby flight (Gulf flight 9267) heard and relayed to the Federal Aviation
Administration (FAA) Air Route Traffic Control Center (ARTCC), Miami, Florida.
The pilot stated that, after talking to the station manager, he slowed the airplane to
about 95 KIAS to try to maintain altitude. The pilot stated that, once he descended from
about 1,500 to 1,000 feet, he realized the airplane could not make it to the airport and that
he would have to ditch the airplane. The pilot stated that he ditched the airplane parallel to
the waves with the flaps retracted. He added that, at the time of the ditching, the winds
were about 15 knots, and the outside air temperature was about 80° to 90° Fahrenheit (F).
The passenger in the copilot seat stated that the pilot did a good job ditching the airplane.
He stated that he noticed a placard on the instrument panel with instructions for ditching,
which stated that the airspeed should be kept in the “blue zone,” and that the airspeed was
within this zone during the ditching. Adult passengers described the contact with the water
as “very hard.” They stated that the airplane landed “flat” and that it did not dive into the
water.
During postaccident interviews, the passengers stated that the pilot did not instruct
them to retrieve their PFDs or to assume a brace position before contact with the water.
The passengers stated that the only time the pilot addressed them after the right engine
failed and before the airplane contacted the water was to tell them to “calm down.”
The airplane was located at 26° 45.547' north latitude and 77° 31.642' west
longitude. The accident occurred during daylight hours.
1.2 Injuries to Persons
Injuries Flight Crew Cabin Crew Passengers Other Total
Fatal 00 202
Serious 00 000
Minor 10 506
None 00 202
Total 10 9010

Factual Information 5 Aircraft Accident Report
1.3 Damage to Airplane
The airplane sustained substantial damage.
1.4 Other Damage
No other damage was reported.
1.5 Personnel Information
1.5.1 The Pilot
The pilot, age 46, was hired by Air Sunshine in September 1995. He held an airline
transport pilot (ATP) certificate, which was issued March 7, 1998, with a multiengine land
rating. Additionally, he held a commercial pilot certificate with a single-engine land rating
and a certified flight instructor (CFI) certificate with single-engine, multiengine, and
instrument ratings. The pilot held an FAA first-class medical certificate, dated June 9,
2003, with no limitations.
According to the pilot, he began flight training at Aviation Training, Hayward,
California. The pilot reported that, before he began working for Air Sunshine, he worked as a
first officer on Embraer 110 airplanes for Payam Aviation Services, Tehran, Iran, for 2 years.
The pilot began working for Air Sunshine in September 1995, performing clerical
work for about 6 months before starting the company’s flight training. He served as first officer
on the company’s Embraer 110 for about 1 1/2 years, during which time he earned his ATP
certificate. In 1998, he upgraded to captain on the Cessna 402. He resigned from Air Sunshine
on September 29, 2002. From September 30 to November 11, 2002, the pilot received flight
training at Arrow Air, Inc., in Miami.
15
The pilot left Arrow Air because he could not
complete the training.
16
On November 23, 2002, the pilot was rehired by Air Sunshine.
Air Sunshine records indicated that the accident pilot had accumulated a total
flying time of about 8,000 hours, about 5,500 hours of which were as pilot-in-command
(PIC) and about 5,000 hours of which were in Cessna 402 airplanes. He had flown
about 251, 69, 13, and 6 hours in the last 90, 30, and 7 days, and 24 hours, respectively.
The pilot’s last PIC line check occurred on July 9, 2002; his last PIC proficiency check
occurred on January 14, 2003; and his last recurrent ground training occurred on June 14,
2003. A search of FAA records found no evidence of enforcement actions.
15
Arrow Air is a 14 CFR Part 121 supplemental all-cargo air carrier. During the time that the pilot was
in training, the company operated McDonnell Douglas DC-8 and Lockheed L-1011 airplanes.
16
A review of Arrow Air’s simulator training records for the pilot revealed that he had received a large
number of “unsatisfactory” grades. Further, the records indicated that the pilot needed to improve his
scanning and checklist skills, including response and organization.

Factual Information 6 Aircraft Accident Report
FAA records revealed that the pilot had been involved in an incident on June 12,
1999, in which the nose landing gear collapsed during landing at FLL. The pilot and
passengers were not injured, and the airplane sustained minor damage. The records also
revealed that the pilot was involved in an accident on March 16, 2000, in which a tire
failed during takeoff from FLL.
17
The pilot aborted the takeoff but was unable to keep the
airplane on the runway. The pilot and passengers were not injured, and the airplane
received substantial damage. Further, a review of the FAA’s Program Tracking and
Reporting System (PTRS) records revealed that, on September 13, 2000, the pilot failed a
ramp check because his airplane was found to have numerous discrepancies and his
passenger briefing was found to be inadequate.
As previously stated, the pilot was scheduled for a 2-day trip sequence on July 12
and 13, 2003. Between 0900 and 1700 on July 12th, the pilot flew five flights and
accumulated about 5 hours of flight time. All of the flights were conducted in the accident
airplane. The pilot stated that, after the last flight (FLL to SRQ), he ate, watched some
television, and went to bed between about 2230 and 2300.
The pilot stated that he awoke about 0730 on July 13th and arrived at SRQ
about 0830 to report for the second day of the trip sequence, which consisted of five
scheduled flights starting about 0930. Each flight was expected to last about 1 hour. The
pilot completed three of the scheduled flights before the accident flight occurred.
1.5.1.1 Flight Check History
Between April 1983 and February 1998, the pilot received the following notices of
disapproval from the FAA:
• In April and May 1983, the pilot received notices of disapproval because he
failed the entire flight test portion of the flight checks
18
he was receiving for
his private pilot certificate. On June 22, 1983, the pilot was rechecked
successfully, and he received his private pilot certificate.
• On October 30, 1985, the pilot received a notice of disapproval because he
failed the “holding” and the “recovery from an unusual attitudes” portions of
the flight check he was receiving for his instrument rating. On November 8,
1985, the pilot was rechecked successfully, and he received his instrument
rating.
• In December 1987 and February 1988, the pilot received notices of disapproval
because he failed the entire flight test portion of the flight checks he was
receiving for his CFI certificate. On March 17, 1988, the pilot was rechecked
successfully, and he received his CFI certificate.
17
A description of this accident, MIA00LA109, can be found on the Safety Board’s Web site at
<http://www.ntsb.gov>.
18
If a pilot receives a notice of disapproval for a flight check, the pilot can be required to be rechecked
on the complete flight check or on designated portions of the flight check.

Factual Information 7 Aircraft Accident Report
• In July 1988 and May 1989, the pilot received notices of disapproval because
he failed the entire flight test portion of the flight checks he was receiving for
his CFI instrument rating. In August 1989, he received another notice of
disapproval because he failed the “holding” portion of the flight check and did
not complete three other portions of the check. On December 8, 1989, the pilot
was rechecked successfully, and he received his CFI instrument rating.
• In February 1998, the pilot received a notice of disapproval because he failed
the “nondirectional beacon approach” portion of the flight check he was
receiving for his ATP certificate. On March 7, 1998, the pilot was rechecked
successfully, and he received his ATP certificate.
1.5.2 The Director of Maintenance
Air Sunshine’s Director of Maintenance was hired by the company in March 1997
as a mechanic; seven months later, he was promoted to Director of Maintenance.
On October 28, 1989, the Director of Maintenance applied for his airframe and
powerplant (A&P) certificate based on work experience
19
he obtained while working as an
assistant mechanic from March 1985 to the date of the application. On October 24, 1990, the
director took the oral and practical examinations required by 14 CFR 65.79.
20
He passed all
of the oral examinations; however, he failed the following portions of the practical exam:
Section I, General – Airframe and Powerplant, subsections (A) weight and balance and
(B) completion of FAA Form 337; and Section IV, Powerplant Theory and Maintenance,
subsection (A) troubleshooting of turbine engines. The director received additional training
in these areas and retook the practical exam on October 30, 1990, at which time he received
his A&P certificate. A search of FAA records found no evidence of enforcement actions.
The Director of Maintenance reported that, from March 1985 to August 1990, he
worked as an assistant mechanic on Cessna 402 airplanes at Airways International, a
14 CFR Part 135 on-demand charter operator in Miami. From January 1988 to March 1989,
he also worked part-time as an assistant mechanic on McDonnell Douglas DC-10 and
Lockheed L-1011 airplanes at Eastern Airlines in Miami. From mid-1990 to mid-1996, he
worked as a mechanic at Airways International. From August 1996 to March 1997, he
worked as a mechanic on Cessna 402, 210, and 206; Piper Cherokee; Britten-Norman
Islander; and Beechcraft 55 and 58 airplanes at Flightline of America, Pembroke Pines,
Florida.
19
According to 14 CFR 65.77, “Experience Requirements,” “each applicant [for a mechanic certificate or
rating]…must present either an appropriate graduation certificate or certificate of completion from a certificated
aviation maintenance technician school or documentary evidence of…at least 30 months of practical experience
concurrently performing the duties appropriate to both the airframe and powerplant ratings.”
20
According to 14 CFR 65.79, “Skill Requirements,” “each applicant [for a mechanic certificate or
rating]…must pass an oral and a practical test on the rating he seeks. The tests cover the applicant’s basic skill in
performing practical projects on the subjects covered by the written test for that rating. An applicant for a
powerplant rating must show his ability to make satisfactory minor repairs to, and minor alterations of,
propellers.”

Factual Information 8 Aircraft Accident Report
1.5.3 The Assistant Mechanic
Air Sunshine’s assistant mechanic was hired by the company on June 6, 2000, to
work in San Juan, Puerto Rico. In March 2003, he transferred to the company’s facility at
FLL. The assistant mechanic did not have an A&P certificate.
On March 31, 2003, the Director of Maintenance signed off a Certificate of
Training for the assistant mechanic, indicating that he had completed 30 hours of basic
indoctrination training. On April 30, 2003, the director signed off a Certificate of Training
for the assistant mechanic, indicating that he had completed 60 hours of aircraft subjects
training. On June 30, 2003, the director signed off a Certificate of Training for the
assistant mechanic, indicating that he had completed 200 hours of on-the-job training for
the “entire aircraft, airframe, engine, propeller, accessories, etc.”
1.6 Airplane Information
The accident airplane, serial number 402C0413, was manufactured by Cessna
Aircraft Company on November 24, 1980. The airplane was operated by several airlines
21
before being sold to Tropical International Airlines, Inc.,
22
on August 29, 1997. From
mid-1997 to late 2000, the airplane was kept at the company’s maintenance facility at FLL.
Air Sunshine’s President stated that, during this time, extensive maintenance was being
performed on the airplane, including left and right engines and propellers replacement, sheet
metal repair, corrosion treatment, and landing gear repair, to make it airworthy.
Tropical International Airlines leased the airplane to Air Sunshine on November 1,
2000.
23
The airplane was inspected in accordance with Air Sunshine’s FAA Approved
Aircraft Inspection Program (AAIP) on November 20, 2000, and found to be airworthy.
24
The airplane was added to the company’s operations specifications on December 6, 2000.
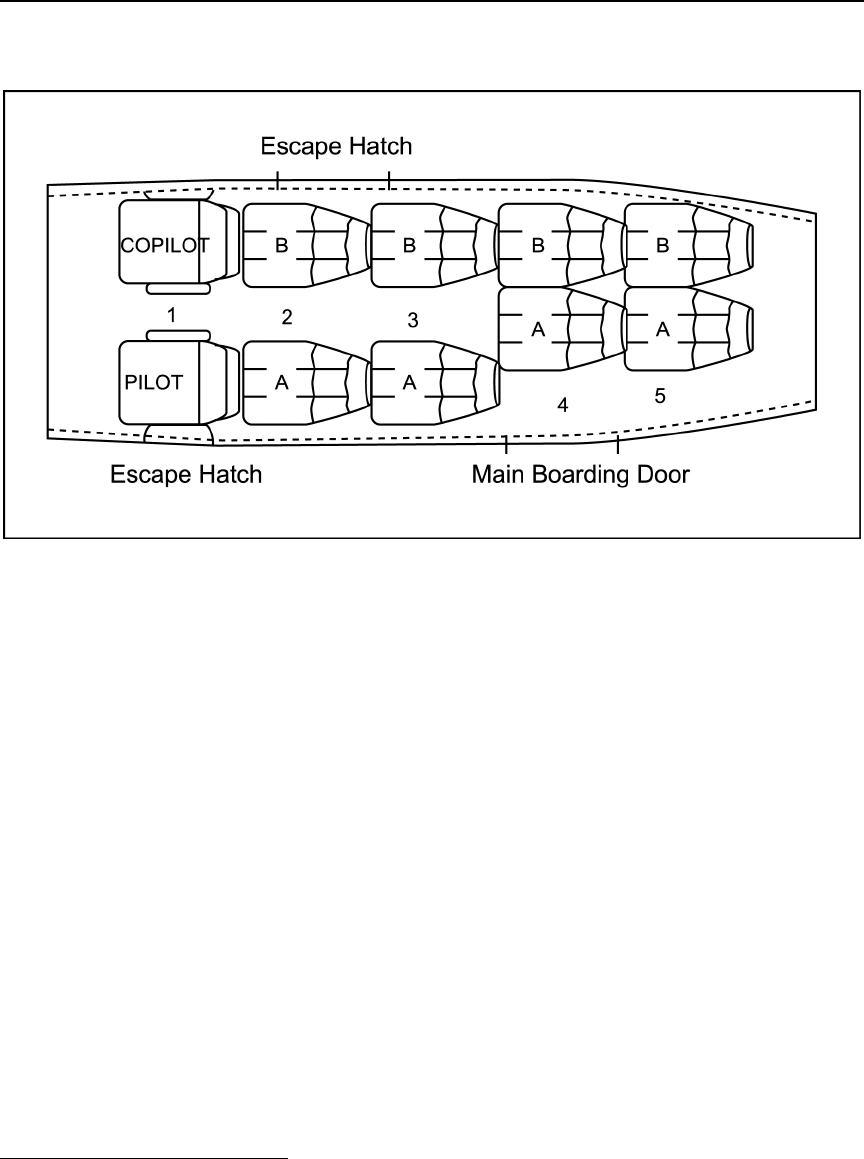
The airplane was configured with a pilot seat (left side), a copilot seat (right side),
and eight passenger seats. (See figure 1.) The airplane was equipped with a window
escape hatch adjacent to the pilot seat (1A); an emergency escape hatch adjacent to seats 2B
and 3B; and a two-section outward opening airstair door (main cabin door) adjacent to
seats 4A and 5A, the lower portion of which was equipped with stairs. The pilot and
copilot seats were equipped with lapbelts and single-strap shoulder harnesses, and the
passenger seats were equipped with lapbelts.
21
On March 1, 1992, the airplane was involved in a nose landing gear collapse while being operated by
Airways International. For more information about this accident, MIA92IA090, see the Safety Board’s Web
site at <http://www.ntsb.gov>.
22
Tropical International Airlines was owned and operated by the same people who own and operate Air
Sunshine.
23
The lease agreement stated that Air Sunshine would be responsible for all expenses, including
maintenance.
24
For more information about Air Sunshine’s AAIP, see section 1.6.1.1
Factual Information 9 Aircraft Accident Report
According to the load manifest form for the accident flight, the airplane’s takeoff
weight was about 6,644 pounds, including 890 pounds of passenger weight,
25
350 pounds
of baggage weight, and 800 pounds of fuel weight. The airplane’s takeoff center of gravity
(CG) was 154.61 inches aft of the reference datum. After the airplane was retrieved from
the water,
26
the baggage was removed from the airplane, dried, and weighed. The baggage
weighed 440.85 pounds, 90 pounds more than the amount that was entered on the load
manifest form. After applying the additional 90 pounds, the weight and CG were still
within acceptable limits.
27
1.6.1 Engines and Propellers
The airplane was equipped with two Teledyne Continental Motors (TCM)
TSIO-520-VB reciprocating engines. These engines are turbo-charged and fuel-injected
with six horizontally opposed air-cooled cylinders. The engines are rated for 325 horsepower
at a power setting of 2,700 rpm with 39 inches Hg manifold pressure up to an altitude of
12,000 feet.
Figure 1. Interior configuration of the accident airplane.
25
Actual passenger weights were used to calculate the total passenger weight.
26
The airplane was retrieved from the water on August 3, 2003. The retrieval was delayed because of
choppy waters.
27
According to the Cessna 402C Pilot Operating Handbook, the airplane’s maximum gross takeoff
weight is 7,210 pounds, and the maximum gross landing weight is 6,850 pounds. The maximum forward CG
for flight 527 was 151.2 inches aft of the reference datum, and the maximum aft CG for the flight was
160.7 inches.

Factual Information 10 Aircraft Accident Report
The engine cylinders incorporate an overhead inclined valve design. The cylinders
have updraft intake inlets and downdraft exhaust outlets mounted to the underside of the
cylinder heads. Each of the six cylinders is attached to the engine case by a series of
threaded studs, through bolts, and nuts. Six 7/16-inch, 20 threads-per-inch studs are
threaded into the case half for exclusive use at each cylinder location and are held down
by 6-point nuts. Additional studs are positioned between the cylinders and are shared by
adjacent cylinders. Two 1/2-inch through bolts, which are located at the engine crankshaft
main bearing positions, are either shared by opposed cylinders or the opposite crankcase
half and are held down by 12-point nuts.
The right engine, serial number 529092, and the left engine, serial
number 811069-R, were manufactured by TCM on February 1, 1991, and January 1, 1997,
respectively. Airmark Overhaul, Inc., in Fort Lauderdale
28
overhauled the right and left
engines on December 14 and December 21, 1999, respectively.
29
At the time of overhaul,
the right and left engines had times since new of 3,582.6 flight hours and 2,400.0 flight
hours, respectively. The right and left engines were installed on the accident airplane on
October 10 and 7, 2000, respectively. The last routine engine maintenance, which included
changing the oil, inspecting the oil filter, looking for leaks, and performing a ground
run-up, was conducted on July 8, 2003, and the time since overhaul for both engines at
that time was 2,246.5 flight hours. At the time of the accident, both engines had a time
since overhaul of 2,270.6 flight hours.
30
The airplane was equipped with two McCauley Propeller Systems 3AF32C505-C
three-bladed, dual-acting, constant-speed propellers. The blades are counterweighted to
help move them toward higher blade angles (that is, toward feather) during operation.
A feather spring inside the propeller moves the blades to the high-pitch (feather) stops.
A centrifugal start-lock system, which uses spring-loaded pins that engage the piston as
the propeller speed drops below approximately 600 rpm, prevents the blades from
traveling all the way to feather during normal engine shutdowns, which reduces the load
on the engine during subsequent engine starts.
1.6.1.1 Air Sunshine’s Approved Aircraft Inspection Program
As a 14 CFR Part 135 operator, Air Sunshine had the option to operate either under
the manufacturers’ maintenance inspection programs or to develop and receive FAA
approval for its own maintenance inspection program. From 1982 to 1992, Air Sunshine
operated under the manufacturers’ (Cessna, TCM, and McCauley Propeller) maintenance
inspection programs.
In early 1992, under the oversight of the Fort Lauderdale Flight Standards District
Office (FSDO), Air Sunshine developed and received approval for its own inspection
28
Airmark Overhaul is an FAA-approved maintenance vendor for Air Sunshine.
29
Maintenance records were not available from the dates of manufacture of the right and left engines to
the dates of the overhauls.
30
For information about TCM’s recommended overhaul limit and Air Sunshine’s overhaul interval, see
section 1.6.1.3.

Factual Information 11 Aircraft Accident Report
program. The company’s initial AAIP was a 3-phase, 60-hour inspection program.
A different phase was performed every 60 hours of operation along with a routine
servicing check, which included an engine oil change, a ground run-up, and a visual
inspection of the airframe. Phases 1 through 3 comprised one full cycle, and an airplane
had to complete one full cycle (that is, the entire aircraft had to have been inspected) every
180 hours of operation.
On November 4, 2002, Air Sunshine submitted revision No. 10, which proposed to
change the company’s AAIP to a 6-phase, 60-hour inspection program, to the FAA for
approval. On January 9, 2003, the FAA approved the change,
31
and the 6-phase, 60-hour
inspection program was in effect at the time of the accident. Each of the six phase
inspections focused on one major airplane section. Phase 1 covered the powerplants,
including a focused engine inspection and a differential compression check of the engine
cylinders; phase 2 covered the wings; phase 3 covered the cabin; phase 4 covered the
landing gear; phase 5 covered the fuselage; and phase 6 covered the empennage. Phases 1
through 6 comprised one full cycle, and an airplane had to complete one full cycle every
360 hours of operation. The last phase 1 inspection was performed at FLL from June 12
to 14, 2003. During this inspection, each engine was determined to have a time since
overhaul of 2,187 flight hours.
1.6.1.2 Differential Compression Checks
TCM Service Bulletin (SB) 03-3 states that differential compression checks are
conducted to identify leaks in the engine cylinders and the sources of any leaks that were
found and that leaks can be caused by abnormal or excessive wear inside the engine
cylinders or their components, problems with the valves or valve seats, and cracks in the
cylinders. The SB also states that compression checks should be conducted “at each
100 hour interval, annual inspection or when cylinder problems are suspected.”
32
According to SB 03-3, before conducting the differential compression check, the
acceptable pressure leakage limit for the equipment being used and the atmospheric
conditions at the time that the check is conducted need to be established. SB 03-3 contains the
following instructions on how to perform differential compression checks on all of its engines:
• remove the most accessible spark plug from each of the six cylinders on each
engine;
• turn the engine crankshaft by hand in the direction of rotation until the piston is
coming up on top dead center at the end of the compression stroke;
31
In early 1998, Air Sunshine requested that its operating certificate be transferred from the FAA’s Fort
Lauderdale FSDO to its San Juan FSDO. The FAA granted the request, and the transfer took place on June 2,
1998. The company’s operating certificate was under the jurisdiction of the San Juan FSDO when the
company applied and was approved to change its AAIP. For more information about FAA oversight of Air
Sunshine, see section 1.17.2.
32
For information about the postaccident change to the differential compression check interval and
other changes to Air Sunshine’s AAIP, see section 1.17.2.5.

Factual Information 12 Aircraft Accident Report
• install a cylinder adapter in the spark plug hole and connect a differential
pressure tester to the cylinder adapter and slowly open the cylinder pressure
valve and pressurize the cylinder to 20 pounds per square inch (psi);
• continue to rotate the engine in the direction of rotation, against the pressure,
until the piston reaches top dead center (that is, with the piston at the end of the
compression stroke and the beginning of the power stroke);
• open the cylinder pressure valve completely;
• move the propeller slightly back and forth with a rocking motion while
directing regulated pressure of 80 psi into the cylinder and adjust regulator as
necessary to maintain a pressure gauge reading of 80 psi; and
• record the pressure indication on the cylinder pressure gauge.
The difference between the pressure directed into the cylinder (80 psi) and the
cylinder pressure shown on the regulator pressure gauge is the amount of leakage through
the cylinder. Any cylinder pressure level greater than that established as the acceptable
pressure leakage limit indicates an acceptable operating condition for a reciprocating
engine. The SB recommends that, if the cylinder pressure levels are less than the
acceptable pressure leakage limit, cylinder borescope inspections should be conducted.
1.6.1.2.1 June 12 to 14, 2003, Differential Compression Checks
As noted previously, the last differential compression checks performed on the
accident airplane’s engines occurred from June 12 to 14, 2003, as part of the airplane’s last
phase 1 inspection. According to the Director of Maintenance, he performed the checks on
the left engine while the assistant mechanic watched and then recorded the readings in the
inspection record. The cylinder differential compression check form
33
in Air Sunshine’s
Maintenance Manual contains the following: “CAUTION - It is recommended that
someone hold the propeller during this check to prevent possible rotation.” (See figure 2.)
The Director of Maintenance stated that, after completing the checks on the left
engine, he asked the assistant mechanic if he felt capable of performing the checks on the
right engine without supervision. The director stated that the assistant replied that he could
perform the checks; as a result, the director left the assistant to perform the checks by
himself without supervision. According to the director, he asked the assistant mechanic to
record the compression check readings for the right engine on a sheet of paper so that he
could review them before making the entries in the cylinder differential compression check
form in the inspection records; however, the assistant mechanic recorded the readings
directly in the inspection record. Figure 2 also shows the compression check readings (in
psi) recorded in the inspection record by the assistant mechanic for both engines.
Accounting for the check equipment used at the time that the checks were performed, the
Safety Board determined that the acceptable pressure leakage limit was 54 psi.
33
The cylinder differential compression check form is part of the company’s AAIP phase 1 inspection
package.

Factual Information 13 Aircraft Accident Report
Note: According to the assistant mechanic and the Director of Maintenance, the number recorded for right engine cylinder
No. 3 was “55.” (Safety Board investigators who reviewed the document noted that the number could be either “55” or “25.”)
The assistant mechanic’s signature and A&P certificate number have been redacted.
Figure 2. Cylinder differential compression check form.

Factual Information 14 Aircraft Accident Report
During postaccident interviews, the assistant mechanic stated that he had never
performed a differential compression check before conducting the checks on the accident
airplane’s right engine. The assistant stated that his normal duties included changing oil,
tires, cables, and spark plugs and cleaning the airplane. When a Safety Board investigator
asked the assistant how to perform the compression check, he stated only that the spark
plugs had to be removed from the cylinders and that the piston had to be at top dead center
on its compression stroke.
The Director of Maintenance stated that, as he was reviewing and signing off on
the day’s maintenance work, he noticed that two of the readings obtained from the
compression checks of the right engine (0 psi for the No. 2 cylinder and 20 psi for the
No. 4 cylinder)
34
were “highly questionable.” The director stated that he asked the
assistant mechanic if he had been careful to get the piston at top dead center on its
compression stroke on each cylinder when he performed the check. The director indicated
that, although the assistant stated that he had been careful to get the piston into its required
position, he appeared uncertain when asked specifically about the two questionable
cylinder readings. The director told the assistant mechanic that the compression checks on
the right engine cylinders would have to be repeated.
According to the Director of Maintenance, after he repeated the checks on the right
engine, all of the cylinder’s compression readings were in the 70-psi range, including the
two cylinders with low readings from the first compression checks. The director stated
that, when he did the rechecks, he was careful to get the piston at top dead center on its
compression stroke and hold the propeller while adding the pressure. He added that, if the
compression level readings had remained low, he would have grounded the airplane. The
director stated that he had the assistant mechanic observe the checks and record the
readings on a sheet of paper. The assistant mechanic stated that he gave the sheet of paper
to the director but that he did not see what the director did with the paper. The director
stated that he recorded the corrected readings on a new cylinder differential compression
check form; however, company personnel did not locate the corrected form. The director
stated that he did not conduct cylinder borescope inspections on cylinder Nos. 2 and 4
because the repeated compression checks yielded readings that were within acceptable
limits.
The Director of Maintenance stated that the company had removed and replaced
an engine cylinder assembly about five or six times in the last 3 years. The director stated
that, before applying torque to the cylinder studs, maintenance personnel coated the studs
with an aluminum-copper-graphite, lithium-based antiseize compound manufactured by
Permatex. TCM SB 96-7B specifies that clean 50-weight aviation-grade engine oil should
be applied to the studs and through bolts before applying torque. Permatex does not
recommend using antiseize compound in high-vibratory environments because such use
could contribute to the loss of torque.
34
The Director of Maintenance stated that he would consider any reading below 58 psi to be too low
and that low readings would require that the cylinder be rechecked. The director did not mention that the
reading recorded for cylinder No. 3 was too low, even though he stated that it was “55.”

Factual Information 15 Aircraft Accident Report
1.6.1.3 Time Between Overhauls
TCM Service Information Letter 98-9A recommends that TSIO-520-VB engines
have a time between overhaul (TBO) of 1,600 hours. Air Sunshine began operating its
airplanes equipped with TSIO-520-VB engines in accordance with this recommendation.
After Air Sunshine’s inspection program received FAA approval in early 1992,
35
the
company applied to the Fort Lauderdale FSDO for a 200-hour extension of its TBO per
the procedures outlined in FAA Order 8300.10, Airworthiness Inspector’s Handbook.
36
The FAA principal maintenance inspector (PMI) for Air Sunshine granted its request and
allowed the company to increase its TBO by 200 hours. From late 1992 to late 1995, Air
Sunshine applied for four additional TBO extensions (of 200 hours, 200 hours, 100 hours,
and 100 hours) for a total TBO extension of 800 hours. The FAA granted approval for all
of the requested extensions, which resulted in a TBO of 2,400 hours.
According to FAA Order 8300.10, approval of TBO extensions is granted based on
“satisfactory service experience and/or a teardown examination of at least one exhibit
engine.” Neither the FAA nor Air Sunshine had retained the paperwork that related to the
five requests for, and approvals of, the extensions of the company’s TBO for longer than
the 2 years required by the FAA. However, Air Sunshine provided the Safety Board with
four teardown reports prepared by Airmark Overhaul (which were submitted as support
for the first four TBO extension requests) and one report prepared by TCM (which was
submitted as support for the last request). These reports were dated July 16, 1992;
November 17, 1992; March 20, 1994; January 20, 1995; and October 9, 1995. All of the
teardowns conducted by Airmark and TCM were of TCM-rebuilt engines.
After Air Sunshine received approval for the last 100-hour TBO extension, the
company petitioned the Fort Lauderdale FSDO to change the company’s operations
specifications to reflect the 2,400-hour TBO, and the Fort Lauderdale FSDO granted the
request under the condition that the company’s airplane engines be rebuilt by TCM. In late
August/early September 1999, after Air Sunshine transferred its operations certificate to
the San Juan FSDO, the company petitioned the San Juan FSDO to remove from the
company’s operations specifications the requirement that TCM rebuilt engines must be
used.
In a letter dated September 9, 1999, the FAA PMI for Air Sunshine stated that he
would grant the company’s request provided it (1) monitored the performance of newly
overhauled engines and reported any abnormal conditions to the San Juan FSDO,
37
(2) used
35
Air Sunshine was required to have its own AAIP to receive FAA approval for TBO extensions.
36
FAA Order 8300.10 indicates that TBO extensions for reciprocating engines can be granted in
increments of up to 200 hours.
37
A review of Air Sunshine and FAA records revealed that the company made no reports to the FAA
between the date of this letter and the date of the accident in which the company reported any abnormal
conditions of its overhauled engines.

Factual Information 16 Aircraft Accident Report
the approved overhaul facilities listed in its Maintenance Manual vendor list,
38
and
(3) established standards for parts to be used during the overhaul process. The PMI added
that, if the engines did not perform satisfactorily, the company’s operations specifications
would be amended back to the original TBO of 1,600 flight hours.
39
1.7 Meteorological Information
The closest airport to the location of the airplane wreckage was Grand Bahamas
International Airport (MYGF), Freeport, Bahamas, which was about 63.9 nautical miles
from where the airplane was located. MYGF does not have an automated weather system.
Weather observations are made by an on-site weather observer and are recorded in
coordinated universal time. Eastern daylight time is 4 hours behind coordinated universal
time.
The 1900 meteorological aerodrome report (METAR) (1500 local time, which was
about 30 minutes before the ditching) indicated that winds were 160° at 8 knots, visibility
was 10 nautical miles, clouds were broken at 2,000 feet, the temperature was 88.5° F, the
dew point was 74.1° F, and the altimeter setting was 30.09 inches of Hg.
The 2000 METAR (1600 local time, which was about 30 minutes after the
ditching) indicated that winds were 140° at 10 knots, visibility was 10 nautical miles, a
few clouds were at 1,500 feet and were scattered at 2,000 feet, the temperature was 88.5° F,
the dew point was 74.1° F, and the altimeter setting was 30.08 inches of Hg.
1.8 Aids to Navigation
The distance measuring equipment on the MYAT VOR
40
had been inoperative for
several years.
1.9 Communications
No communication problems were reported.
1.10 Airport Information
MYAT was the destination airport for flight 527. The airplane was ditched about
7.35 nautical miles west-northwest of the airport.
38
After its operations specifications were amended, Air Sunshine started using Airmark Overhaul, a
company on the FAA-approved vendor list, to overhaul its engines.
39
For information about postaccident changes to Air Sunshine’s operations specifications, see
section 1.17.2.5.
40
VOR stands for very high frequency omnidirectional range.

Factual Information 17 Aircraft Accident Report
1.11 Flight Recorders
The accident airplane was not equipped with either a CVR or an FDR and was not
required to be so equipped.
1.12 Wreckage and Impact Information
1.12.1 General
The airplane was submerged in water for about 3 weeks after the accident.
Underwater photographs taken before the airplane was recovered from the water showed
that the window escape hatch adjacent to the pilot seat (1A) was open. The emergency
escape hatch adjacent to seats 2B and 3B was found closed. The top and bottom portions
of the main cabin door adjacent to seats 4A and 5A were found open.
Impact damage was noted on the lower fuselage skin from the wing main spar
forward, and damage was noted on the nose cone. The landing gear was found retracted.
All of the airplane’s major components,
41
except for the left aileron and the
outboard section of the right elevator and balance weight, were recovered attached to the
airplane. The separated sections were not recovered. The rudder trim tab actuator was
found positioned between 5° and 10° trailing edge tab right; the elevator trim tab actuator
was found positioned at 15° trailing edge tab down. The left flap was found extended
about 15°, and the cowl flap was nearly closed. The right flap was found extended about 15°,
and the cowl flap was open. An oil sheen was noted on the exterior surface of the right
engine upper cowling, from the louvers aft to the trailing edge of the wing; on the interior
surface of the upper cowling; and on the upper and lower exterior surfaces of the
horizontal stabilizer.
The left fuel selector valve handle in the cockpit was found positioned to the left
main fuel tank; the right fuel selector valve handle was missing; therefore, its position
could not be determined. The emergency crossfeed/shutoff valve handle was found
positioned to the crossfeed position. The left and right auxiliary fuel pump switches were
found in the off position. The left and right cowl flap controls were found out (closed) and
in (open), respectively. Both the flap selector and flap position indicator were found at
about 15° flaps extended,
42
and the landing gear selector handle was found in the retracted
position. The elevator trim indicator was found positioned to full nose up. The aileron trim
indicator was found positioned slight left wing down. The rudder trim indicator was found
positioned nose left.
41
A major component is necessary for an airplane to sustain flight.
42
During postaccident interviews, the pilot stated that he did not extend the flaps during the flight. The
pilot stated that he would normally extend the flaps when he was about 3 miles from an airport. When he
was asked how the flaps became extended to 15°, the pilot replied that after the ditching, some of the
passengers crawled over him and that one of them might have hit the switch that extended the flaps. He
stated that the flaps were extended electrically and that he had left the power on after the ditching.

Factual Information 18 Aircraft Accident Report
All seats were found attached to the floor and were undamaged. All lapbelts were
present and were found to operate normally. The seatback stowage pockets for seats 2A
and 2B did not contain safety briefing cards;
43
all of the other stowage pockets contained
briefing cards.
Six packaged PFDs were found in the airplane. One PFD was found forward of the
pilot seat, and one PFD was found forward of the copilot seat. The remaining four PFDs
were found in their stowage areas (under seats 2A, 2B, 3A, and 5A). The PFDs were
brought to the Safety Board’s headquarters in Washington, D.C., and were examined on
August 28, 2003. The sealed plastic pouches were opened, and the PFDs were inflated by
pulling the inflation rings. All of the PFDs were undamaged and were found to operate
normally. Inspection records found inside the plastic pouches containing the PFDs
indicated that they had been inspected within the past 5 years, in accordance with Federal
regulations.
1.12.2 Engines and Propellers
The left engine was attached to the airframe, and the propeller was attached to the
engine. The outboard lower engine cowling had separated and was not located. The left
engine was removed and examined, under Safety Board supervision, at TCM’s facility. All
six cylinders and their valves were intact. No evidence of preexisting damage was found.
The left propeller was removed and examined, under Safety Board supervision, at
McCauley Propellers’ facility. The left propeller hub was intact and undamaged, and all
three blades were installed in the hub. Examination of the left propeller revealed no
evidence of preimpact damage. The feather-stop mechanism was attached and
undamaged, and the start-lock mechanism
44
was intact and undamaged.
The right engine was attached to the airframe in its normal position, and the
propeller was attached to the engine. Damage was noted on the leading edge skin from the
engine outboard to the wing tip; the leading edge skin from the engine nacelle inboard of
the wing root was crushed up and aft. The lower inboard engine cowling was separated
and was not recovered; the lower outboard engine cowling was in place.
The right engine No. 2 (inboard aft) cylinder was found separated from the engine
crankcase, exposing a portion of the crankshaft, and held onto the engine by the exhaust
pipe tubing and by an electrical cable that was secured to the cylinder assembly by an adel
clamp. The two magnetos were found protruding through the upper outboard engine
cowling but remained attached to the engine by ignition leads. (See figure 3.) Two 6-point
flanged nuts, one 12-point flanged nut with a fractured threaded piece, and a nonfractured
connecting rod were recovered from the engine compartment area. Piston ring pieces were
found in the partially separated No. 2 cylinder assembly.
43
The stowage pockets on these seatbacks held the briefing cards for use by the passengers in seats 3A
and 3B. For more information about the airplane’s interior configuration, see section 1.6.
44
As noted previously, the start-lock mechanism is a system designed to prevent the propeller from
traveling all the way to feather during normal engine shutdowns.

Factual Information 19 Aircraft Accident Report
The right engine was removed and examined, under Safety Board supervision, at
TCM’s facility. After engine disassembly at TCM, some of the right engine components
were brought to the Safety Board’s Materials Laboratory in Washington, D.C., for further
examination. For additional information about the metallurgical inspections of the right
engine components, see section 1.16.3.
The right propeller was removed and examined, under Safety Board supervision,
at McCauley Propeller’s facility. The right propeller hub was intact and undamaged, and
all three blades were intact and installed in the hub and appeared to be in the feathered
position. The blade angles were measured as follows: blade No. 1 was 82.2°, blade No. 2
was 82.4°, and blade No. 3 was 82.3°. The feather angle for this propeller is 82.2°
(+/-0.3°). All of the blade counterweights were present and in place. The propeller piston
was undamaged, and the centrifugal weights and springs were in place. The piston rod and
feathering spring were intact, in place, and undamaged. The feather-stop and start-lock
mechanisms were intact and undamaged.
Figure 3. Exterior of the upper outboard engine cowling.

Factual Information 20 Aircraft Accident Report
1.13 Medical and Pathological Information
Fluid specimens obtained from the pilot were sent to the Royal Bahamas Police
Force’s Forensic Science Laboratory for toxicological analysis. The fluid specimens tested
negative for alcohol and drugs.
45
According to the Rand Memorial Hospital (Freeport, Grand Bahamas) autopsy
report, the cause of death for the deceased 4-year-old child was “drowning secondary to
plane crash.” According to the Princess Margaret Hospital (Freeport, Grand Bahamas)
pathology report, the deceased adult passenger had injuries “consistent with the history of
plane crash accident.” Further, the report stated that the deceased adult passenger had a
cerebral contusion and rib fractures. The report also stated that a “section of both lungs
showed edema and congestion.”
1.14 Fire
No evidence of an in-flight fire was found, and the accident did not result in a
postcrash fire.
1.15 Survival Aspects
1.15.1 General
The pilot reported that he was not wearing his shoulder harness when the airplane
contacted the water and that he hit his head on the instrument panel during the ditching.
46
During postaccident interviews, one passenger stated that the pilot “did not appear to have
much clarity and was not particularly coherent” after the ditching. Another passenger
stated that he “took charge of the situation because the pilot was incoherent in the water.”
The passenger also stated that the pilot “did not look like he could swim” and that he had
to give the pilot his PFD.
The passenger in the copilot seat reported a bump on his head and a cut on his leg.
The passenger stated that he was not wearing his shoulder harness during the ditching
because the pilot had not informed him before the flight departed that his seat was so
equipped. The passengers in seats 2A and 2B reported bruises on their hips from the
lapbelts. The passenger in seat 3B reported a contusion on her forehead.
After the airplane contacted the water, the pilot opened the pilot-side window
hatch. The pilot, four adult passengers (from the copilot seat and seats 2A, 2B, and 3B),
45
The drugs tested in the postaccident analysis included benzoylecgonine, barbiturates,
benzodiazapines, and opiates.
46
Title 14 CFR 91.105(b) requires that required flight crewmembers of a U.S.-registered civil aircraft
keep their shoulder harnesses fastened while at their assigned duty stations during takeoff and landing.

Factual Information 21 Aircraft Accident Report
and one child (who had been sitting on the passenger in seat 3B’s lap) evacuated the
airplane through the pilot-side window escape hatch. One adult and three children (from
seats 4A, 4B, 5A, and 5B) evacuated the airplane through the main cabin door.
1.15.2 Emergency Briefings
Air Sunshine’s FAA-approved General Operations Manual, Section 4, “Emergency
Procedures,” contains the following guidance to pilots on briefing passengers before a
ditching:
• review the emergency ditching evacuation procedures with the passengers;
• instruct passengers to don life vests at that time, without inflating them in the
airplane;
• review the operation of the inflation ring and the manual/oral blow-up tubes;
and
• instruct passengers to inflate their life vests once they are outside of the aircraft.
As noted previously, passengers reported that the pilot did not tell them to retrieve
and don their PFDs before the airplane contacted the water. They stated that the only time
he addressed the passengers after the right engine failed and before the airplane contacted
the water was to tell them to “calm down.”
As the result of a postaccident focused inspection of Air Sunshine (conducted from
July 22 to August 29, 2003), the FAA instructed the company to amend its emergency
ditching procedures.
47
The amended procedures contain the following guidance to pilots
on briefing passengers before a ditching:
• instruct all passengers to don life vests as soon as any emergency occurs during
overwater operation;
• instruct passengers to familiarize themselves with emergency evacuation
procedures, including special evacuation procedures for those passengers who
are assisting others, such as children and handicapped individuals;
• review ditching procedures before ditching, including instructing passengers to
partially inflate their life vests through the use of the blow-up tubes; and
• instruct passengers that, only once they have gotten outside the airplane, they
should fully inflate their life vests by pulling the inflation ring.
1.15.3 Personal Flotation Devices
Title 14 CFR Part 135 requires specific emergency equipment, including approved
life preservers and rafts, a survival kit, and an emergency locator transmitter, to be
47
For more information about the FAA’s postaccident focused inspection of Air Sunshine, see
section 1.17.2.4.

Factual Information 22 Aircraft Accident Report
installed on airplanes that conduct extended overwater operations (that is, operate flights
over water at a horizontal distance greater than 50 nautical miles from the nearest
shoreline). Because Air Sunshine flight 527 did not qualify as an extended overwater
flight, the airplane was not required to be equipped with such emergency equipment.
However, 14 CFR 91.205 requires that aircraft operated for hire over water and beyond
power-off gliding distance to shore be equipped with approved flotation gear that is
readily available to each occupant.
48
The airplane was equipped with 10 PFDs.
49
According to the markings on the
PFDs, they met the requirements of FAA Technical Standard Order (TSO) C-13e, which
defines minimum performance standards for PFDs. The markings on the PFDs indicated
that they were approved for use by adults and children and that children should have their
PFDs put on them by adults per crew instruction.
The PFDs on the airplane were vests with two separate symmetrically arranged
chambers and a retention strap. The PFD is donned when a user inserts its head through a
hole in the PFD and fastens the retention strap around its waist. A PFD is inflated when
the user pulls an inflation ring that discharges carbon dioxide cartridges into the two
chambers. The user can also inflate a PFD by blowing into a tube that is located on each
chamber. A correctly donned and inflated PFD that meets the requirements of TSO C-13e
should provide the user with 35 pounds of buoyancy, automatically correctly position the
user in the water within 5 seconds, and hold the user’s nose and mouth “clear of the
waterline.”
Only 4 of the 10 PFDs installed on the airplane were retrieved and used by the
passengers.
50
The passenger in seat 3B, who was holding a child on her lap, retrieved the
PFD from under her seat. The passenger in seat 5A retrieved three PFDs and put them on
the three children accompanying her before the airplane contacted the water.
According to the passenger in the copilot seat, he could not retrieve his PFD
because it was wedged between the seat and the wall of the airplane. The passenger in
seat 2A and another passenger who tried to help her stated that they could not retrieve the
PFD for seat 2A “because the Velcro that closed the container [the fabric pouch] would
not separate.” These two passengers stated that they exited the airplane without the PFD
when the water reached knee level. The passengers who were not able to retrieve their
PFDs did not try to retrieve them until the airplane contacted the water.
Once the airplane occupants were in the water, airplanes circling the area at the
time of the accident dropped several PFDs. The passengers retrieved some of these PFDs
and distributed them. The adult female passenger (in seat 5A) and the child accompanying
48
This requirement applied to flight 527.
49
According to the President of Air Sunshine, after Tropical International Airlines purchased the
airplane in 1997, that company installed the PFDs on the airplane, which were stowed in fabric pouches that
the company had made.
50
As noted in section 1.12.1, the six PFDs that were still in the airplane were found undamaged and
were capable of normal operation.

Factual Information 23 Aircraft Accident Report
her who died after the evacuation were not wearing a PFD when they were recovered from
the water. The passenger in seat 1B reported that he took the PFD off of the child who died
after the evacuation. This passenger stated that, when he took the PFD from the child, it
was not inflated and that one of the inflation chambers had a hole in it. The passenger
stated that he provided the PFD to another passenger and that the undamaged chamber
inflated normally.
51
Another passenger stated that the other two children’s PFDs were also
not inflated and that he inflated one chamber on each of their vests.
No information indicates whether the other passengers donned their PFDs
correctly. However, during postaccident interviews, none of the passengers appeared to be
familiar with the proper donning and inflating procedures (for example, none of the
passengers reported fastening the retention straps around their waists).
Passengers reported that the airplane sank within several minutes after contacting
the water. Passengers stated that they tried to stay together in the water; however, two
groups were eventually formed, and, because of the waves, the two groups drifted apart.
Passengers reported that two of the children traveling with the female passenger in seat 5A
were extremely frightened when they entered the water and that they were frantic to the
point that they were “dangerous” to nearby passengers who were treading water.
Passengers also reported that the female passenger in seat 5A who was not wearing a PFD
was seen floating face down shortly after entering the water. The passengers were in the
water for about 1 1/2 hours before being rescued, as detailed in section 1.15.4.
1.15.4 Search and Rescue
At 1533, the Air Sunshine pilot who had just taken off from Marsh Harbor
transmitted a distress call. (That airplane’s altitude was too low to allow the pilot to
contact the Miami ARTCC directly.) The pilot of Gulf flight 9267 heard the distress call
and relayed the message to the Miami ARTCC. At 1540, the Miami ARTCC notified
MYGF that Air Sunshine flight 527 was in the water. MYGF personnel responded that the
airport did not have any helicopters and that, therefore, it could not assist with the search
and rescue. At 1541, the Miami ARTCC notified the U.S. Coast Guard at Opa-Locka,
Florida, that the flight 527 airplane was in the water.
After receiving the notification, the U.S. Coast Guard launched from Air Station
Miami one HH-65 (an Aerospaciale Dolphin helicopter), which departed about 1551 and
arrived on scene about 1702, and one Falcon jet, which departed about 1606 and arrived
on scene about 1636. In addition, the Coast Guard launched one HH-60J (a Sikorsky Jayhawk
helicopter) from Andros Island, Bahamas, which departed about 1605 and arrived on scene
about 1702.
52
Two life rafts were dropped from the Falcon after it arrived on scene. One of
51
The deceased child’s PFD was not recovered; therefore, the condition of her PFD could not be
determined.
52
According to the Coast Guard, about 1605, the winds at the crash site were about 11 knots, and the
waves were about 4 feet high. The Coast Guard did not estimate wave height for the time of its arrival on scene.

Factual Information 24 Aircraft Accident Report
the rafts landed near one of the groups of passengers
53
and was used by two adult
passengers; the other raft did not land near any of the passengers.
A rescue diver from the HH-65 recovered the pilot, one child passenger, and two
adult passengers, all of whom were hoisted into the helicopter and then flown to MYGF.
According to the rescue diver from HH-60J, he found two children wearing PFDs, and
each of the children was holding an arm of an adult female who was floating face down in
the water and “appeared to be deceased.” The diver recovered the two children, removed
one of the children’s PFDs, and placed the PFD on the deceased female.
54
The rescue diver
then recovered two additional adult passengers who were hanging onto one of the life rafts
dropped from the Falcon. All of these passengers and the rescue divers from both
helicopters were hoisted into HH-60J.
At the request of a Royal Bahamian police officer, a private fishing boat went to the
accident site about the same time as the helicopters arrived. Two men on the boat retrieved
the bodies of two passengers. The flight crew of HH-60J stated that they saw occupants on
the boat performing CPR on the two passengers. HH-60J dropped a rescue diver who
determined that one of the passengers was a child. The rescue diver hoisted the child onto
the helicopter and performed CPR on the child until landing at MYGF. The boat carried the
deceased female passenger to MYGF. After arriving at the MYGF, all of the passengers that
had been hoisted into HH-60J were transported to Rand Memorial Hospital.
1.16 Tests and Research
1.16.1 Cessna Airplane Performance Data
The Cessna 402C Aircraft Information Manual, Section 5, “Performance,”
contains a performance chart for estimating the airplane’s climb rate with one inoperative
engine. Conditions for the use of the chart include the following: operative engine power
at maximum (2,700 rpm and 39 inches Hg manifold pressure), fuel flow in the white arc
on the fuel flow gauge,
55
landing gear retracted, flaps at 0°, inoperative propeller
feathered, wing bank 5° toward operative engine with about 1/2-ball
56
slip indicated on the
turn-and-bank indicator, and inoperative engine cowl flaps closed. Safety Board
investigators used the information from Cessna’s performance chart and accounted for the
53
According to the commander of HH-60J, when the helicopter arrived on scene, the passengers were
clustered in three groups, about 110 yards away from each other.
54
The rescue diver stated that he placed one of the children’s PFDs on the deceased female so that she
would be easier to locate after the survivors were retrieved from the water.
55
According to Cessna’s Aircraft Information Manual, white arc is used for “(Takeoff and Engine
Inoperative Power-Sea Level to 12,000 feet) 200.0 Pounds per hour (16.8 psi) to 210.0 Pounds per hour
(18.0 psi).”
56
During coordinated, straight-and-level flight, the ball is centered between the turn-and-bank
indicator’s reference lines. In the event of an engine failure, the pilot banks 5° toward the operative engine to
ensure that about a 1/2-ball slip is indicated on the turn-and-bank indicator to create the most efficient bank
angle, which creates minimum drag.

Factual Information 25 Aircraft Accident Report
weight of the airplane (between 6,444 and 6,534 pounds),
57
the outside air temperature
(90° F), the winds (about 15 knots),
58
and the altitude (3,500 feet) at the time that the right
engine failed in estimating that the airplane would have had a climb rate of about 200 fpm
if nothing had occurred to negatively affect the airplane’s performance.
Cessna provided the following climb rate penalty data:
59
flaps at 15° (the
configuration at which the accident airplane was found) at 103, 100, and 95 knots yields
penalties of -165, -155, and -145 fpm, respectively; a windmilling propeller (pilot and
passenger statements indicated that the right engine propeller was windmilling, not
feathered, after the right engine failed) yields a penalty of -400 fpm; cowl flap of
inoperative engine open (the postaccident configuration in which the airplane’s right
engine cowl flap was found) yields a penalty of -9 fpm; and protruding magnetos (the
right engine magnetos penetrated the engine cowling in flight) yields a penalty of -4 fpm.
1.16.2 Airplane Performance Study
The Safety Board conducted an airplane performance study to establish the effects
that the pilot’s actions, airplane damage, and windmilling propeller had on the airplane’s
performance after the right engine failed. Because the airplane did not have an FDR or a
CVR and no radar data relating to the accident flight were available, the study used
statements from the pilot, passengers, and Air Sunshine’s station manager to determine the
sequence of the pilot’s actions throughout the flight.
With the use of the data provided by Cessna and a range of average indicated
airspeeds between 115 and 95 knots,
60
the airplane performance study determined that the
airplane’s descent rate was between about 560 and 212 fpm during its descent from
3,500 to 2,000 feet. The airplane traveled between about 5 and 10 nautical miles during
this portion of the flight. With the use of a range of average indicated airspeeds between
105 and 90 knots, the study determined that the airplane’s descent rate was between about
429 and 360 fpm during its descent from 2,000 feet to the point of contact with the water.
The airplane traveled about 7.6 nautical miles during this portion of the flight. At the time
of the right engine failure, the airplane was about 20 to 25 miles from MYAT. The study
determined that the airplane was airborne for at least 7 minutes after the right engine failed
and before it contacted the water. At 90 knots, and with the engine damage, the airplane
57
The difference in weight would have caused less that a 40 fpm difference in the climb rate.
58
Airport weather data were obtained from Miami International Airport and MYGF. The data showed
that the estimates provided by the pilot (the winds were about 15 knots, and the outside air temperature was
80° to 90° F) at the time of the ditching were accurate.
59
Cessna could not quantify the penalties for the following variables that also could have decreased the
climb rate: operation of the airplane at greater or less than the recommended wing bank of 5° toward
operative engine; operation of the airplane at greater or less than the recommended 1/2-ball slip on the
turn-and-bank indicator; and operation of the airplane on a nonsteady descent (for example, decreasing pitch
angle to increase speed and then reducing pitch to arrest descent rate).
60
According to the pilot, the blue radial on the accident airplane’s airspeed indicator, which shows the
single-engine best climb rate, was pointing to about 105 knots.

Factual Information 26 Aircraft Accident Report
could have tolerated a descent rate of an average of about 200 fpm and been able to
maintain flight and reach MYAT.
1.16.3 Metallurgical Inspections
1.16.3.1 Right Engine Cylinder Assemblies
The right engine No. 2 cylinder assembly was separated from the engine
crankcase. The other five cylinder assemblies were intact and attached to the engine
crankcase.
The Nos. 1, 3, 4, 5, and 6 cylinder bores were covered with corrosive material and
sand and salt residue, consistent with salt water immersion. No discernible damage to the
cylinder assemblies or to the valves was noted. All of the valves and valve springs were
intact and undamaged. The valve faces and springs were coated with sand, salt, and oil,
and the faces were oxidized.
The No. 2 cylinder assembly was generally intact with no apparent damage to the
valves or cylinder head. The cylinder bore was covered by a layer of corrosive material;
no large-scale marking, scoring, or gouging was found under the corrosion.
The No. 2 cylinder skirt area (the inboard portion of the cylinder that projects into
the engine crankcase when assembled) was damaged and deformed in multiple places.
The damage displaced various portions of the inboard edge of the cylinder skirt both
toward and away from the cylinder centerline. The spacing between the deformed areas
was about equal to the distance between the No. 2 cylinder hold-down studs and through
bolts. The cylinder base flange was also damaged with the two upper aft mounting holes
(at the intact stud locations) distorted adjacent to the inboard (case side) surface.
Five of the engine cylinder assemblies (Nos. 1 through 5) had markings on the
heads and base flanges, identifying them as FAA Parts Manufacturing Approval
components. The letters “EC” were steel-stamped into the cylinder head, indicating that
the cylinders were manufactured by Engine Components, Inc (ECI). One of the valve
rocker bosses on each of these cylinders was also marked with steel-stamped numbers 29689-1
through -5. The first five numbers corresponded to the work order number for the last
engine overhaul performed by Airmark Overhaul, and the last number corresponded to the
position of the cylinder (1 through 5). The cylinders were installed in their respective
positions on the engine crankcase.
The markings on the No. 6 cylinder were not consistent with those on an
ECI-manufactured cylinder. The letters “DET” and “E” and the number “99” were
steel-stamped into the cylinder head. One of the valve rocker bosses was marked with the
steel-stamped number “33258-3,”
61
and another of the rocker bosses was vibro-etched
with the number “7-99.”
61
This work order number corresponded to a propeller strike inspection that was conducted on another
one of the company’s engines, serial number 816113-R. For more information about this engine, see section
1.17.1.3.1.

Factual Information 27 Aircraft Accident Report
1.16.3.2 Right Engine Pistons
The Nos. 1, 3, 4, 5, and 6 pistons from the right engine were intact. The No. 2
piston was found fractured into two large pieces and many small pieces. Only about
35 percent of the No. 2 piston was recovered.
Magnified optical examinations of the fractures on the No. 2 piston found features
consistent with overstress separations; no indications of preexisting cracking were found.
On the largest piece, the piston was circumferentially fractured along the lower oil control
ring and vertically in the plane of the piston pin but offset to one side. Deformation on the
outer edge of the piston skirt adjacent to the fracture at the oil control ring groove was
consistent with partial canting of the piston in the cylinder after the fracture occurred.
1.16.3.3 Right Engine Crankcase
The left half of the right engine crankcase was fractured and damaged in line with
the No. 2 cylinder connecting rod, which was consistent with continued rotation of the
engine and flailing of the connecting rod after the complete separation of the cylinder. The
right half of the engine crankcase was also damaged in line with the No. 2 cylinder
connecting rod. The main portion of the connecting rod was heavily distorted in the rod
bearing and piston pin areas. The piston pin area had many impact marks, and the pin hole
and bushing were flattened. The connecting rod bolt pieces were also distorted and
fractured through the shank. Optical examinations revealed fracture features consistent
with overstress separations. A portion of the crankcase, which contained the two upper
center studs of the No. 2 cylinder, was missing.
The engine crankcase surfaces that contact the cylinder skirt and base flange of the
No. 2 cylinder contained several different impact marks and contact features. Small, raised
ridges were present on the forward side of the mounting face corresponding to the
installed edges of the No. 2 cylinder base flange. Additionally, the bore portion of the
crankcase that mates with the No. 2 cylinder skirt contained several sharp circumferential
dents, scrapes, and other contact marks that are consistent with progressive outboard
movement of the cylinder skirt. The cylinder skirt edge marks continued onto the lower
portion of the mounting surface where a series of concentric dents, which matched the
machined contour and overall radius of the innermost edge of the cylinder skirt, were
found. Light fretting damage was noted in some areas of the contact surface with the
cylinder base flange.
1.16.3.4 Right Engine No. 2 Cylinder Hold-Down Studs and Through Bolts
Of the eight hold-down studs and two through bolts that retain the No. 2 cylinder to
the engine crankcase, three of the studs were found intact in the crankcase without nuts, four
of the studs and the two through bolts were found fractured, and one of the studs was not
found. The intact studs found in the crankcase without nuts had minimal thread damage.
The outboard portions of one of the fractured hold-down studs and one of the
fractured through bolts were recovered. The stud piece was found without a nut attached,

Factual Information 28 Aircraft Accident Report
and the through bolt piece was found with a nut attached. The outboard portions of the
other three fractured studs were not recovered. The other fractured through bolt, which is
where the nut would normally be, was not recovered. Figure 4 shows the condition in
which the right engine No. 2 cylinder retention system components were found.
Note: The cylinder base flange is outlined in blue, and the mounting surface is outlined in red.
Optical and scanning electron microscopic examinations of four of the hold-down
stud and two of the through bolt fractures found features that were consistent with
high-stress and low-cycle fatigue propagation. For all of the studs and through bolts with
fatigue cracking, initiation was from multiple locations in a thread root along one side of the
fastener. The fatigue propagated in a high-stress manner with parallel fissures and striations
until ductile overstress occurred at about 50 percent of the fastener’s cross-section. Some
spots of corrosive material were visible at random areas across the fractures; however, little
or no oxidation or corrosion was apparent in the fracture origin areas. A comparison of
height measurements of the No. 2 cylinder studs’ features with features on other cylinder
studs in the engine crankcase revealed that the studs had been installed to similar depths.
Figure 4. The condition in which the right engine No. 2 cylinder retention system
components were found.
Through Bolt Fatigue,
Nut in Place
Stud Intact,
Case Threads Stripped,
No Nut
Through Bolt Fatigue,
Outboard Piece
Not Recovered
Stud Fatigue,
Outboard Piece
Not Recovered
Stud Fatigue,
Outboard Piece
Not Recovered
Stud Fatigue,
Outboard Piece
Not Recovered
Stud Intact,
No Nut
Stud Intact,
Bent, No Nut
Stud Intact,
Missing from Case
Stud Fatigue,
Outboard Piece
Recovered, No Nut

Factual Information 29 Aircraft Accident Report
1.16.3.5 Cylinder Hold-Down Nuts
The cylinder hold-down nuts from the Nos. 1, 3, 4, 5, and 6 right engine cylinders
were recovered on their respective hold-down studs and through bolts; three of the
hold-down nuts were found in the engine compartment. Thirty 7/16-inch-diameter,
6-point, flanged cylinder hold-down nuts were examined. Two of these hold-down nuts
were found in the engine compartment after recovery of the airplane, and 28 of these
hold-down nuts were removed from the right engine cylinders during engine teardown.
Initial optical examinations found two different styles of nuts. Seven of the nuts
had concave transition from the wrench flats to the enlarged washer flange. These nuts
were consistent with an exemplar cylinder hold-down nut provided by Superior Air Parts
with standard 7/16-20 UNF-3B thread form.
62
Twenty-three of the nuts had a convex
transition from the wrench flats to the enlarged washer flange and were embossed with
two opposed sets of parallel lines. These nuts were consistent with TCM flanged nuts with
the optional, nonstandard Spiralock thread form.
63
According to TCM, the company has
exclusively procured cylinder hold-down nuts with the Spiralock thread form since
about 1990. One of the nuts found loose in the engine compartment was a Superior-style
hold-down nut, and the other nut was a TCM-style nut with the Spiralock thread form.
According to Airmark Overhaul’s Quality Assurance Manager, the company uses
OEM-specified hold-down nuts or nuts provided by Superior Air Parts. The manager
stated that, since he began working at Airmark in April 1984, if the company was
overhauling an engine and 36 6-point cylinder hold-down nuts were needed and 24 with a
TCM part number and 12 with a Superior Air part number were in stock, both types of
nuts would be used to complete the overhaul rather than hold up production. He stated that
this procedure was “accepted in industry.”
1.17 Organizational and Management Information
1.17.1 Air Sunshine
Air Sunshine, Inc., was formed in June 1982 and began conducting Part 135
on-demand charter flights on September 2, 1982, and Part 135 scheduled commuter flights
in 1983. The company provides commuter and charter services in South Florida and the
Caribbean. The company has offices and a permanent maintenance facility in Fort
Lauderdale. The company has a ticket counter and two rooms at Luis Munoz Marin
International Airport (SJU), San Juan, Puerto Rico, but no permanent maintenance facility
there. Air Sunshine’s President stated that the company keeps its maintenance records in
the two rooms it has at SJU.
62
Standard 7/16-20 internal threads have a 7/16-inch major diameter and 20 threads per running inch of
UN fine 60° threads with a class 3 fit.
63
Spiralock internal threads are proprietary and were developed by Spiralock Corporation, a subsidiary
of Detroit Tool Industries Company. The internal threads of the Spiralock nut engage the external threads at
the crests of the stud threads.

Factual Information 30 Aircraft Accident Report
At the time of the accident, the company employed 12 pilots, 10 of whom were
captains and 2 of whom were first officers. According to Air Sunshine’s President, the
company typically employed three A&P-certified mechanics and one or two assistant
mechanics in San Juan and four A&P-certified mechanics and three assistant mechanics in
Fort Lauderdale. The company operated three to four flights daily out of FLL and about
six to eight flights daily out of SJU with a fleet of seven Cessna 402C airplanes and one
Embraer 110 airplane.
The Director of Maintenance stated that company maintenance was conducted in
both Fort Lauderdale and San Juan. According to the director, if an airplane is in Fort
Lauderdale when an inspection becomes due, the inspection is conducted there. He stated
that, because most of the flights conducted on its Cessna 402 airplanes originated in San
Juan, most of the inspections of these airplanes were conducted there.
64
Air Sunshine’s
President stated that extensive maintenance and sheet metal work were conducted in Fort
Lauderdale because the company owned a hangar at FLL. He stated that inspections
conducted in San Juan were typically conducted on the ramp and that, if an airplane
needed to be “placed on jacks,” the company would obtain hangar space at SJU.
Since March 26, 1987, Air Sunshine has experienced four incidents and six
accidents, including the flight 527 accident. Three of the accidents, including the accident
flight, resulted in fatalities. On January 23, 1992, a Cessna 402C crashed near Clewiston,
Florida, and two people were killed. On February 8, 1987, a Cessna 402C crashed into the
Atlantic Ocean while on final approach to Cyril E. King Airport, Charlotte Amalie, Virgin
Islands, and two people were killed. Both accidents were determined to be caused by pilot
error; no mechanical malfunctions were reported with either airplane.
1.17.1.1 Air Sunshine’s In-Flight Engine Failure Procedures
In-flight engine failure procedures were taught during company training and were
contained in Air Sunshine’s Training Manual. The manual states that, if an engine were to
fail in flight, the pilot should comply with memory items and follow the prescribed checklist.
Air Sunshine’s Training Manual, section 3, revision 6, dated May 10, 1990, contains the
following in-flight engine failure procedures:
1. Inoperative Engine – DETERMINE.
2. Operative Engine – ADJUST as required.
Before Securing [shutting down] Inoperative Engine:
3. Fuel Flow – CHECK. If deficient, position auxiliary fuel pump to ON.
4. Fuel Selectors – MAIN TANKS (Feel For Detent).
5. Fuel Quantity – CHECK.
64
Air Sunshine’s General Manager reported to Safety Board investigators that the company conducted
45 inspections of its Cessna 402 airplanes in Fort Lauderdale and 17 inspections of its Cessna 402 airplanes
in San Juan between January 1 and July 13, 2003.

Factual Information 31 Aircraft Accident Report
6. Oil Pressure and Oil Temperature – CHECK.
7. Magneto Switches – CHECK ON.
8. Mixture – ADJUST. Lean until manifold pressure begins to increase, then
enrich as power increases.
Air Sunshine’s Training Manual states that, if the engine does not start after
performing the first eight steps of the in-flight engine failure procedures, the pilot was to
perform the following procedures:
65
9. Inoperative Engine – SECURE [shut down].
a. Throttle – CLOSE.
b. Mixture – IDLE CUT-OFF.
c. Propeller – FEATHER.
d. Fuel Selector – OFF (Feel For Detent).
e. Auxiliary Fuel Pump – OFF.
f. Magneto Switches – OFF…
i. Cowl Flap – CLOSE…
10. Trim Tabs – ADJUST 5° bank toward operative engine with approximately
1/2 ball slip indicated on the turn and bank indicator.
Air Sunshine’s Training Manual also stated that, if an engine failure were to occur,
the single-engine best climb rate should be maintained regardless of whether the altitude
could be maintained because that speed guaranteed the best climb rate or the least altitude
loss with an inoperative engine. Cessna’s 402C Aircraft Information Manual, Section 3,
“Emergency Procedures,” states the following:
The one engine inoperative best rate-of-climb speed becomes important when
there are no obstacles ahead on takeoff, or when it is difficult to maintain or gain
altitude in single-engine emergencies. The one engine inoperative best
rate-of-climb speed is 104 KIAS with wing flaps and landing gear up. This speed
is indicated by a blue radial on the airspeed indicator.
During postaccident interviews, the accident pilot stated that he was trained by Air
Sunshine that, in the event of an in-flight engine failure, a pilot should push “all the engine
levers forward (throttle, mixture, and propeller levers).” As noted previously, the pilot
stated that his first action after he heard the bang and saw oil coming out of the right
engine cowling was to shut down the failed engine. The pilot stated that he did not follow
the company’s in-flight engine failure procedures because he knew which engine had
failed. The pilot added that he did not follow the in-flight engine failure checklist because
he was “too busy flying the airplane.” The passenger in the copilot seat stated that the pilot
pushed the throttle, mixture, and propeller levers of the operative engine forward
immediately after he tried to shut down the failed engine.
65
These procedures were also contained in Cessna’s 402C Aircraft Information Manual.

Factual Information 32 Aircraft Accident Report
Air Sunshine’s Director of Operations, who is also a check captain and conducts
company training, stated that he trained pilots to perform the following procedures if an
in-flight engine failure occurred: (1) mixture [lever] – full forward, (2) propeller [lever] –
full forward, (3) throttles [lever] – full forward, (4) flaps – up [retracted], (5) gear – up
[retracted], (6) fuel selector – on main tanks, (7) auxiliary pump – on, (8) identify the
failed engine, (9) verify the failed engine, (10) feather the propeller, and (11) call for the
[engine failure] checklist.
1.17.1.2 Ditching Procedures
Air Sunshine’s Training Manual, section 3, contained the following ditching
procedures:
Landing Gear – UP.
Approach – HEADWIND if high winds. PARALLEL to SWELLS if light wind
and heavy swells.
Wing Flaps – DOWN 45°.
Power – AS REQUIRED (300 Feet Per Minute Descent).
Airspeed – 95 KIAS minimum.
Attitude – DESCENT ATTITUDE through touchdown.
The pilot stated, during postaccident interviews, that he did not extend the flaps
before ditching.
1.17.1.3 Company Record-Keeping
1.17.1.3.1 Maintenance Records
As noted previously, although Air Sunshine’s Director of Maintenance told Safety
Board investigators that he and the assistant mechanic had repeated the compression
checks after initially getting unacceptably low readings (below 54 psi) for two of the right
engine cylinders (Nos. 2 and 4) during the airplane’s last scheduled engine maintenance in
June 2003, no documentation of the repeated checks was found. Further, no records were
found indicating that any inspections or corrective maintenance had been performed on
the right engine cylinders after getting the low compression check readings. As previously
mentioned, TCM SB 03-3 recommends that, if cylinder pressure levels are lower than the
limit established by the acceptable pressure leakage check (in this case, 54 psi), a cylinder
borescope inspection is to be conducted. In addition, no records were found indicating that
any of the right engine cylinders had been removed since the engine was last overhauled
(December 14, 1999).
A review of Air Sunshine’s maintenance records revealed that the number stamped
on the No. 6 cylinder from the right engine did not match the number recorded in the
maintenance records; however, the maintenance records for the right engine did not

Factual Information 33 Aircraft Accident Report
indicate that the No. 6 cylinder had ever been removed or replaced. Air Sunshine’s General
Manager stated that, according to company records, the cylinder installed in the No. 6
position on the accident airplane was a cylinder previously installed in the No. 3 position on
another one of the company’s engines, serial number 816113-R, which was installed on
N220RS. The General Manager stated that, from January to July 2001, engine serial
number 816113-R was not installed on N220RS and that, during that time, the engine “was
basically sitting in [the company’s] parts room.” He added that the No. 3 cylinder from
engine serial number 816113-R must have been installed on the accident engine at some
point during that time. However, the maintenance records for N220RS did not indicate that
the No. 3 cylinder had ever been removed or replaced from engine serial number 816113-R.
Further, a review of Air Sunshine’s maintenance records revealed no reports to the FAA
that any of the company’s engines were running unsatisfactorily from the date that its
operations specifications were amended (September 9, 1999) to the date of the accident.
66
1.17.1.3.2 Aircraft Flight Logs
A Safety Board review of the accident airplane’s flight logs from the first flight
conducted on December 23, 2002, to the last flight conducted on July 12, 2003, revealed
that the airplane had been operated a total of 543.8 hours on 559 flights. During this time,
pilots reported three maintenance-related discrepancies.
A review of the flight logs also revealed that the first flight to be conducted after
the last phase 1 check (June 14, 2003) occurred on June 16, 2003. From the June 16th
flight to the first flight conducted on the day of the accident, the airplane had been
operated a total of 79.7 hours on 83 flights. During this time, no pilot-reported
maintenance-related discrepancies were recorded.
1.17.2 Federal Aviation Administration Oversight
1.17.2.1 General
Air Sunshine was initially certificated in 1982 by the Miami FSDO. The
company’s operations certificate was transferred to the Fort Lauderdale FSDO in 1986. As
noted previously, in early 1998, Air Sunshine asked the FAA to transfer its operations
certificate to the San Juan FSDO. The FAA granted the request, and the certificate was
transferred to the San Juan FSDO on June 2, 1998.
According to the PMI for Air Sunshine, airplanes that are based at FLL are
maintained there, and airplanes that are based at SJU are maintained there. The PMI, who
is based in San Juan, reported that he scheduled three to four trips a year to FLL as part of
his work program.
66
As noted previously, the PMI stated that he would grant Air Sunshine’s request to amend its
operations specifications provided that the company monitored the performance of newly overhauled
engines and reported any abnormal conditions to the San Juan FSDO.

Factual Information 34 Aircraft Accident Report
1.17.2.2 San Juan Flight Standards District Office Preaccident Oversight of
Air Sunshine
According to the FAA’s planned oversight program for Air Sunshine, the PMI
planned on conducting the following inspections for fiscal year 2003 (from October 1,
2002, to September 30, 2003): two required and two additional facility inspections at FLL,
two required and two additional ramp inspections of the Embraer 110 at FLL, two
required and two additional ramp inspections of the Cessna 402s at FLL, one required and
one additional spot check of the Cessna 402s at FLL, one required aircraft (Embraer 110)
records inspection and one additional aircraft records inspection at FLL, and one required
maintenance records inspection and one additional maintenance records inspection at SJU.
A review of FAA records indicated that, from October 1, 2002, to July 8, 2003, the PMI
conducted 10 ramp inspections, 2 spot inspections, and 1 aircraft records inspection.
The review of FAA records also indicated that the PMI conducted an inspection of
Air Sunshine’s Fort Lauderdale facility from March 25 to 27, 2003. In an April 1, 2003,
letter to the company, the PMI stated that he found five Maintenance Manual-related
discrepancies during the inspection. The PMI also reported that he conducted an
inspection of Air Sunshine’s San Juan facility from July 8 to 10, 2003. In a July 15, 2003,
letter to the company, the PMI stated that he found three Maintenance Manual- and three
aircraft records-related discrepancies. None of the aircraft records-related discrepancies
involved the accident airplane.
1.17.2.3 Fort Lauderdale Flight Standards District Office Postaccident
Oversight of Air Sunshine
Although the Fort Lauderdale FSDO has no maintenance oversight responsibilities
for Air Sunshine, according to an aviation safety inspector from Fort Lauderdale, after the
accident, the Fort Lauderdale FSDO Manager contacted the San Juan FSDO Manager to
advise him that the Fort Lauderdale FSDO wanted to conduct additional surveillance of Air
Sunshine. A review of FAA records indicated that, from July 14 to September 30, 2003,
personnel from the Fort Lauderdale FSDO conducted 2 facility inspections, which found
scales that were out of calibration and cargo that was not secured; 21 ramp inspections,
which found numerous maintenance-related discrepancies with Air Sunshine’s Cessna 402C
airplanes; and 5 spot inspections, which found numerous maintenance-related discrepancies.
1.17.2.4 San Juan Flight Standards District Office Postaccident Oversight of
Air Sunshine
According to the FAA, after the accident, the San Juan FSDO increased
surveillance of Air Sunshine in all areas. The FAA stated that, from July 14, 2003, to
February 25, 2004, the San Juan FSDO conducted 45 inspections of the company.
From July 22 to August 29, 2003, the San Juan FSDO conducted a focused
inspection of Air Sunshine. During this inspection, the FAA determined that the
company’s record-keeping system was inadequate, its maintenance program was deficient,
its passenger briefing card and overwater safety briefing needed to be revised, its pilot
training needed to be revised, and its engine compression check interval was too high.

Factual Information 35 Aircraft Accident Report
The FAA stated that, as a result of these inspections, the following actions were taken:
• The FAA filed an Enforcement Investigative Report regarding the deficiencies
found in Air Sunshine’s record-keeping system. The FAA stated that
subsequent records inspections revealed that the deficiencies were corrected.
• The FAA sent a letter to Air Sunshine, addressing all of the maintenance
discrepancies. The FAA stated that all of the corrective actions were
documented in its PTRS.
• The FAA sent a letter to Air Sunshine, requiring the company to revise its
General Operations Manual, section 3 (relating to the passenger briefing card
and the overwater safety briefing). On October 1, 2003, the FAA accepted
revision No. 31, which amended the overwater safety briefing. On July 6, 2004,
the FAA accepted revision No. 32, which amended the passenger briefing card.
• The FAA sent a letter to Air Sunshine, requesting that the company revise its
FAA-approved Pilot Training Manual. On February 12, 2004, the FAA
accepted revision No. 15, which corrected outdated information and
training-hour requirements and conformed to the new format of FAA Order
8400.10, Air Transportation Operations Inspector’s Handbook.
• On November 18, 2003, Air Sunshine submitted and the FAA approved
revision No. 11 to Air Sunshine’s AAIP, which lowered the compression check
interval from 360 to 120 hours.
1.17.2.5 Additional Postaccident Actions
On February 26, 2004, Air Sunshine’s PMI sent the company a letter regarding its
AAIP. The PMI stated that, effective immediately, the company’s Operations
Specification Part D-101 would be amended to specify that only TCM could rebuild the
company’s TCM TSIO-520-VB engines. The PMI further stated that, pending mitigating
actions on the part of Air Sunshine, he was proposing to reduce the TBO from 2,400 flight
hours to the manufacturer-recommended TBO of 1,600 flight hours, effective March 12,
2004. The PMI asked Air Sunshine to provide in writing, by March 4, 2004, a detailed
plan for any actions that the company planned on taking in response to the PMI’s letter.
In a letter to the FAA dated March 3, 2004, Air Sunshine’s General Manager
responded that the company did not agree with the FAA that TCM rebuilt engines were
superior to engines that were overhauled by Airmark Overhaul. He added that Airmark
was a TCM distributor and that Airmark used TCM guidelines and “brand new
millennium cylinders.”
67
He further stated that “throughout the years we have found
quality control and attention to details of Airmark highly superior to the mass production
errors inherent of large factories like TCM.” The manager asked the PMI to reconsider its
decision to require Air Sunshine to use only TCM rebuilt engines.
The General Manager stated that the company would revise its AAIP to include a
cylinder inspection every 1,600 flight hours, which would include replacement of valves,
67
“Millennium” cylinders are Superior Air Parts cylinders. Five of the six cylinders from the right
engine were ECI cylinders.

Factual Information 36 Aircraft Accident Report
rings, and gaskets. The manager also stated that the cylinder inspection would include, if
necessary, replacement of valve seats, guides, and pistons. He added that the company
would revise its compression check interval and place additional constraints, such as
replacing of cylinders if the compression levels fell below the limit established in
accordance with TCM SB 03-3. The manager stated that the company had already revised
its AAIP to require three compression checks during a 360-flight-hour inspection cycle
(compression checks would be conducted once every 120 flight hours). At the time of the
accident, one compression check was required during a complete inspection cycle
(compression checks were conducted once every 360 hours).
The General Manager stated that Air Sunshine was also willing to conduct
cylinder inspections on the four engines in its fleet that had more than 1,600 flight hours
and that the company had already ordered one new TCM engine to replace an engine that
had about 2,200 flight hours. The manager also stated that the company had followed all
of the guidelines to obtain the TBO extension to 2,400 flight hours, including preparing
five engine teardown reports, and that the company had operated for 11 years and for more
than 100,000 flight hours under the extended TBO.
1.18 Additional Information
1.18.1 Previous Ditching Accidents
On January 1, 2002, a Piper PA-31 operated by Air Taxi, Inc., as a Part 135
nonscheduled commuter flight was ditched in the Atlantic Ocean after fuel exhaustion.
Three passengers and the pilot sustained serious injuries, and one passenger died.
According to the surviving passengers, the pilot did not conduct a preflight briefing or an
emergency briefing before the ditching. Four of the PFDs on board the airplane were
retrieved after the airplane was in the water.
68
On August 20, 2000, a Piper PA-31 operated by Big Island Air as a Part 135
commuter flight was ditched in the Pacific Ocean after a loss of engine power. All of the
passengers retrieved their PFDs before the ditching. The passengers reported that, shortly
after the engine problem occurred, the pilot instructed them to retrieve and don their PFDs
and assume a crash position. One passenger retrieved, donned, and partially inflated her
PFD, but she was not able to evacuate the airplane and, as a result, died.
68
A description of this accident, MIA04FA48, can be found on the Safety Board’s Web site at
<http://www.ntsb.gov>.

37 Aircraft Accident Report
2. Analysis
2.1 General
The pilot was properly certificated and qualified under Federal regulations. No
evidence indicated any preexisting medical or physical condition that might have
adversely affected the pilot’s performance during the accident flight.
The airplane was properly certificated and equipped in accordance with Federal
regulations. The airplane was equipped with FAA-approved flotation gear, as required by
Federal regulations.
The airplane was loaded in accordance with FAA-approved company weight and
balance procedures. The weight and balance of the airplane were within prescribed limits
during all phases of the flight.
Given the distance from shore at which the ditching occurred and the availability
of emergency response equipment, the search and rescue efforts were timely and
appropriate. The accident was survivable.
69
The inoperative distance measuring equipment on the MYAT VOR was not a
factor in this accident.
This analysis discusses the accident sequence, including the airplane’s
performance after the right engine failed and the cause of this failure. This analysis also
discusses Air Sunshine-related maintenance issues, pilot proficiency, and the need for
emergency briefings.
2.2 Accident Sequence
The accident flight departed FLL about 1427. The takeoff and cruise portions of
the flight were uneventful. The pilot reported that the flight’s cruise altitude was about
7,500 feet and that the cruise speed was about 160 KIAS.
The pilot reported that, while descending through an altitude of about 3,500 feet at
an airspeed of about 135 to 140 KIAS and a distance of about 20 to 25 miles from MYAT,
he heard a bang and saw oil coming out of the right engine cowling. Several of the
passengers reported seeing white smoke coming from the engine followed by a stream of
oil and then hearing a loud bang. The passengers reported seeing parts falling from the
69
Although the accident was survivable, two passengers died after evacuating the airplane. Section 2.9
discusses the pilot’s failure to conduct an emergency briefing after the right engine failed and this failure’s
effect on the outcome of the accident.

Analysis 38 Aircraft Accident Report
engine after they heard the loud bang. The pilot reported that, after attempting to shut
down the right engine, he applied full power to the left engine and slowed to about 95 KIAS,
but he could not maintain altitude. He stated that, once the airplane descended through an
altitude of about 1,500 to 1,000 feet, he realized that the airplane could not make it to the
airport and, therefore, he decided to ditch the airplane.
The on-site examination of the airplane after it was recovered from the water
revealed that both of the right engine magnetos had penetrated through the engine cowling
and that they were hanging onto the engine by their harnesses. After opening the engine
cowling, the No. 2 cylinder was found separated from the engine crankcase at the cylinder
flange. Therefore, the Safety Board concludes that the airplane’s right engine failed while
the airplane was descending through an altitude of about 3,500 feet.
2.3 Airplane Performance After the Right Engine Failure
Air Sunshine’s Training Manual states that, if a failed engine does not start after
performing steps 1 through 8 of the in-flight engine failure procedures (see section 1.17.1.1),
the pilot should close the throttle, cut off mixture, and feather the propeller on the
inoperative engine; move the fuel selector, auxiliary fuel pump, and magneto switches for
the inoperative engine to off; and close the cowl flaps. The left fuel selector valve in the
cockpit was found positioned to the left main fuel tank; the position of the right fuel selector
valve was not determined. The right cowl flap was found open. Further, Air Sunshine’s
Training Manual states that, before ditching, the pilot should extend the wing flaps to 45°.
The pilot stated that he did not extend the flaps before ditching; however, the Safety Board
notes that the airplane was found with the left and right flaps extended to 15°.
70
Several factors existed that adversely affected the airplane’s performance,
including the windmilling propeller (-400 fpm penalty), the protruding magnetos (-4 fpm
penalty), and the open right engine cowl flap (-9 fpm penalty). In addition, flaps that are
extended to 15° could cause a -145 to -165 fpm penalty. However, Safety Board
investigators could not determine when the flaps were extended; therefore, it is unknown
when the penalty for flaps at 15° started.
Several other factors could also have degraded the airplane’s performance,
including not flying at the recommended airspeeds, operating with a bank angle and
sideslip not in accordance with Cessna’s recommended in-flight engine failure
configuration, and not maintaining a steady descent. However, Cessna could not quantify
the penalties for these variables. The Safety Board calculated that, at an airspeed of
90 knots and with the engine damage, the airplane could have tolerated a descent rate of
about 250 fpm and have been able to maintain flight and reach land. The pilot stated that,
during the ditching, the descent rate was between about 200 and 300 fpm. Board
calculations showed that the airplane’s descent rate was between 560 and 212 fpm during
its descent from 3,500 feet to 2,000 feet and was between 429 and 360 fpm during its
descent from 2,000 feet to contact with the water.
70
The pilot stated that one of the passengers might have hit the electrically controlled switch that
extends the flaps while they were evacuating the airplane.

Analysis 39 Aircraft Accident Report
On the basis of this evidence, the Safety Board concludes that several factors
contributed to the degradation of the airplane’s performance and its inability to maintain
flight and reach land, including the windmilling propeller, the protruding magnetos, the open
right engine cowl flap, and the possibility that the flaps were extended to 15° at some point
during the descent. The Safety Board further concludes that, during the descent from 3,500
to 2,000 feet, the airplane’s descent rate was between about 560 and 212 fpm, and that,
during the descent from 2,000 feet to contact with the water, its descent rate was between
429 and 360 fpm. The Safety Board also concludes that, if the average descent rate had been
about 200 fpm or less, the airplane would have been able to maintain flight and reach MYAT.
The pilot stated that, when he tried to feather the right propeller, it continued to turn
until the airplane contacted the water. Two passengers stated that the propeller continued
turning until the airplane contacted the water. However, when the propeller was removed
and examined, the blade angles were measured to be within the specified range for feather
(82.2° +/-0.3°). Further, the propeller’s start-lock mechanism showed no evidence of
damage, such as witness marks, which would have been expected if the propeller had been
on the start locks at the time that it contacted the water. Therefore, the Safety Board
concludes that the right propeller was in the fully feathered position, but Board
investigators could not determine at what point the propeller became fully feathered.
2.4 Right Engine Failure Sequence
Previous Safety Board investigations of engine cylinder separations have shown
that cylinder stud failures generally occurred as a progressive sequence of fatigue
fractures. Typically, the initial fracture has been caused by high-cycle, low-stress fatigue
(indicating preexisting cracking that was not created during the engine cylinder
separation) and has penetrated nearly the entire fastener section. Subsequent fractures
have shown decreasing amounts of fatigue followed by overstress and fracture features
that were increasingly indicative of high-stress propagation. However, the accident
airplane right engine No. 2 cylinder stud fractures showed no evidence of a progressive
sequence of fatigue, indicating that a sudden onset of higher loads occurred.
Although combustion instabilities, such as detonation or preignition, can cause the
rapid increase of the loads on the studs, no evidence of such an event was found. A partial
piston or ring failure can also increase the loads on the studs; however, metallurgical
evidence indicated that the No. 2 cylinder piston fractures were caused by sudden
overstress. Optical examinations of the fractured studs and through bolts confirmed that
they failed as a result of high-stress fatigue.
Small, raised ridges observed on the forward side of the right engine No. 2
cylinder mounting face indicated that the cylinder was rocking on the engine crankcase,
pivoting around the through bolt on the forward side of the base flange. For this motion to
occur, some of the cylinder studs opposite of this location had to become fractured or the
nuts opposite of this location had to become loose. Two of the studs from this area were
found intact but without the nuts.

Analysis 40 Aircraft Accident Report
In addition, two intact cylinder hold-down nuts were found in the engine
compartment area. Typically, cylinder hold-down nuts become separated from the cylinder
hold-down studs if the threads on the nuts or studs are stripped (pulled out) or if the nuts
become loose and unthreaded by vibration. The threads on the two cylinder hold-down
nuts found in the engine compartment area were intact; the damage to the threads of the
nonfractured studs in the engine crankcase was minimal. Therefore, the hold-down nuts
on the two unfractured studs must have become loose and backed off of the studs. The
Safety Board is unaware of any previous instances of cylinder separations in which the
hold-down nuts completely backed off of multiple studs.
The loss of the cylinder hold-down nuts on the two unfractured studs would have
caused the loads to be transferred to the remaining studs and through bolts. The increased
load would have been sufficient to initiate and propagate high-stress fatigue fractures in
four of the remaining studs and both through bolts; the loads on the remaining stud would
have been sufficient to strip its case threads. The presence of fractures of the four broken
studs, the fractures of the two broken through bolts, and the stripped case threads at
another stud location indicated that the nuts were present on these studs and through bolts
for a significant portion of the failure sequence.
Several sharp circumferential dents, scrapes, and other contact marks on the bore
portion of the case that mates with the No. 2 cylinder skirt show that the failure of the
No. 2 cylinder retention system caused the progressive outboard movement of the
cylinder. At some point, the piston fragmented and, the connecting rod, wrist pin, and
piston fragments separated from the engine.
On the basis of the metallurgical evidence, the Safety Board concludes that two or
more of the right engine No. 2 cylinder hold-down nuts became loose and backed off of
the studs, which resulted in the remaining studs and through bolts fracturing in high-stress
fatigue, allowing the cylinder to separate from the engine.
2.5 Cause of the Loosened No. 2 Cylinder Hold-down
Nuts
The probability that two or more cylinder hold-down nuts would simultaneously
loosen is very low. Therefore, an outside influence, such as the application of insufficient
torque to the nuts during maintenance, likely occurred. The Safety Board reviewed Air
Sunshine’s maintenance records to determine when insufficient torque might have been
applied to the nuts.
Between the time of the last compression checks (June 12 to 14, 2003) and the
accident, the engine accumulated 83 flight hours. No records were found indicating that
any other maintenance was performed on the accident engine at the time of and after the
last compression check. Although it is possible that insufficient torque was applied to the
cylinder hold-down nuts during undocumented maintenance at the time of the last known

Analysis 41 Aircraft Accident Report
maintenance event,
71
it is also possible that insufficient torque was applied during
undocumented maintenance subsequent to the last known event. However, if a mechanic
does not apply enough torque to a nut during maintenance, the nut typically becomes loose
soon afterward. Therefore, the Safety Board concludes that the simultaneous loosening of
two or more of the right engine No. 2 cylinder hold-down nuts resulted from the
application of insufficient torque, which was applied by Air Sunshine maintenance
personnel during undocumented maintenance.
2.6 Air Sunshine Maintenance Record-Keeping and
Practices
The Safety Board’s review of Air Sunshine’s maintenance records revealed several
discrepancies. The review revealed that the number stamped on the No. 6 cylinder from
the accident airplane’s right engine did not match the number recorded in the maintenance
records. The maintenance records for the right engine did not indicate that the No. 6
cylinder had ever been removed or replaced. Further, although the company’s General
Manager reported that the No. 6 cylinder was originally the No. 3 cylinder from another
one of the company’s engines, the maintenance records for the other engine did not
indicate that its No. 3 cylinder had ever been removed or replaced. Air Sunshine’s records
showed no evidence that the company had reported any problems with its engine to the
FAA
72
despite evidence found during this investigation that indicated that at least two
cylinders were removed and replaced on two separate engines.
In 1998, Air Sunshine applied to change its AAIP from a 3-phase, 60-hour
inspection program to a 6-phase, 60-hour inspection program. The FAA approved the
change, which was in effect at the time of the accident. As a result of this change, engine
differential compression checks were conducted once every 360 hours instead of every
180 hours. Subsequent to the accident, Air Sunshine changed its AAIP to require that
three compression checks be conducted during a 360-hour inspection cycle (once every
120 hours), and the FAA approved this change. Although the company’s modified AAIP
increased the number of compression checks in a 360-hour cycle, the compression check
interval is still well beyond the 100-hour interval recommended in SB 03-3.
In addition, during the last differential compression checks performed on the
airplane’s engines (from June 12 to 14, 2003), the assistant mechanic recorded readings of
0 psi for the right engine No. 2 cylinder and 20 psi for the No. 4 cylinder. Further, Safety
Board investigators who reviewed the engine differential compression check form on
which the assistant mechanic recorded the readings noted that the number recorded for the
71
Typically, torque only needs to be applied to cylinder hold-down nuts after cylinder installations.
Cylinders are not removed and reinstalled during compression checks; therefore, insufficient torque would
not have been applied during the June 2003 compression checks.
72
As noted previously, in a September 9, 1999, letter to Air Sunshine, the PMI stated that he would
grant the company’s request to amend its operations specifications to reflect the 2,400-flight-hour TBO if
the company monitored the performance of newly overhauled engines and reported any abnormal conditions
to the San Juan FSDO.

Analysis 42 Aircraft Accident Report
No. 3 cylinder could have been either 55 or 25. The Director of Maintenance told Safety
Board investigators that, because the readings were low, he repeated the checks on all of
the right engine cylinders. He stated that all of the readings were in the 70-psi range.
However, Board investigators could not find any documentation indicating that the checks
had been repeated.
The differential compression checks on the right engine were performed by an
assistant mechanic without supervision or assistance, even though he did not have an A&P
certificate. During postaccident interviews, the assistant mechanic stated that he had never
conducted a compression check before conducting the checks on the accident airplane’s
right engine. When a Safety Board investigator asked the assistant how to perform the test,
he did not appear to be familiar with the entire test. Further, Air Sunshine’s Maintenance
Manual contained a caution, stating that two people should conduct the compression checks.
The Safety Board notes that, for the compression checks to be conducted safely and
properly, the two people who conduct the checks should have adequate training and
experience. However, Air Sunshine’s Director of Maintenance allowed a non-A&P
certified assistant mechanic, who had never previously performed engine compression
checks, to perform the checks by himself without supervision. Further, a review of the
assistant mechanic’s training records indicated that he did not complete on-the-job training
for the entire airplane until 14 to 16 days after he performed the compression checks. The
assistant mechanic should not have been working unsupervised during on-the-job training,
which indicated that the company’s on-the-job maintenance training was not adequate.
Last, during postaccident interviews, the Director of Maintenance stated that,
when company maintenance personnel remove and replace an engine cylinder assembly,
they coat the cylinder hold-down studs with an aluminum-copper-graphite, lithium-based
antiseize compound manufactured by Permatex before applying torque to the studs. The
use of the Permatex compound is not in accordance with TCM SB 96-7B. Permatex does
not recommend using antiseize compound in high-vibration environments because it
could contribute to the loss of torque. Although the threads of the right engine studs and
through bolts showed no evidence of this compound, the Safety Board is concerned that
Air Sunshine indicated that it was using an antiseize compound on its engines. The Safety
Board concludes that, at the time of the accident, Air Sunshine’s maintenance
record-keeping and practices were not adequate.
Subsequent to the accident, the FAA conducted a focused inspection of Air
Sunshine (from July 22 to August 29, 2003). During these inspections, the FAA
determined that the company’s maintenance program was deficient. The FAA stated that it
had sent a letter to Air Sunshine in which all of the maintenance discrepancies were
addressed and that all of the company’s corrective actions in response to these
discrepancies had been documented in the FAA’s PTRS. Therefore, the Safety Board
concludes that the FAA’s oversight of Air Sunshine was in accordance with standard
guidelines, but was insufficient to detect inadequate maintenance record-keeping and
practices at the company.

Analysis 43 Aircraft Accident Report
2.7 Pilot Proficiency
A review of Arrow Air’s simulator training records for the pilot revealed that he
had received a large number of “unsatisfactory” grades and that he needed to improve his
scanning and checklist skills, including response and organization.
73
Further, on
September 13, 2000, the pilot failed a ramp check because an FAA inspector found that
the airplane had numerous discrepancies and that his passenger briefing was inadequate.
Airplane performance calculations show that the windmilling propeller and the
protruding magnetos alone were not sufficient to cause the airplane to descend as rapidly
as it did. Other factors that were most likely caused or controlled by the pilot, including
not flying at the recommended airspeeds and flap settings, operating with a bank angle and
sideslip that were not in accordance with Cessna’s recommended in-flight engine failure
configuration, and not maintaining a steady descent, could have degraded the accident
airplane’s performance. If the pilot had been more proficient, he might have been able to
decrease the descent rate enough to maintain flight and reach land.
A review of FAA records revealed that, from April 1983 to February 1998, the
pilot failed nine flight checks. The pilot failed two flight checks that he was receiving for
his private pilot certificate, one flight check that he was receiving for his instrument pilot
rating, one flight check that he was receiving for his ATP certificate, two flight checks that
he was receiving for his CFI certificate, and three flight checks that he was receiving for
his CFI instrument rating.
Therefore, the Safety Board concludes that the pilot had a history of
below-average flight proficiency, including numerous failed flight tests, before the
accident flight, which contributed to his inability to maintain maximum flight
performance and reach land after the right engine failed.
2.8 Pilot Failure to Use Shoulder Harness
Federal regulations require flight crewmembers of U.S.-registered civil aircraft to
keep their shoulder harnesses fastened during takeoff and landing, including during a
ditching. During postaccident interviews, the pilot stated that he did not have his shoulder
harness fastened during the ditching. He added that, because his harness was not fastened,
he hit his head on the instrument panel when the airplane hit the water, which made him
dizzy. Two passengers indicated that the pilot was incoherent when he was in the water.
One of the passengers also stated that the pilot “did not look like he could swim” and that
he had to give the pilot his PFD. Therefore, the Safety Board concludes that the pilot was
not wearing his shoulder harness during the ditching, and, because he was not wearing his
harness, he sustained a head injury that reduced his ability to assist passengers after the
ditching.
73
The pilot did not complete Arrow Air’s pilot training program.

Analysis 44 Aircraft Accident Report
2.9 Emergency Briefings
Air Sunshine’s FAA-approved General Operations Manual stated that, before a
ditching, the pilot should review the emergency ditching evacuation procedures with the
passengers and instruct them to don their PFDs without inflating them in the airplane. The
manual added that the pilot should also review with the passengers how to operate the
PFDs. Because these instructions were also contained in the company’s operations
specifications, the instructions were required to be performed by the pilot.
In a 1985 safety study titled, Air Carrier Overwater Emergency Equipment and
Procedures,
74
the Safety Board concluded that “the ability of flight and cabin
crewmembers to assist passengers effectively during ditchings and following inadvertent
water impacts may be the single most important factor in the survival outcome.” As noted
previously, passengers reported that, after the right engine failed, the pilot did not tell them
to retrieve or don their PFDs before the airplane contacted the water. The passengers
stated that the only time the pilot addressed them after the right engine failed and before
the airplane contacted the water was to tell them to “calm down.”
According to the Safety Board’s airplane performance study, the airplane was
airborne for at least 7 minutes after the right engine failed and before it contacted the
water. Even though the pilot did not instruct the passengers to retrieve their PFDs, the
passenger in seat 3B, who was holding a child on her lap, retrieved the PFD from under
her seat, and the passenger in seat 5A retrieved three PFDs and put them on the children
accompanying her. None of the other passengers or the pilot attempted to retrieve their
PFDs before the airplane contacted the water. After the airplane was in the water, several
of these passengers tried to retrieve their PFDs, but none was successful.
If the pilot had instructed the adult passengers to retrieve and don their PFDs and
had reviewed how to operate the PFDs shortly after the right engine failed, all of the
passengers would have had adequate time to retrieve and don their PFDs before the
airplane contacted the water. The Safety Board is aware that, subsequent to the accident,
Air Sunshine amended its emergency ditching procedures by adding the instruction that all
occupants should don PFDs as soon as any emergency occurs during overwater
operations.
The Safety Board concludes that, after determining that he was going to ditch the
airplane, the pilot failed to conduct an emergency briefing, which was required by the
emergency ditching procedures contained in Air Sunshine’s General Operations Manual,
and that this failure contributed to passenger fatalities. The Safety Board further concludes
that the passengers would have had sufficient time to retrieve and don their PFDs if the
pilot had instructed them to do so shortly after the right engine failed.
74
For more information, see National Transportation Safety Board, Air Carrier Overwater Emergency
Equipment and Procedures, Safety Study NTSB/SS-85/02 (Washington, DC: NTSB, 1985).

Analysis 45 Aircraft Accident Report
On January 1, 2002, a Piper PA-31 operated by Air Taxi, Inc., was ditched in the
Atlantic Ocean after fuel exhaustion. Three passengers and the pilot sustained serious
injuries, and one passenger died. According to the surviving passengers, the pilot did not
conduct a preflight briefing or an emergency briefing before the ditching. None of the
PFDs on board the airplane were retrieved until the airplane was in the water.
In contrast, on August 20, 2000, a Piper PA-31 operated by Big Island Air was
ditched in the Pacific Ocean after a loss of engine power. All of the passengers retrieved
their PFDs before the ditching. The passengers reported that, shortly after the engine
problem occurred, the pilot instructed them to retrieve and don their PFDs and assume a
crash position. As indicated by this event, if passengers aboard flights that operate over
water are adequately briefed and have time to prepare during an emergency, deaths may be
prevented.
The Safety Board concludes that having pilots provide adequate emergency
briefings to passengers is an important survival factor. Therefore, the Safety Board
believes that the FAA should issue a flight standards information bulletin to principal
operations inspectors of all Part 135 single-pilot operators that carry passengers and
operate over water, which familiarizes them with the circumstances of the Air Sunshine
flight 527 accident and emphasizes the need for pilots to provide timely emergency
briefings. The bulletin should state that these briefings should include, at a minimum,
information about the location and operation of the on-board emergency equipment and
exits.

46 Aircraft Accident Report
3. Conclusions
3.1 Findings
1. The pilot was properly certificated and qualified under Federal regulations. No
evidence indicated any preexisting medical or physical condition that might have
adversely affected the pilot’s performance during the accident flight.
2. The airplane was properly certificated and equipped in accordance with Federal
regulations. The airplane was equipped with Federal Aviation
Administration-approved flotation gear, as required by Federal regulations.
3. The accident airplane was loaded in accordance with Federal Aviation
Administration-approved company weight and balance procedures. The weight and
balance of the airplane were within prescribed limits during all phases of the flight.
4. Given the distance from shore at which the ditching occurred and the availability of
emergency response equipment, the search and rescue efforts were timely and
appropriate. The accident was survivable.
5. The inoperative distance measuring equipment on the Treasure Cay Airport very high
frequency omnidirectional range was not a factor in this accident.
6. The airplane’s right engine failed while the airplane was descending through an
altitude of about 3,500 feet.
7. Several factors contributed to the degradation of the airplane’s performance and its
inability to maintain flight and reach land, including the windmilling propeller, the
protruding magnetos, the open right engine cowl flap, and the possibility that the flaps
were extended to 15° at some point during the descent.
8. During the descent from 3,500 to 2,000 feet, the airplane’s descent rate was between
about 560 and 212 feet per minute (fpm), and, during the descent from 2,000 feet to
contact with the water, its descent rate was between 429 and 360 fpm.
9. If the average descent rate had been about 200 feet per minute or less, the airplane
would have been able to maintain flight and reach Treasure Cay Airport.
10. The right propeller was in the fully feathered position, but Safety Board investigators
could not determine at what point the propeller became fully feathered.
11. Two or more of the right engine No. 2 cylinder hold-down nuts became loose and
backed off of the studs, which resulted in the remaining studs and through bolts
fracturing in high-stress fatigue, allowing the cylinder to separate from the engine.

Conclusions 47 Aircraft Accident Report
12. The simultaneous loosening of two or more of the right engine No. 2 cylinder
hold-down nuts resulted from the application of insufficient torque, which was
applied by Air Sunshine maintenance personnel during undocumented maintenance.
13. At the time of the accident, Air Sunshine’s maintenance record-keeping and practices
were not adequate.
14. The Federal Aviation Administration’s oversight of Air Sunshine was in accordance
with standard guidelines, but was insufficient to detect inadequate maintenance
record-keeping and practices at the company.
15. The pilot had a history of below-average flight proficiency, including numerous failed
flight tests, before the accident flight, which contributed to his inability to maintain
maximum flight performance and reach land after the right engine failed.
16. The pilot was not wearing his shoulder harness during the ditching, and because he
was not wearing his harness, he sustained a head injury that reduced his ability to
assist passengers after the ditching.
17. After determining that he was going to ditch the airplane, the pilot failed to conduct
an emergency briefing, which was required by the emergency ditching procedures
contained in Air Sunshine’s General Operations Manual, and this failure contributed
to passenger fatalities.
18. The passengers would have had sufficient time to retrieve and don their personal
flotation devices if the pilot had instructed them to do so shortly after the right engine
failed.
19. Having pilots provide adequate emergency briefings to passengers is an important
survival factor.
3.2 Probable Cause
The National Transportation Safety Board determines that the probable cause of
this accident was the in-flight failure of the right engine and the pilot’s failure to
adequately manage the airplane’s performance after the engine failed. The right engine
failure resulted from inadequate maintenance that was performed by Air Sunshine’s
maintenance personnel during undocumented maintenance. Contributing to the passenger
fatalities was the pilot’s failure to provide an emergency briefing after the right engine
failed.

48 Aircraft Accident Report
4. Recommendation
As a result of its investigation of the July 13, 2003, Air Sunshine flight 527
accident, the National Transportation Safety Board makes the following recommendation
to the Federal Aviation Administration:
Issue a flight standards information bulletin to principal operations
inspectors of all Part 135 single-pilot operators that carry passengers and
operate over water, which familiarizes them with the circumstances of the
Air Sunshine flight 527 accident and emphasizes the need for pilots to
provide timely emergency briefings. The bulletin should state that these
briefings should include, at a minimum, information about the location and
operation of the on-board emergency equipment and exits. (A-04-55)
BY THE NATIONAL TRANSPORTATION SAFETY BOARD
ELLEN ENGLEMAN CONNERS
Chairman
CAROL J. CARMODY
Member
MARK V. ROSENKER
Vice Chairman
RICHARD F. HEALING
Member
DEBORAH A. P. HERSMAN
Member
Adopted: October 13, 2004

49 Aircraft Accident Report
5. Appendix
Appendix A
Investigation and Public Hearing
Investigation
The National Transportation Safety Board learned about the accident about 1545
on July 13, 2003. A go-team was not assembled, and the Safety Board did not immediately
respond to the scene of the accident. An Air Safety Investigator from the Board’s Southeast
Regional Field Office departed Miami on July 31, 2003, to observe the recovery of the
airplane, which occurred on August 3, 2003, about 1120. Investigators from Cessna Aircraft
Company and the Federal Aviation Administration (FAA) were also present during the
recovery.
Parties to the investigation were the FAA, Teledyne Continental Motors, McCauley
Propeller Systems, and Cessna Aircraft Company. The Bahamian Government designated
an accredited representative to assist in the investigation.
Public Hearing
No public hearing was held for this accident.

this page intentionally left blank
