Panniculectomy and Body Contouring Procedures
Page 1 of 11
UnitedHealthcare Commercial and Individual Exchange Medical Policy
Effective 07/01/2024
Proprietary Information of UnitedHealthcare. Copyright 2024 United HealthCare Services, Inc.
UnitedHealthcare
®
Commercial and Individual Exchange
Medical
Policy
Panniculectomy and Body Contouring Procedures
Policy Number: MP.014.23
Effective Date: July 1, 2024
Instructions for Use
Table of Contents Page
Application ............................................................................. 1
Coverage Rationale .............................................................. 1
Documentation Requirements ............................................... 2
Definitions .............................................................................. 2
Applicable Codes .................................................................. 3
Description of Services ......................................................... 3
Clinical Evidence ................................................................... 3
U.S. Food and Drug Administration ...................................... 9
References ............................................................................ 9
Policy History/Revision Information .................................... 10
Instructions for Use ............................................................. 10
Application
UnitedHealthcare Commercial
This Medical Policy applies to all UnitedHealthcare Commercial benefit plans.
UnitedHealthcare Individual Exchange
This Medical Policy applies to Individual Exchange benefit plans in all states except for Colorado.
Coverage Rationale
Panniculectomy
Panniculectomy is considered reconstructive and medically necessary in certain circumstances. For medical
necessity clinical coverage criteria, refer to the InterQual
®
CP: Procedures, Panniculectomy, Abdominal.
Click here to view the InterQual
®
criteria.
Panniculectomy is considered cosmetic and not medically necessary when performed for the following
indications:
• For any other condition that does not meet the InterQual
®
criteria
• In conjunction with abdominal or gynecologic surgery, including but not limited to hernia repair, bariatric surgery, C-
section, or hysterectomy, unless the member meets the InterQual
®
CP: Procedures, Panniculectomy, Abdominal
criteria
• When performed for primarily cosmetic purposes
Body Contouring Procedures
Body contouring procedures, including but not limited to the following, are considered cosmetic and not
medically necessary:
• Abdominoplasty
• Lipectomy, including Suction-Assisted Lipectomy (unless part of an approved procedure); for post-mastectomy, refer
to the Medical Policy titled Breast Reconstruction
• Repair of Diastasis Recti
Related Commercial/Individual Exchange Policies
• Breast Reconstruction
• Cosmetic and Reconstructive Procedures
• Gender Dysphoria Treatment
• Liposuction for Lipedema
•
Omnibus Codes
Community Plan Policy
• Panniculectomy and Body Contouring Procedures
Medicare Advantage Policy
• Cosmetic and Reconstructive Procedures

Panniculectomy and Body Contouring Procedures
Page 2 of 11
UnitedHealthcare Commercial and Individual Exchange Medical Policy
Effective 07/01/2024
Proprietary Information of UnitedHealthcare. Copyright 2024 United HealthCare Services, Inc.
Note: For information on liposuction for lipedema, refer to the Medical Policy titled Liposuction for Lipedema.
Documentation Requirements
Benefit coverage for health services is determined by the member specific benefit plan document and applicable laws that
may require coverage for a specific service. The documentation requirements outlined below are used to assess whether
the member meets the clinical criteria for coverage but do not guarantee coverage of the service requested.
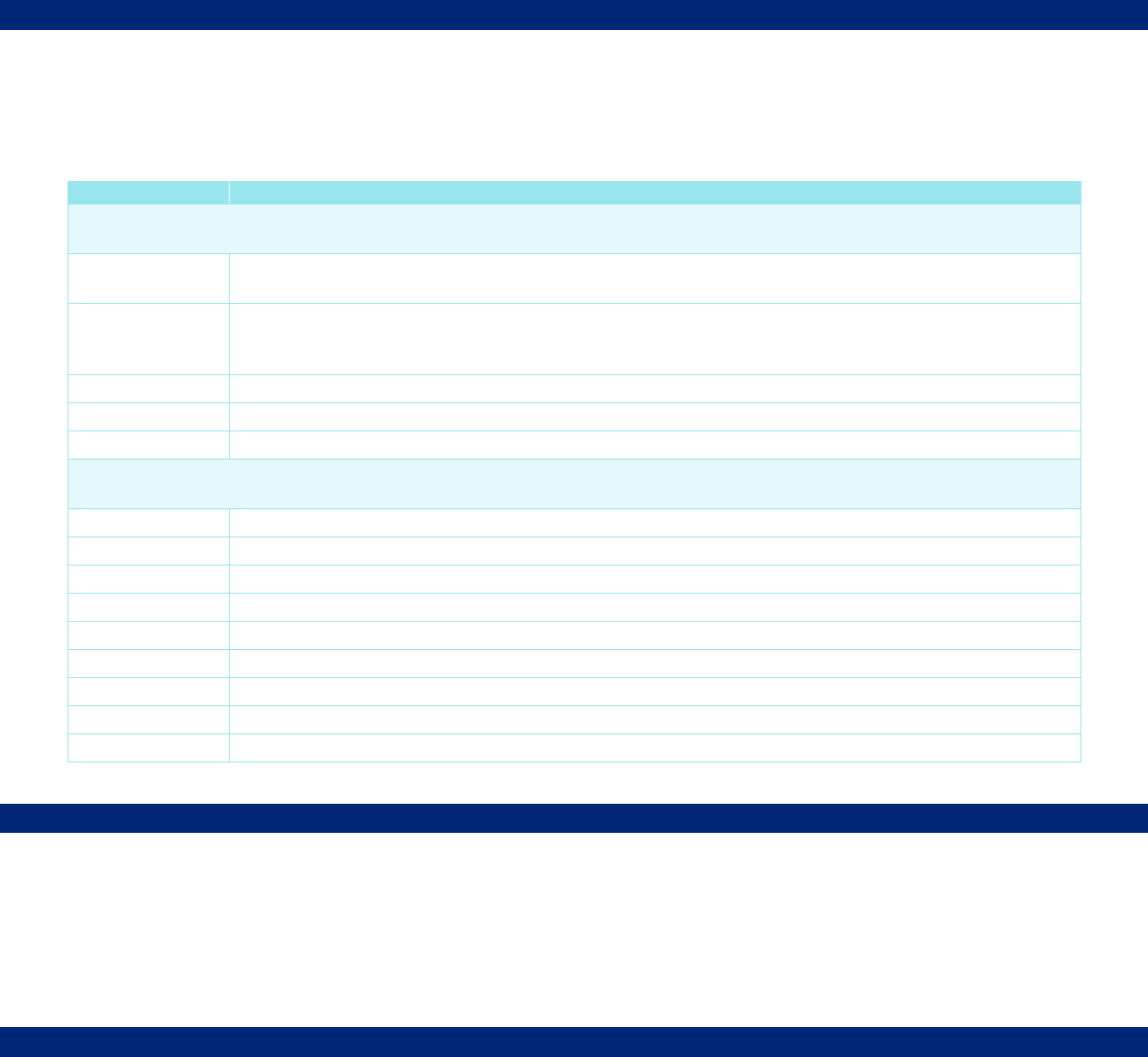
CPT Codes*
Required Clinical Information
Panniculectomy and Body Contouring Procedures
15830
15847
15877
15878
15879
Medical notes documenting the following, when applicable:
• Primary complaint, history of complaint, and physical exam, including:
o Grade of panniculus
o Body mass index (BMI)
o History of recent weight loss in lbs/kgs
o History of weight stability and duration
o History of dermatologic complications
• Diagnosis of dermatologic complications (e.g., skin infection, ulcers, maceration, skin
breakdown, etc.)
• Treatments (e.g., antibiotic, corticosteroid, antifungal) for dermatologic complications tried,
failed, or contraindicated; include the dates, duration of treatment, and reason for
discontinuation
• Details of functional limitations due to pannus interfering with activities of daily living (ADL)
• Relevant surgical history, including dates
• Physician treatment plan, including specific and associated procedures
• Upon request we may require high-quality color photographs
o For panniculectomy, photographs of a full-frontal view of the hanging pannus, a full-frontal
view of pannus elevated that allows for the evaluation of any skin damage, and a full lateral
view of the hanging pannus
o All photographs must be labeled with the date taken and the applicable case number
obtained at time of notification, or member’s name and ID number on the photograph(s)
o Note: Submission of color photographs can be submitted via the external portal at
www.uhcprovider.com/paan; faxes of color photographs will not be accepted
*For code descriptions, refer to the Applicable Codes section.
Definitions
The following definitions may not apply to all plans. Refer to the member specific benefit plan document for applicable
definitions.
Abdominoplasty: Typically performed for cosmetic purposes, involves the removal of excess skin and fat from the pubis
to the umbilicus or above, and may include fascial plication of the rectus muscle diastasis and a neoumbilicoplasty (ASPS,
2017).
Diastasis Recti: A vertical abnormal separation of the rectus abdominis muscles (Olsson et al., 2021).
Functional or Physical or Physiological Impairment: A Functional or Physical or Physiological Impairment causes
deviation from the normal function of a tissue or organ. This results in a significantly limited, impaired, or delayed capacity
to move, coordinate actions, or perform physical activities and is exhibited by difficulties in one or more of the following
areas: physical and motor tasks; independent movement; performing basic life functions (Medicare, 2023).
Panniculectomy: Involves the removal of hanging excess skin/fat in a transverse or vertical wedge but does not include
muscle plication, neoumbilicoplasty or flap elevation. A cosmetic Abdominoplasty is sometimes performed at the time of a
functional Panniculectomy (ASPS, 2017).
Suction-Assisted Lipectomy: Suction-Assisted Lipectomy (SAL), more commonly known as Liposuction, is an outpatient
procedure that removes adipose tissue from the subcutaneous space with the goal of achieving a more desirable body
contour (Wu et al., 2020).
Panniculectomy and Body Contouring Procedures
Page 3 of 11
UnitedHealthcare Commercial and Individual Exchange Medical Policy
Effective 07/01/2024
Proprietary Information of UnitedHealthcare. Copyright 2024 United HealthCare Services, Inc.
Applicable Codes
The following list(s) of procedure and/or diagnosis codes is provided for reference purposes only and may not be all
inclusive. Listing of a code in this policy does not imply that the service described by the code is a covered or non-covered
health service. Benefit coverage for health services is determined by the member specific benefit plan document and
applicable laws that may require coverage for a specific service. The inclusion of a code does not imply any right to
reimbursement or guarantee claim payment. Other Policies and Guidelines may apply.
CPT Code
Description
The following codes may be cosmetic; review is required to determine if considered cosmetic or
reconstructive.
15830
Excision, excessive skin and subcutaneous tissue (includes lipectomy); abdomen, infraumbilical
panniculectomy
15847
Excision, excessive skin and subcutaneous tissue (includes lipectomy), abdomen (e.g.,
abdominoplasty) (includes umbilical transposition and fascial plication) (List separately in addition to
code for primary procedure)
15877
Suction assisted lipectomy; trunk
15878
Suction assisted lipectomy; upper extremity
15879
Suction assisted lipectomy; lower extremity
The following codes are considered cosmetic; the codes do not improve a functional, physical, or
physiological impairment.
15832
Excision, excessive skin and subcutaneous tissue (includes lipectomy); thigh
15833
Excision, excessive skin and subcutaneous tissue (includes lipectomy); leg
15834
Excision, excessive skin and subcutaneous tissue (includes lipectomy); hip
15835
Excision, excessive skin and subcutaneous tissue (includes lipectomy); buttock
15836
Excision, excessive skin and subcutaneous tissue (includes lipectomy); arm
15837
Excision, excessive skin and subcutaneous tissue (includes lipectomy); forearm or hand
15838
Excision, excessive skin and subcutaneous tissue (includes lipectomy); submental fat pad
15839
Excision, excessive skin and subcutaneous tissue (includes lipectomy); other area
15876
Suction assisted lipectomy; head and neck
CPT
®
is a registered trademark of the American Medical Association
Description of Services
An abdominal panniculus is an apron of skin and fat that hangs down from the abdomen. This often occurs following
massive weight loss and can lead to skin infections, rashes, and difficulty completing activities of daily living (Sachs et al.,
2021). A Panniculectomy is a surgery that removes this excess skin and fat but typically does not involve the abdominal
muscles (ASPS, 2017).
Body contouring is a collection of procedures to change the shape of the body. Adipose tissue is usually removed, with or
without removal of excess skin. Body contouring procedures can be either invasive or nonsurgical.
Clinical Evidence
Panniculectomy
There is insufficient quality evidence to conclude that panniculectomy in conjunction with abdominal or gynecological
surgery, including, but not limited to, hernia repair, bariatric surgery, C-section, or hysterectomy, outweighs negative
outcomes. Additional peer-reviewed literature is needed to determine if there are any long-term benefits and that the
benefits outweigh the risks when panniculectomy is performed at the same time.
Elhage et al. (2021) evaluated the outcomes and quality of life (QOL) in patients undergoing complex abdominal wall
reconstruction (AWR) with panniculectomy utilizing 3D volumetric-based propensity match in a prospective cohort study.
A prospective database from a tertiary referral hernia center was queried for patients undergoing open AWR. 3D CT
volumetrics were analyzed and a propensity match comparing AWR patients with and without panniculectomy was
Panniculectomy and Body Contouring Procedures
Page 4 of 11
UnitedHealthcare Commercial and Individual Exchange Medical Policy
Effective 07/01/2024
Proprietary Information of UnitedHealthcare. Copyright 2024 United HealthCare Services, Inc.
created including subcutaneous fat volume (SFV). QOL was analyzed using the Carolinas Comfort Scale. Propensity
match yielded 312 pairs, all with adequate CT imaging for volumetric analysis. The panniculectomy group had a higher
BMI (p = 0.03) and were more likely female (p < 0.0001), but all other demographics and comorbidities were similar. The
panniculectomy group was more likely to have undergone prior hernia repair (77% vs 64%, p < 0.001), but hernia area,
SFV, and CDC wound class were similar (all p > 0.05). Requirement of component separation (61% vs 50%, p = 0.01)
and mesh excision (44% vs 35%, p = 0.02) were higher in the panniculectomy group, but operative time were similar (all p
≥ 0.05). Panniculectomy patients had a higher overall wound occurrence rate (45% vs 32%, p = 0.002) which was
differentiated only by a higher rate of wound breakdown (24% vs 14%, p = 0.003); all other specific wound complications
were equal (all p ≥ 0.05). Hernia recurrence rates were similar (8% vs 9%, p = 0.65) with an average follow-up of 28
months. Overall QOL was equal at 2 weeks, and 1, 6, and 12 months (all p ≥ 0.05). The authors concluded that despite
panniculectomy patients and their hernias being more complex, concomitant panniculectomy increased wound
complications but did not negatively impact infection rates or long-term outcomes and recommended concomitant
panniculectomy be considered in appropriate patients to avoid two procedures.
In a retrospective cohort study, Gebran et al. (2021) evaluated the risk profile of panniculectomy when performed in select
patients at the time of bariatric surgery. The Metabolic and Bariatric Surgery Accreditation and Quality Improvement
Program (MBSAQIP) database (2016-2017), in which data on 379,544 bariatric surgeries were reported was examined.
Concurrent panniculectomy procedures were identified by Current Procedural Technology (CPT) codes. Patient
characteristics and in-hospital as well as 30-day complications were compared between the body contouring group and
propensity score-matched bariatric surgery controls. One hundred twenty-four patients met inclusion criteria and were
matched to 248 controls. An infra-umbilical panniculectomy was performed in the majority of patients (n = 94, 75.8%).
Most patients received an open rather than laparoscopic bariatric surgery (n = 87, 70.2%). There were no statistically
significant differences between 30-day mortality (1.9%), wound complications (11.5%), readmission (12.5%) and
reoperation (5.8%) between the 2 groups (p > .05). Wound complications occurred in 11.5% of patients and were
associated with prolonged hospital stay (odds ratio 4.65, 95% confidence interval 1.99–10.86, p < .001) and a body mass
index (BMI) > 50 (odds ratio 3.19, 95% confidence interval 1.02–9.96, p = .046). The authors concluded, in select
patients, panniculectomy at the time of bariatric surgery was not associated with increased in-hospital or 30-day adverse
outcomes compared with matched bariatric surgery controls, however, revision surgery may be needed once weight loss
stabilizes. The study was limited by database limitations, short-term follow up, and multiple outcome variables.
Nag et al. (2021) performed a retrospective cohort study and systematic review to evaluate the premise that the addition
of panniculectomy to gynecologic surgery in the obese and morbidly obese patient population results in a statistically
significant improvement in measurable outcomes. The American College of Surgeons National Surgical Quality
Improvement Program (NSQIP) database was reviewed to assess the association of complications with panniculectomy
combined with gynecologic surgery in the morbidly obese patient population. The query identified 296 patients with a BMI
greater than 30 who had panniculectomy concomitant with gynecologic surgery. The results demonstrated a statistically
significant relationship (p < 0.05) of these concomitant procedures with superficial infection, wound infection, pulmonary
embolism, systemic sepsis, return to operating room, length of operation and length of stay. A systematic review of the
literature was then performed which identified only 5 studies that included comparative cohorts of those with gynecologic
surgery, with and without panniculectomy. There was no significant benefit across the studies in measured parameters.
The authors concluded that there was no statistically significant benefit associated with performing panniculectomy in
conjunction with gynecologic surgery in the morbidly obese patient population and that there was significant elevation of
negative outcomes in morbidly obese patients undergoing combined procedures.
In a systematic meta-analysis, Prodromidou et al. (2020) assessed the current knowledge concerning the safety and
efficacy of combining panniculectomy in surgical management of endometrial cancer (EC) in obese patients. Four
electronic databases were systematically searched for articles published up to May 2019. A total of five studies, of which
two were non-comparative and three comparative, were included. Meta-analysis of complications among panniculectomy
and conventional laparotomy group revealed no difference in either intra- or post-operative complication rates. Moreover,
no difference was reported in surgical site complications (p = 0.59), while wound breakdown rates were significantly
elevated in the laparotomy group (p = 0.02). The authors concluded panniculectomy combined surgery for the
management of EC can be considered a safe procedure in selected patients and presents with comparable outcomes to
conventional laparotomy procedures with regard to non-surgical and surgical site complications and improved wound
breakdown rates. The authors noted that the outcomes must be cautiously interpreted because of the limited number of
studies included in this meta-analysis and their retrospective nature.
Sosin et al. (2020) conducted a systematic meta-analysis to assess the durability, complication profile, and safety of
simultaneous ventral hernia repair and panniculectomy (SVHRP) through a large data-driven repository of SVHRP cases.
The current SVHRP literature was queried using the MEDLINE, PubMed, and Cochrane databases. Predefined selection
criteria resulted in 76 relevant titles yielding 16 articles for analysis. Meta-analysis was used to analyze primary outcomes,
Panniculectomy and Body Contouring Procedures
Page 5 of 11
UnitedHealthcare Commercial and Individual Exchange Medical Policy
Effective 07/01/2024
Proprietary Information of UnitedHealthcare. Copyright 2024 United HealthCare Services, Inc.
identified as surgical-site occurrence and hernia recurrence. Secondary outcomes included review of techniques used and
systemic complications, which were analyzed with pooled weighted mean analysis from the collected data. There were
917 patients who underwent an SVHRP (mean age, 52.2 ±7.0 years; mean BMI, 36.1 ±5.8 kg/m; mean pannus weight,
3.2 kg). The mean surgical-site occurrence rate was 27.9% (95% CI, 15.6 to 40.2%; I = 70.9%) and the mean hernia
recurrence rate was 4.9% (95% CI, 2.4 to 7.3%; I = 70.1%). Mean follow-up was 17.8 ±7.7 months. The most common
complications were superficial surgical-site infection (15.8%) and seroma formation (11.2%). Systemic complications were
less common (7.8%), with a thromboembolic event rate of 1.2%. The overall mortality rate was 0.4%. The authors
concluded SVHRP is associated with a high rate of surgical-site occurrence, but surgical-site infection seems to be less
prominent than previously anticipated. The authors indicated the low hernia recurrence rate and the safety of this
procedure support its current implementation in abdominal wall reconstruction. (McNichols et al., 2018 is included in this
review)
In a retrospective cohort study, Diaconu et al. (2019) compared outcomes in obese patients who undergo ventral hernia
repair with concurrent panniculectomy versus ventral hernia repair alone. Postoperative complications were compared
between patient who underwent concurrent panniculectomy and those who did not. A total of 223 patients were analyzed:
122 in the ventral hernia repair with concurrent panniculectomy group and 101 in the ventral hernia repair-only group.
Median follow-up duration was 141 days. Patients in the ventral hernia repair with concurrent panniculectomy group had
more surgical-site occurrences (57 percent versus 40 percent; p = 0.012). Both groups had similar rates of surgical-site
occurrences that required an intervention (39 percent versus 31 percent; p = 0.179) and similar rates of hernia recurrence
(23 percent versus 29 percent; p = 0.326). Multivariate analysis showed that concurrent panniculectomy increased the risk
of surgical-site occurrences by two-fold; however, it did not increase the risk of surgical-site occurrences that required an
intervention. The authors concluded the addition of a panniculectomy to ventral hernia repair increases surgical-site
occurrences but does not increase complications that require an intervention.
Fennimore et al. (2015) conducted a retrospective cohort study to determine whether a modified abdominal
panniculectomy at the time of cesarean delivery decreases wound complications in morbidly obese women. The study
included 59 morbidly obese patients who delivered via cesarean section at a single center between 2003 and 2009. A
total of 30 morbidly obese patients who underwent modified panniculectomy at the time of cesarean section were
compared to a control group of 29 morbidly obese women who underwent cesarean section alone. Of the 30 women who
underwent modified panniculectomy at the time of cesarean, 3% (n = 1) developed operative site infection that required
readmission. In the control group, 24% (n = 7) developed operative site infection (p = 0.026), and 10% (n = 3) were
readmitted (p = 0.35). There was no difference in the postpartum length of hospital stay, intraoperative blood loss,
operative time, and infant delivery time between the two groups. In the cohort, morbidly obese women who underwent
panniculectomy at the time of cesarean section had lower incidence of wound complications without significant increase in
operative time, hospital length of stay, and infant delivery time. The authors concluded modified panniculectomy at the
time of cesarean may be a useful adjunct in an effort to decrease postoperative infectious morbidity in obese patients,
however, the effects of the procedure on long-term healing, future obstetric outcomes, and other medical conditions
warrant further evaluation.
Clinical Practice Guidelines
American Society of Plastic Surgeons (ASPS)
ASPS (2019) recommends when an abdominoplasty or panniculectomy are performed solely to enhance a patient's
appearance in the absence of any signs or symptoms of functional abnormalities, the procedure should be considered
cosmetic in nature and not a compensable procedure unless specified in the patient's policy. ASPS further recommends
that a panniculectomy should be considered a reconstructive procedure when performed to correct or relieve structural
defects of the abdominal wall, improve skin health within the fold beneath the pannus, and/or help improve chronic low
back pain due to functional incompetence of the anterior abdominal wall. In rare circumstances, plastic surgeons may
perform a hernia repair in conjunction with an abdominoplasty or panniculectomy. A true hernia repair involves opening
fascia and/or dissection of a hernia sac with return of intraperitoneal contents back to the peritoneal cavity. A true hernia
repair should not be confused with diastasis recti repair, which is often part of a standard abdominoplasty.
In a practice parameter, ASPS (2017) noted panniculectomy could be considered as a functional correction in patients
who are of appropriate height and weight, and have a history of problems including panniculitis or chronic back pain that
have persisted despite an adequate trial of non-surgical management, or have a functional impairment in activities of daily
living/work, etc. ASPS notes a strong relationship between increased BMI and surgical complication across the surgical
spectrum. Acarturk et al. (2004) retrospectively compared the surgical outcomes of 21 patients that had simultaneous
panniculectomy and bariatric surgery to 102 patients that delayed panniculectomy following bariatric surgery by a mean of
17 months. Those who had simultaneous surgery had significantly more complications and higher mortality.
Panniculectomy and Body Contouring Procedures
Page 6 of 11
UnitedHealthcare Commercial and Individual Exchange Medical Policy
Effective 07/01/2024
Proprietary Information of UnitedHealthcare. Copyright 2024 United HealthCare Services, Inc.
Society of Obstetricians and Gynaecologists of Canada (SOGC)
SOGC clinical practice guideline for gynecologic surgery for patients with obesity (Yong et al., 2019) reviews the evidence
for panniculectomy performed concurrently with gynecologic surgeries. The guideline notes that studies in this area have
been primarily small, retrospective, and/or non-comparative studies. The authors indicated that panniculectomy can be
considered at the time of open hysterectomy in patients with obesity, although it is rarely performed; and when a
combined procedure is done, consideration should be given to postoperative antibiotics.
Body Contouring
Body contouring procedures are typically performed for cosmetic purposes. Body contouring procedures can include, but
are not limited to, abdominoplasty, lipectomy, and body lifts. Procedures are often combined for a more global aesthetic
improvement (Shermak, 2020).
In a retrospective case study, Ibrahiem (2022) assessed a comparison of operative risk, hospital length of stay,
complication rate, and patient satisfaction in massive weight loss patients (MWLP) according to the number of surgical
procedures performed in the same surgical setting. The study included 653 MWLP who underwent multiple contouring
procedures simultaneously in a single surgical procedure. All patients underwent surgery between 2016 and 2020. The
patients studied were divided into 4 groups according to the number of anatomical areas operated on. A total of 1254
body contouring procedures were included in the study with a mean of 17 months. The study found that the number of
blood transfusions were statically significantly higher in the IV group (22 patients) than in the other three groups (p value =
0.001). There were no blood transfusions in groups I and II. In comparison to other studies, the average hospital stay was
1.25 days. The overall complication rate (major and minor) was 105 cases (16.07%) in all groups. Patient satisfaction was
highest in patients who underwent 2-3 procedures within the same surgical setting compared to patients who underwent +
3 procedures. The author concluded performing 2 to 3 combined cosmetic procedures in the same surgical setting did not
significantly increase the overall complication rates in the study, but four or more combined procedures were associated
with an increase in the complication rate.
Kalmar et al. (2022) performed a retrospective cohort study to determine whether certain complications are more likely to
occur in patients undergoing functional panniculectomy versus cosmetic abdominoplasty. The study included a total of
11,137 patients who underwent excision of excessive infraumbilical abdominal skin, either a functional panniculectomy (n
= 6397) or cosmetic abdominoplasty (n = 4740). Patients undergoing functional panniculectomy were significantly more
likely to have comorbidities than those undergoing cosmetic abdominoplasty (p < .001). Overall adverse events (p < .001),
medical complications (p = .047), surgical complications (p < .001), related readmission (p < .001), and related
reoperation (p < .001) were significantly higher in patients undergoing functional panniculectomy. Surgical complications
significantly higher in functional panniculectomy included superficial incisional infection (p < .001), deep incisional
infection (p < .001), organ/space infection (p < .001), dehiscence (p = .003), and bleeding requiring transfusion (p = .003).
The researchers concluded functional panniculectomy have increased risk of superficial incisional infection, deep
incisional infection, organ/space infection, dehiscence, bleeding requiring transfusion, and sepsis compared to patients
undergoing cosmetic abdominoplasty. These adverse events are associated with specific preoperative comorbidities in
these patients.
ElAbd et al. (2021) performed a systematic review and meta-analysis to evaluate the effect of body contouring surgery
(BCS) on the magnitude and durability of weight loss after bariatric surgery. Eleven articles were included. The pooled
sample size was 2307, of which 691 were cases who underwent BCS post-bariatric surgery. Nine studies reported results
of BMI changes, six provided excess wight loss (%EWL), and five used total body weight loss (%TBWL). Significant
improvement in weight loss was observed in the BCS group when measured by either body mass index change (∆BMI)
%TBWL, or %EWL. Sub-group analysis showed that increased follow-up time was associated with higher TBWL% (p
0.02). The authors concluded the evidence in this review strongly supports the added long-term benefits of body
contouring surgery for selected patients after massive weight loss following bariatric surgery. Future studies should
attempt to adjust for certain confounding variables, such as the type of bariatric and body contouring surgery performed,
the weight of skin excised during body contouring surgery, and the number of body contouring procedures performed and
their effects on weight loss parameters.
In a systematic review, Jessen et al. (2021) sought to describe surgical techniques used to correct abdominal rectus
diastasis and to investigate recurrence rates and other postoperative complications in relation to the different surgical
techniques. A total of 61 studies met inclusion criteria: 46 used an open approach and 15 used a laparoscopic approach
for repair of the abdominal rectus diastasis. The most common repair was by the classic open low abdominoplasty with a
transverse incision. Laparoscopic techniques were also used. All repairs included a plication of the rectus sheath. In the
open repairs, plication of the anterior rectus sheath was performed as either single- or double-layer and with either
permanent, slowly absorbable, or absorbable suture, with permanent suture being the most common. The authors

Panniculectomy and Body Contouring Procedures
Page 7 of 11
UnitedHealthcare Commercial and Individual Exchange Medical Policy
Effective 07/01/2024
Proprietary Information of UnitedHealthcare. Copyright 2024 United HealthCare Services, Inc.
concluded many different techniques can be used in the correction of abdominal rectus diastasis. In the current literature,
no evidence suggests that one technique is superior to another. Recurrence rate and other complication rates were in
general low. Further research is needed due to limitations which include very limited number of patients, and lack of high-
level evidence with validated assessments of outcomes.
In a systematic review, Van Kerckhoven et al. (2021) evaluated the treatment of diastasis recti. After inclusion criteria was
met 24 articles were reviewed. Patients (n = 931) with rectus diastasis were studied with a follow-up period from 3 weeks
to 20 years. Treatment techniques included rectus sheath plication (n = 761) and midline mesh reinforcement (n = 170).
The most frequently noted comorbidity was obesity and 10.6 percent were smokers. Recurrence was reported in 5
percent of the patients. The most frequent complication was seroma (7%), followed by abdominal hypoesthesia (6%), and
surgical site infection (2%). Chronic pain was reported in 4 percent of the patients. Satisfaction was assessed subjectively
in the majority of patients and was generally rated as high. The authors concluded treatment of diastasis recti is reliable
and long-lasting but could not identify which treatment technique was more reliable.
Jiang et al. (2021) noted many post-bariatric patients have impaired health-related quality of life (HRQoL) due to excess
skin following weight loss; however, it is inconclusive whether body contouring surgery (BCS) improves this impairment. In
a systematic review, the authors summarized existing evidence of the effect of BCS on HRQoL and determine the
prevalence of, the desire for, and barriers to BCS (secondary outcomes). Randomized controlled trials, cohort, cross-
sectional, case-control, and longitudinal studies were systematically searched in PubMed, Embase, the Cochrane Central,
and Web of Science. After screening 1923 potential records, 24 studies (representing 6867 participants) were deemed
eligible. Only 18.5% of respondents from cross-sectional studies underwent BCS, with abdominal BCS as the most
common procedure. Most participants desired BCS but listed "cost" and "lacking reimbursement" as the main barriers.
The authors concluded the results suggest that most post-bariatric patients who underwent BCS experienced
improvements in their HRQoL, which could be seen in almost every dimension evaluated, including body image and
physical and psychosocial functions. The authors recommended both bariatric and plastic surgeons should regard BCS
not only as an aesthetic supplement but also as a vital part of functional recovery in the surgery-mediated weight loss
journey and, thus, provide it to more post-bariatric patients.
Olsson et al. (2021) performed a systematic review to analyze the outcomes of rectus diastasis (RD) repair, focusing on
functional changes following surgery. A comprehensive search in PubMed and Web of Science was performed. Suitable
papers were selected using titles and abstracts with terms suggesting surgical treatment of RD. All abstracts were
scrutinized, and irrelevant studies excluded in four stages. Reports providing original data, including outcome assessment
following surgery, were included. Ten papers with a total of 780 patients were found to fulfil the search criteria. Study
design, surgical procedure, follow-up time, functional outcome and assessment instruments were compiled. All included
studies reported improvements in a variety of functional aspects regardless of surgical method. The outcomes assessed
include core stability, back pain, abdominal pain, posture, urinary incontinence, abdominal muscle strength and quality of
life. The authors concluded that the review showed surgical repair of RD is a safe and effective treatment that improves
functional disability, however, the absence of standardized instruments for assessing outcome makes it impossible to
compare studies. Since indications for surgery are relative and related to core function, the authors recommended valid
instruments for assessing indication and outcome are needed to ensure benefit of the procedure. The study was limited
by the number of studies included in the review and a low level of evidence in some of the included studies.
In a systematic review, Gormley et al. (2020) reviewed the effect of rectus plication on abdominal strength, function, and
postoperative complications. A comprehensive search of CINAHL, Embase, Medline and Web of Science was performed.
Screening and data extraction were performed in duplicate. Data were extracted from the included articles, and outcomes
were analyzed categorically. A total of 497 patients from seven articles were included. Mean age was 44.5 years (range
20.5-72) and 94.4% were female. Three articles reported abdominal strength measurements, with two showing significant
improvement. Four articles used the SF-36 survey, all demonstrating improvement in physical function subscale
postoperatively. An additional six instruments were used to assess functional outcomes, of which four demonstrated
significant improvement. The overall complication rate was 17.0%. The authors noted rectus plication is commonly
performed during abdominoplasty to improve abdominal form and function. They concluded that while the literature to
date is encouraging with respect to functional outcomes, improvements in abdominal strength are less consistent.
Heterogeneity in patient population, outcome measures, and comparison groups limit the strength of the authors’
conclusions. The authors recommend future research should include a large comparative study as well as a protocol for
standardizing outcomes in this population.
Wu et al. (2020) note liposuction is the second most commonly performed cosmetic surgery in the United States. Suction-
assisted lipectomy, more commonly known as liposuction, is an outpatient procedure that removes adipose tissue from
the subcutaneous space with the goal of achieving a more desirable body contour. It is the second most commonly
performed cosmetic surgery in the United States and the most common surgical procedure in patients between the ages
Panniculectomy and Body Contouring Procedures
Page 8 of 11
UnitedHealthcare Commercial and Individual Exchange Medical Policy
Effective 07/01/2024
Proprietary Information of UnitedHealthcare. Copyright 2024 United HealthCare Services, Inc.
of 35 and 64. Liposuction is used to achieve body contouring by removing excess fat deposits in undesirable areas of the
body. Fat is suctioned from demarcated areas in the body amenable to contouring. Liposuction is also increasingly being
used as an adjunct to enhance other aesthetic procedures such as breast augmentation, cervicoplasty, abdominoplasty,
gluteal fat transfer, and body contouring for postsurgical bariatric patients. Non cosmetic indications are expanding,
particularly fat grafting for breast, facial, and pedal reconstruction.
Akram et al. (2014) investigated indications for surgical repair of RD in a systematic review. The authors presented
classifications of RD, current knowledge on the relation to pregnancy, and conservative and surgical management. A
systematic search in PubMed, Embase, Cochrane, and CINAHL revealed 437 studies. Inclusion criteria were applied
according to the above mentioned subjects of interest. In total 28 studies were included, representing 3725 patients, 11 of
these by assessing reference lists of included studies. Only one RCT was found; most studies were case series lacking
statistical analysis. RD was common in post-partum women. Antepartum activity level may have a protective effect on RD
and exercise may improve post-partum symptoms of RD. Repair was done during abdominoplasty or laparoscopically.
The patient-satisfaction was high and long-term recurrence was reported by one study, while five reported no recurrence.
Overall major complications were few, while minor complications were primarily seroma and wound complications. RD is
by itself not a true hernia and, therefore, not associated with the risk of strangulation. The authors conclusions included
repair is mostly done due to cosmetic reasons, the condition does not necessarily require repair, and conservative
management may be an alternative. The authors further note that, if done, the protrusion of the abdomen, rather than the
diastasis itself should influence the decision of repair. The authors recommended that future studies use the established
classifications (e.g. Beer, Rath, or Nahas) when reporting RD and long-term outcome of treatment. Comparison of
surgical techniques and studies that address and compare conservative management with surgery are needed.
Staalesen et al. (2012) performed a systematic review to evaluate the quality of evidence of benefits and risks for patients
having abdominoplasty from massive weight loss or childbirth. Outcome measures were quality-of-life, respiratory
function, back pain, and complication rates. PubMed, Cochrane Database of Systematic Reviews, CRD, CINDAHL,
AMED, PsycINFO and different Health technology Assessment organizations (SBU, Kunnskapssenteret,
Sundhetsstyrelsen) were searched for articles published until October 2011. Inclusion criteria were studies written in
English or Scandinavian language including at least 30 patients with a control group and a case series of at least 100
patients. Review articles and case studies were excluded. The scientific level of evidence was evaluated using the
GRADE-system. One small, controlled study on abdominoplasty was found indicating a positive effect on quality-of-life.
No controlled studies evaluating the other outcomes respiratory function and back pain were found. One prospective
study reported minor complications averaging to 25%. Fourteen retrospective studies reported the same pattern. The
major complication venous thromboembolism was found in 2%-8% in three series. The authors concluded that the quality
of evidence of positive health effects for patients having abdominoplasty is very low concerning all studied outcomes.
Clinical Practice Guidelines
American Society of Plastic Surgeons (ASPS)
ASPS (2016) states abdominoplasties are typically performed for purely cosmetic indications such as unacceptable
appearance due to fat maldistribution or contour deformities caused by pregnancy, stretch marks, contracted scars, and
loose hanging skin after weight loss.
In a practice parameter, ASPS (2017) indicates the timing for body contouring surgery is ideally performed after the
patient maintains a stable weight for 2 to 6 months. For post bariatric surgery patients, this often occurs 12-18 months
after surgery or at the 25 kg/mg
2
to 30 kg/mg
2
weight range. Sometimes procedures are staged. An initial functional
panniculectomy with limited tissue undermining and/or reduction mammaplasty may be necessary to increase the
patient’s comfort and facilitate the ease of exercise and further weight loss. Once the patient approaches his/her ideal
body weight more refined body contouring surgery may be performed to address aesthetic issues.
ASPS (2017) indicates deformities associated with massive weight loss vary greatly depending on the patients’ body type,
their fat deposition pattern, and the amount of weight gained or lost. These deformities can lead to patient dissatisfaction
with appearance, inability to exercise, impaired ambulation, chronic back, neck and shoulder pain, difficulty with hygiene
and symptoms such as uncontrolled intertrigo, infections, and skin necrosis. A panniculectomy or abdominoplasty alone
will eliminate the large hanging abdominal panniculus and its associated symptomatology, but may leave redundant tissue
known as “dog ears” posterior to the excision. Circumferential approaches such as belt lipectomy, and circumferential
lipectomy provide a superior aesthetic result because the anterior deformities as well as back and side rolls are
addressed, and the buttocks lifted. Abdominoplasty and circumferential lipectomy typically would be considered cosmetic
procedures.
Panniculectomy and Body Contouring Procedures
Page 9 of 11
UnitedHealthcare Commercial and Individual Exchange Medical Policy
Effective 07/01/2024
Proprietary Information of UnitedHealthcare. Copyright 2024 United HealthCare Services, Inc.
U.S. Food and Drug Administration (FDA)
This section is to be used for informational purposes only. FDA approval alone is not a basis for coverage.
Panniculectomy and body contouring procedures are procedures and, therefore, not regulated by the FDA. However,
devices and instruments used during the surgery may require FDA approval. Refer to the following website for additional
information: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfPMN/pmn.cfm
. (Accessed February 8, 2024)
References
Acarturk TO, Wachtman G, Heil B, et al. Panniculectomy as an adjuvant to bariatric surgery. Ann Plast Surg. 2004
Oct;53(4):360-6; discussion 367.
Akram J, Matzen SH. Rectus abdominis diastasis. J Plast Surg Hand Surg. 2014 Jun;48(3):163-9.
American Society of Plastic Surgeons. ASPS recommended insurance coverage criteria for third-party payers-
abdominoplasty. Jan 2016. Reaffirmed Sep 2018.
American Society of Plastic Surgeons. ASPS recommended insurance coverage criteria for third-party payers-
panniculectomy. Jul 2006. Reaffirmed Mar 2019.
American Society of Plastic Surgeons. Practice parameter for surgical treatment of skin redundancy for obese and
massive weight loss patients. Jun 2017. Available at:
https://www.plasticsurgery.org/documents/Health-
Policy/Guidelines/guideline-2017-skin-redundancy.pdf. Accessed February 22, 2023.
Diaconu SC, McNichols CHL, AlFadil S, et al. Postoperative outcomes in obese patients that undergo ventral hernia repair
versus ventral hernia repair with concurrent panniculectomy. Plast Reconstr Surg. 2019 Apr;143(4):1211-1219.
ElAbd R, Samargandi OA, AlGhanim K, et al. Body contouring surgery improves weight loss after bariatric surgery: a
systematic review and meta-analysis. Aesthetic Plast Surg. 2021 Jun;45(3):1064-1075.
Elhage SA, Marturano MN, Deerenberg EB, et al. Impact of panniculectomy in complex abdominal wall reconstruction: A
propensity matched analysis in 624 patients. Surg Endosc. 2021 Sep;35(9):5287-5294.
Fennimore R, Fabbri S, Miranda-Seijo P. Panniculectomy at the time of cesarean section and postoperative wound
complications in morbidly obese women. J Reprod Med. 2015 Nov-Dec;60(11-12):535-9.
Gebran SG, Wasicek PJ, Ngaage LM, et al. Panniculectomy at the time of bariatric surgery: a propensity score-matched
analysis of outcomes in the MBSAQIP database. Surg Obes Relat Dis. 2021 Jan 1;17(1):177-184.
Gormley J, Copeland A, Augustine H, et al. Impact of rectus diastasis repair on abdominal strength and function: A
systematic review. Cureus. 2020 Dec 29;12(12):e12358.
Ibrahiem SMS. Investigating the safety of multiple body contouring procedures in massive weight loss patients. Aesthetic
Plast Surg. 2022 Dec;46(6):2891-2902.
Jessen ML, Öberg S, Rosenberg J. Surgical techniques for repair of abdominal rectus diastasis: a scoping review. J Plast
Surg Hand Surg. 2021 Aug;55(4):195-201.
Jiang Z, Zhang G, Huang J, et al. A systematic review of body contouring surgery in post-bariatric patients to determine its
prevalence, effects on quality of life, desire, and barriers. Obes Rev. 2021 May;22(5):e13201.
Kalmar CL, Park BC, Kassis S, et al. Functional panniculectomy vs cosmetic abdominoplasty: Multicenter analysis of risk
factors and complications. J Plast Reconstr Aesthet Surg. 2022 Sep;75(9):3541-3550.
McNichols CHL, Diaconu S, Liang Y, et al. Outcomes of ventral hernia repair with concomitant panniculectomy. Ann Plast
Surg. 2018 Apr;80(4):391-394.
Medicare Coverage Database. Local Coverage Determination. Sacroiliac Joint Injections and Procedures L39462. 2024.
LCD - Sacroiliac Joint Injections and Procedures (L39462) (cms.gov)
. Accessed February 23, 2024.
Nag S, Patel T, Gaughan JP, et al. Panniculectomy performed in conjunction with gynecologic surgery in obese and
morbidly obese patients: A national surgical quality improvement program analysis and systematic review of the literature.
Ann Plast Surg. 2021 Nov 1;87(5):600-605.
Olsson A, Kiwanuka O, Sandblom G, et al. Evaluation of functional outcomes following rectus diastasis repair-an up-to-
date literature review. Hernia. 2021 Aug;25(4):905-914.

Panniculectomy and Body Contouring Procedures
Page 10 of 11
UnitedHealthcare Commercial and Individual Exchange Medical Policy
Effective 07/01/2024
Proprietary Information of UnitedHealthcare. Copyright 2024 United HealthCare Services, Inc.
Prodromidou A, Iavazzo C, Psomiadou V, et al. Safety and efficacy of synchronous panniculectomy and endometrial
cancer surgery in obese patients: A systematic review of the literature and meta-analysis of postoperative complications. J
Turk Ger Gynecol Assoc. 2020 Dec 4;21(4):279-286.
Sachs D, Sequeira Campos M, Murray J. Panniculectomy. 2021 Oct 9. In: StatPearls [Internet]. Treasure Island (FL):
StatPearls Publishing; 2022 Jan.
Shermak MA. Abdominoplasty with combined surgery. Clin Plast Surg. 2020 Jul;47(3):365-377.
Sosin M, Termanini KM, Black CK, et al. Simultaneous ventral hernia repair and panniculectomy: A systematic review and
meta-analysis of outcomes. Plast Reconstr Surg. 2020 Apr;145(4):1059-1067.
Staalesen T, Elander A, Strandell A, et al. A systematic review of outcomes of abdominoplasty. J Plast Surg Hand Surg.
2012 Sep;46(3-4):139-44.
Van Kerckhoven L, Nevens T, Van De Winkel N, et al. Treatment of rectus diastasis: should the midline always be
reinforced with mesh? A systematic review. J Plast Reconstr Aesthet Surg. 2021 Aug;74(8):1870-1880.
Wu S, Coombs DM, Gurunian R. Liposuction: Concepts, safety, and techniques in body-contouring surgery. Cleve Clin J
Med. 2020 Jun;87(6):367-375.
Yong PJ, Thurston J, Singh SS, et al. Guideline No. 386-Gynaecologic surgery for patient with obesity. J Obstet Gynaecol
Can. 2019 Sept 1; 41(9):1356-1370.
Policy History/Revision Information
Date
Summary of Changes
09/01/2024
Related Policies
• Updated reference link to the Medicare Advantage Medical Policy titled Cosmetic and
Reconstructive Procedures
07/01/2024
Coverage Rationale
Panniculectomy
• Replaced language indicating “Panniculectomy is not considered medically necessary when
performed for the [listed] indications” with “Panniculectomy is considered cosmetic and not
medically necessary when performed for the [listed] indications”
• Revised list of cosmetic and not medically necessary indications; replaced “when performed for
primarily cosmetic purposes, including but not limited to, post childbirth in order to return to pre-
pregnancy shape” with “when performed for primarily cosmetic purposes”
Documentation Requirements
• Updated list of required clinical information; replaced criterion for panniculectomy requiring
“photographs of a full-frontal view of the hanging pannus, a full-frontal view of pannus elevated
that allows any skin damage can be evaluated, and a full lateral view of the hanging pannus”
with “photographs of a full-frontal view of the hanging pannus, a full-frontal view of pannus
elevated that allows for the evaluation of any skin damage, and a full lateral view of the hanging
pannus”
Supporting Information
• Updated Clinical Evidence and References sections to reflect the most current information
• Archived previous policy version MP.014.22
Instructions for Use
This Medical Policy provides assistance in interpreting UnitedHealthcare standard benefit plans. When deciding coverage,
the member specific benefit plan document must be referenced as the terms of the member specific benefit plan may
differ from the standard plan. In the event of a conflict, the member specific benefit plan document governs. Before using
this policy, please check the member specific benefit plan document and any applicable federal or state mandates.
UnitedHealthcare reserves the right to modify its Policies and Guidelines as necessary. This Medical Policy is provided for
informational purposes. It does not constitute medical advice.
This Medical Policy may also be applied to Medicare Advantage plans in certain instances. In the absence of a Medicare
National Coverage Determination (NCD), Local Coverage Determination (LCD), or other Medicare coverage guidance,
CMS allows a Medicare Advantage Organization (MAO) to create its own coverage determinations, using objective
evidence-based rationale relying on authoritative evidence (Medicare IOM Pub. No. 100-16, Ch. 4, §90.5
).
Panniculectomy and Body Contouring Procedures
Page 11 of 11
UnitedHealthcare Commercial and Individual Exchange Medical Policy
Effective 07/01/2024
Proprietary Information of UnitedHealthcare. Copyright 2024 United HealthCare Services, Inc.
UnitedHealthcare may also use tools developed by third parties, such as the InterQual
®
criteria, to assist us in
administering health benefits. UnitedHealthcare Medical Policies are intended to be used in connection with the
independent professional medical judgment of a qualified health care provider and do not constitute the practice of
medicine or medical advice.
