
(
PB98-916401
NTSB/MAR-98/01
NATIONAL
TRANSPORTATION
SAFETY
BOARD
WASHINGTON,
D.C.
20594
MARINE ACCIDENT REPORT
ALLISION OF THE LIBERIAN FREIGHTER
BRIGHT
FIELD WITH THE POYDRAS STREET
WHARF, RIVERWALK MARKETPLACE, AND
NEW ORLEANS HILTON HOTEL IN
NEW ORLEANS, LOUISIANA
DECEMBER 14, 1996
E!!!k!d
P
.,
‘e.
:--9
-Q
.
‘
‘..
—.
-.
–—
—’””
6885A
\
U S
GOWRNMEhl
PRINT!%
OFFICE
IW
0+4!4s
Abstract: On December 14, 1996, the fully loaded Liberian bulk carrier Bright Field
temporarily lost propulsion power as the vessel was navigating outbound in the Lower
Mississippi River at New Orleans, Louisiana. The vessel struck a wharf adjacent to a populated
commercial area that included a shopping mall, a condominium parking garage, and a hotel. No
fatalities resulted from the accident, and no one aboard the Bright Field was injured; however, 4
serious injuries and 58 minor injuries were sustained during evacuations of shore facilities, a
gaming vessel, and an excursion vessel located near the impact area. Total property damages to
the Bright Field and to shoreside facilities were estimated at about $20 million.
The safety issues discussed in this report are the adequacy of the ship’s main engine and
automation systems, the adequacy of emergency preparedness and evacuation plans of vessels
moored in the Poydras Street wharf area, and the adequacy of port risk assessment for activities
within the Port of New Orleans. This report also addresses three other issues: the actions of the
pilot and crew during the emergency, the lack of effective communication (as it relates to the
actions of the pilot and crew aboard the Bright Field on the day of the accident), and the delay in
administering toxicological tests to the vessel crew.
As a result of its investigation, the National Transportation Safety Board issued
recommendations to the U.S. Coast Guard, the U.S. Army Corps of Engineers, the State of
Louisiana, the Board of Commissioners of the Port of New Orleans, International RiverCenter,
Clearsky Shipping Company, New Orleans Paddlewheels, Inc., the New Orleans Baton Rouge
Steamship Pilots Association, the Crescent River Port Pilots Association, and Associated Federal
Pilots and Docking Masters of Louisiana, Inc.
The National Transportation Safety Board is an independent Federal agency dedicated to
promoting aviation, railroad, highway, marine, pipeline, and hazardous materials safety. Established
in 1967, the agency is mandated by Congress through the Independent Safety Board Act of 1974 to
investigate transportation accidents, determine the probable causes of the accidents, issue safety
recommendations, study transportation safety issues, and evaluate the safety effectiveness of
government agencies involved in transportation. The Safety Board makes public its actions and
decisions through accident reports, safety studies, special investigation reports, safety
recommendations, and statistical reviews.
Information about available publications may be obtained by contacting:
National Transportation Safety Board
Public Inquiries Section, RE-51
490 L’Enfant Plaza, S.W.
Washington, D.C. 20594
(202) 314-6551
Safety Board publications may be purchased, by individual copy or by subscription, from:
National Technical Information Service
5285 Port Royal Road
Springfield, Virginia 22161
(703) 605-6000
#..+5+10"1("6*'".+$'4+#0"(4'+)*6'4
$4+)*6"(+'.&"9+6*"6*'"21;&4#5"564''6
9*#4(."4+8'49#.-"/#4-'62.#%'."#0&
0'9"14.'#05"*+.610 "*16'."+0
0'9"14.'#05.".17+5+#0#
&'%'/$'4"36."3;;8
MARINE ACCIDENT REPORT
Adopted: January 13, 1998
Notation 6885A
0#6+10#.
64#052146#6+10
5#('6;"$1#4&
9CUJKPIVQP."&0%0"427;6

this page intentionally left blank
iii
CONTENTS
EXECUTIVE SUMMARY.........................................................................................................vii
INVESTIGATION
Synopsis .......................................................................................................................................... 1
Preaccident Events ..........................................................................................................................1
The Accident ................................................................................................................................... 5
Injuries...........................................................................................................................................10
Vessel Damage..............................................................................................................................10
Other Damage................................................................................................................................ 10
Crew Information .......................................................................................................................... 14
The Pilot................................................................................................................................. 14
The Master ............................................................................................................................. 14
The Chief Engineer................................................................................................................16
The Previous Chief Engineer................................................................................................. 17
Vessel Information ........................................................................................................................ 17
Bright Field............................................................................................................................ 17
Automated Propulsion Control System ..........................................................................18
Engine Lubricating Oil System.......................................................................................19
Cruise Ships ........................................................................................................................... 20
Gaming and Excursion Vessels.............................................................................................. 20
Waterway Information................................................................................................................... 21
River Stage............................................................................................................................. 21
Vessel Traffic Control............................................................................................................ 21
Port Information............................................................................................................................ 22
Dredging................................................................................................................................. 22
The Wharf Area...................................................................................................................... 23
Federal Jurisdiction................................................................................................................23
Meteorological Information ..........................................................................................................25
Toxicological Information.............................................................................................................25
Survival Aspects............................................................................................................................ 26
Bright Field............................................................................................................................ 26
Enchanted Isle........................................................................................................................26
Nieuw Amsterdam.................................................................................................................. 26
Queen of New Orleans...........................................................................................................27
Creole Queen ......................................................................................................................... 30
Riverwalk Marketplace..........................................................................................................32
Hilton Riverside Hotel ...........................................................................................................33
Emergency Response.....................................................................................................................34
Port of New Orleans Harbor Police ....................................................................................... 34
Coast Guard Group New Orleans ..........................................................................................35
Louisiana Office of Emergency Preparedness .......................................................................35
iv
Police Departments ................................................................................................................35
New Orleans Fire Department ...............................................................................................35
New Orleans Department of Health and Emergency Medical Services................................. 35
Emergency Preparedness...............................................................................................................36
Riverwalk Marketplace..........................................................................................................36
New Orleans Hilton Riverside Hotel ..................................................................................... 36
Queen of New Orleans...........................................................................................................36
Safety Briefings............................................................................................................... 37
Signage............................................................................................................................ 37
Emergency Egress........................................................................................................... 37
Drills ............................................................................................................................... 38
Creole Queen ......................................................................................................................... 38
Inspections, Tests, and Research...................................................................................................38
Steering Gear.......................................................................................................................... 39
Main Engine—General .......................................................................................................... 39
Main Engine Lubricating Oil Sump.......................................................................................39
Main Engine Lubricating Oil Pumps/Motors......................................................................... 39
Main Engine Lubricating Oil System Second Filter/Strainer ................................................40
Main Engine Lubricating Oil Purifier.................................................................................... 40
Automatic Main Engine Lubricating Oil Trip Function ........................................................41
Alarms, Indicators, and Recorders.........................................................................................41
Remote Engine Control Tests ................................................................................................41
Preventive Maintenance.........................................................................................................41
Reports and Recordkeeping ................................................................................................... 41
Main Engine Lubricating Oil Testing and Analysis............................................................... 42
Spare Parts and Calibration Tools.......................................................................................... 42
Sulzer Inspection....................................................................................................................42
Chief Engineer’s Assessment................................................................................................. 43
Tests, Reports, and System Calibration ................................................................................. 43
Computer Simulation.............................................................................................................44
Other Information..........................................................................................................................44
Port Risk Analysis and Management—Coast Guard............................................................. 44
Port Risk Analysis and Management—Other Stakeholders .................................................. 45
Lower Mississippi River Safety Study............................................................................ 45
Louisiana World Exposition........................................................................................... 45
International RiverCenter................................................................................................ 46
New Orleans Aquarium of the Americas........................................................................ 46
Gaming Vessel Risks and Background........................................................................... 47
Operation Safe River....................................................................................................... 50
Changes Made Since the Accident......................................................................................... 51
River Front Alert Network.............................................................................................. 51
New Notices, Rules, and Operating Regulations............................................................ 51
Steering Loss Study ........................................................................................................ 53
Ship Drill Alarms............................................................................................................ 53
Riverwalk Marketplace Alert System............................................................................. 53
v
Vessel Egress..................................................................................................................54
Status of the Queen of New Orleans...............................................................................54
General .......................................................................................................................................... 55
ANALYSIS
Accident Overview........................................................................................................................55
Engineering Aspects......................................................................................................................56
Main Engine Shutdown and Restart....................................................................................... 56
Lubricating Oil Pump Operation............................................................................................ 57
General Condition of the Bright Field’s Engineering Plant................................................... 57
Vessel Owner’s Oversight of the Bright Field’s Engineering Plant...................................... 58
Communication............................................................................................................................. 59
Master-Pilot Briefing at the Anchorage .................................................................................59
Language Differences............................................................................................................. 60
Information Exchange During the Emergency....................................................................... 60
Emergency Response.....................................................................................................................62
Vessel Emergency Preparedness and Evacuation Plans................................................................ 63
Vessel Evacuation..................................................................................................................63
Emergency Drills....................................................................................................................65
Safety Briefings and Signage.................................................................................................66
Shoreside Emergency Alert and Response............................................................................. 67
Toxicological Testing.................................................................................................................... 68
Risk Assessment and Risk Management....................................................................................... 69
Findings......................................................................................................................................... 75
CONCLUSIONS
Findings......................................................................................................................................... 74
Probable Cause.............................................................................................................................. 76
RECOMMENDATIONS............................................................................................................ 77
APPENDIXES
APPENDIX A--Investigation........................................................................................................81
APPENDIX B--Chronology of Bright Field Engineering Problems ............................................ 83
APPENDIX C--Voyage Data Recorders (VDRs) .........................................................................89

this page intentionally left blank

vii
Shortly after 1400 on December 14, 1996,
the fully loaded Liberian bulk carrier
Bright
Field
temporarily lost propulsion power as the
vessel was navigating outbound in the Lower
Mississippi River at New Orleans, Louisiana.
The vessel struck a wharf adjacent to a
populated commercial area that included a
shopping mall, a condominium parking garage,
and a hotel. No fatalities resulted from the
accident, and no one aboard the
Bright Field
was injured; however, 4 serious injuries and 58
minor injuries were sustained during
evacuations of shore facilities, a gaming vessel,
and an excursion vessel located near the impact
area. Total property damages to the
Bright Field
and to shoreside facilities were estimated at
about $20 million.
The National Transportation Safety Board
determines that the probable cause of this
accident was the failure of Clearsky Shipping
Company to adequately manage and oversee the
maintenance of the engineering plant aboard the
Bright Field
, with the result that the vessel
temporarily lost power while navigating a high-
risk area of the Mississippi River. Contributing
to the amount of property damage and the
number and types of injuries sustained during
the accident was the failure of the U.S. Coast
Guard, the Board of Commissioners of the Port
of New Orleans, and International RiverCenter
to adequately assess, manage, or mitigate the
risks associated with locating unprotected
commercial enterprises in areas vulnerable to
vessel strikes.
The major safety issues identified in this
investigation are the adequacy of the ship’s
main engine and automation systems, the
adequacy of emergency preparedness and
evacuation plans of vessels moored in the
Poydras Street wharf area, and the adequacy of
port risk assessment for activities within the
Port of New Orleans. This report also addresses
three other issues: the actions of the pilot and
crew during the emergency, the lack of effective
communication (as it relates to the actions of the
pilot and crew aboard the
Bright Field
on the
day of the accident), and the delay in
administering toxicological tests to the vessel
crew.
As a result of its investigation of this
accident, the Safety Board issued safety
recommendations to the U.S. Coast Guard, the
U.S. Army Corps of Engineers, the State of
Louisiana, the Board of Commissioners of the
Port of New Orleans, International RiverCenter,
Clearsky Shipping Company, New Orleans
Paddlewheels, Inc., the New Orleans Baton
Rouge Steamship Pilots Association, the
Crescent River Port Pilots Association, and
Associated Federal Pilots and Docking Masters
of Louisiana, Inc.
EXECUTIVE SUMMARY

this page intentionally left blank

1
Synopsis
Shortly after 1400 on December 14, 1996,
the fully loaded Liberian bulk carrier
Bright
Field
temporarily lost propulsion power as the
vessel was navigating outbound in the Lower
Mississippi River at New Orleans, Louisiana.
The vessel struck a wharf adjacent to a
populated commercial area that included a
shopping mall, a condominium parking garage,
and a hotel. No fatalities resulted from the
accident, and no one aboard the
Bright Field
was injured; however, 4 serious injuries and 58
minor injuries were sustained during
evacuations of shore facilities, a gaming vessel,
and an excursion vessel located near the impact
area. Total property damages to the
Bright Field
and to shoreside facilities were estimated at
about $20 million.
Preaccident Events
According to vessel records, on September 2,
1996, the 735-foot, 36,120 gross-ton
Bright Field
completed loading a cargo of coal in
Banjarmasin, Indonesia. On September 12, 1996,
the vessel departed Indonesia with a 28-member
Chinese crew bound for Davant, Louisiana. The
estimated date of arrival at Southwest Pass,
Louisiana,
1
(the vessel’s entrance point to the
Mississippi River) was October 26, 1996. Shortly
after departure, the ship began to experience
problems with its engineering plant, necessitating
a 3-day layover in Singapore while repairs were
made to the main engine. After the repairs were
completed, the
Bright Field
continued its voyage.
The trip was interrupted on several occasions by
continuing main engine problems.
On November 21, 1996, the
Bright Field
arrived at a bulk coal-handling facility near
Davant, Louisiana (mile 55 AHP
2
), where it
1
Southwest Pass is the westernmost of the several
entrances to the Mississippi River and is the one most often
used.
2
Distances in the Mississippi River are measured in
statute miles “above head of passes” (AHP), which is
located 20 miles above Southwest Pass.
unloaded its cargo. (See figure 1.) After its holds
were prepared to load grain and after waiting for
a loading berth, the
Bright Field
arrived at
Cargill Terminal, located at mile 140 AHP in
Reserve, Louisiana, on December 9, 1996.
There the vessel loaded 56,397 metric tons of
corn in its seven cargo holds. The vessel left the
terminal at 1530 on December 11, 1996.
3
The
vessel moved from the terminal area to the
lower portion of La Place Anchorage at mile
135 AHP, where it remained at anchor for 2
days while scheduled repairs were made to the
main engine’s turbocharger and air cooler.
On December 14, 1996, the vessel’s agent
contacted the New Orleans Baton Rouge
Steamship Pilots Association (NOBRA) and
requested that a pilot be dispatched to the vessel.
4
The sailing time was set for 1030. The pilot who
was dispatched to the
Bright Field
stated that he
was called for duty about 0730. He said he was
told that the ship was headed to sea, which
meant that he would take the ship to a specified
location, where he would be replaced by a pilot
from the Crescent River Port Pilots Association
for the remainder of the trip downriver. The
pilot said he expected to be aboard the
Bright
Field
for about 3 hours.
The
Bright Field
third mate and chief
electrician stated that on the morning of
December 14 they completed all predeparture
tests for both bridge and engineering, including
testing the bridge main engine console lights and
alarms. With the successful completion of the
tests, the master ordered standby engines at 0943.
The pilot boarded the vessel via launch at 1040,
3
At the time of departure, the draft of the vessel was
11.96 meters (about 39 feet 4 inches) forward and 12.06
meters (about 39 feet 8 inches) aft.
4
Louisiana State law requires that a qualified and
certified State pilot be on board any vessel in foreign trade
navigating the Mississippi River in the State. Although
NOBRA, as well as other pilot associations, dispatches
pilots, bills and collects pilotage fees, and pays association
expenses, including staff and transportation fees, the pilots
themselves are self-employed and contract for their services
directly with vessel operators.
INVESTIGATION

2
N
0LOH
473
0LOH
453
0LOH
433
0LOH
<8
0LOH
83
7
R#
*
XO
I#
RI
0H[LFR#
D
Q
G
+
H
DG#R
I
#3D
VV
H
V
/$.(#3217&+$575$,1
1(:
25/($16
#
$
%
&
'
:
#
$
%
&
'
:
0#5HVHUYH
0#1RUFR
0#'HVWUHKDQ
0#1LQH#0LOH#3RLQW
0#'DYDQW
0#$FFLGHQW#6LWH
/RFDWLRQ#/HJHQG
Figure 1 -- Lower Mississippi River

3
and the third mate escorted him to the
wheelhouse, where he was introduced to the
master at 1044.
The ship’s master spoke what the pilot
described as broken, but adequate, English. The
pilot said that, to facilitate communication, he
spoke slowly and used simple words, and he
believed that he and the master understood each
other. The master also stated that he was
satisfied with their ability to communicate. The
pilot said he gave helm orders in English to the
helmsman, who repeated them in English before
carrying them out. The second mate reported
that he also repeated (in English) the pilot’s
orders and then carried them out. Other than
orders and their repetition, the pilot said he had
no verbal exchanges with the second mate or the
helmsman.
The pilot, who had not previously handled
the
Bright Field
, said he asked if the ship’s
navigational equipment and engine were in good
working order. He stated that the master
answered with “just a simple ‘yes’ to both
questions.” The master stated that he asked the
pilot about the operational procedures for
departing the anchorage.
5
These were the only
items reported as being discussed during the
predeparture briefing. The pilot said he then
proceeded to acquaint himself with the
wheelhouse layout (figure 2) and with the
vessel’s posted maneuvering information. At the
time, the vessel’s main engine was being
operated from the wheelhouse.
At 1055,
6
the pilot began the normal
procedures for getting underway by ordering the
first engineering maneuvering bell (dead slow
ahead). According to the third mate, he (the
third mate) attempted to execute the pilot’s
order using the wheelhouse engine controls, but
the vessel’s main engine did not start. He then
called the engine control room and told the chief
engineer—in Chinese—that the engine did not
start. Engine control was transferred to the
engine control room. Both the master and the
chief engineer stated that their normal practice
5
This information typically includes, among other
details, the location of assist tugboats and the order in
which the two anchors are to be raised.
6
Times are taken from engine bell logs.
was to transfer engine control to the engine
control room in the event of a nonemergency
problem with the propulsion system.
After the engines were started (1055.5, dead
slow ahead), engine control was transferred
back to the wheelhouse. The pilot ordered stop
engine, and the engine was stopped. At 1110,
the pilot ordered dead slow ahead. Again, the
engine could not be started from the
wheelhouse, and again control was transferred
to the engine control room, from which the
engine was restarted. After the accident, the
pilot stated that he had not been advised of the
difficulties in starting the engine from the
wheelhouse, nor was he informed on those
occasions when engine control was transferred
to or from the engine control room.
The
Bright Field
departed the La Place
anchorage at 1112. Engine maneuvering control
was transferred back to the wheelhouse, and the
pilot ordered full ahead maneuvering speed (56
rpm) in order to familiarize himself with the
ship’s responsiveness to rudder and engine
orders. He said he determined that the
Bright
Field
handled as expected for a fully loaded
bulk cargo vessel operating in high-river-stage
conditions.
7
At 1134, the pilot ordered sea speed
(72 rpm) for better ship handling. The pilot said
it was necessary to operate the ship at maximum
speed in order to obtain the best maneuverability
in that operating environment.
Engine rpm was increased to sea speed
using wheelhouse controls. At 1159, as the
vessel approached Norco, Louisiana, the pilot
ordered the
Bright Field’
s
speed reduced to full
ahead maneuvering speed (56 rpm). The
Bright
Field
remained at full ahead maneuvering speed
until it reached the vicinity of Destrehan,
Louisiana, when the pilot again ordered sea
speed of 72 rpm, resulting in a ground speed
(speed of the ship plus speed of the current) of
about 16 knots.
About 1300, the pilot ordered the master to
send a seaman to stand by the anchors.
8
The
7
On the day of the accident, the river was at high river
stage, measuring 12.5 feet on the Carrollton gauge with an
approximate 4 1/2-mph current.
8
A Board of Commissioners of the Port of New
Orleans ordinance required that all vessels navigating

4
master sent the ship’s carpenter, with a handheld
radio, to serve as anchor watch.
9
A few miles
above Nine Mile Point, the pilot established
VHF communications
10
with an inbound tow
and inbound ship, both below Nine Mile Point.
The vessels agreed to a starboard-to-starboard
meeting, and all three vessels met at the point.
The pilot of the
Bright Field
said that, because
the inbound tow was farther off the bank than
anticipated, he maneuvered his ship
closer to the
left descending bank of the river. The
Bright
through the New Orleans Port area maintain an anchor
standby of at least one competent seaman, who was to be
stationed at the anchor windless and be prepared to drop
anchor if necessary.
9
Serving as anchor watch was a regularly assigned
duty of the
Bright Field
’s carpenter.
10
VHF channel 67 was assigned for routine bridge-to-
bridge (navigation/safety) communication in the Lower
Mississippi River.
Field
pilot sounded the danger signal
11
to alert
the workers at the Southport barge fleeting
facility
12
to the proximity of the
Bright Field
.
The
Bright Field
passed the area without
incident and continued down the river at sea
speed. The master told Safety Board
investigators that about this time he became
concerned that the pilot might be oversteering
the vessel, but he said he did not voice his
concerns to the pilot.
About 1350, the pilot made the first radio
call to the U.S. Coast Guard Gretna light
operator.
13
The Gretna light operator advised the
11
Five or more shorts blasts on the ship’s whistle.
12
A
fleet
in this instance refers to one or more tiers of
barges. A fleeting facility is the geographic area along or
near a river bank where a barge mooring service is located.
13
According to 33
Code of Federal Regulations
(CFR)
161.402(b), “Movements of vessels in vicinity of Algiers
Point, New Orleans Harbor,” during a high river stage,
1$9,*$7,21
(48,30(17
&+$57
7$%/(
5$'$5
2$53$
72#/2:(5
'(&.6
+(/060$1
+$/$50#/,*+762
7(/(3+21(6,
5$'$5
+(/0
*<52
3,/27
:,1'2:6#+8,
:+,67/(
&21752/
%87721
0$67(5
3257
%5,'* (
:,1*
:,1'2:6
6(&21'
0$7(
0$18(9(5,1*
/(9(52(1*,1(
25'(5
7(/(*5$3+
:2+#(1*,1(
&21752/#&2162/(
67$5%2$5'
%5,'* (
:,1*
$)7
):
'
Figure 2 -- navigation bridge layout
Bri
g
ht Field

5
Bright Field
that the ship was cleared to transit
Algiers Point and that a seagoing tow boat was
inbound at the Point. The pilot stated that, while
the
Bright Field
was transiting under the
Crescent City Connection Bridges, he allowed
the vessel to acquire a current-induced swing to
port to facilitate the upcoming maneuver around
Algiers Point.
The Accident
The swing to port as the ship passed under
the Crescent City Connection Bridges pointed
the vessel toward the left descending bank, the
side of the river where the Poydras Street wharf
and the Riverwalk Marketplace shopping mall
were located and where gaming, excursion, and
cruise ships were docked. About 1406, while the
Bright Field
was still transiting under the
bridges, power output from the vessel’s main
engine dropped. At this time, the vessel’s
automated propulsion control system
14
reported
low main engine lubricating oil pressure and
main engine trip due to low oil pressure.
15
The pilot said he noticed that the vessel had
gotten quiet and that the engine-induced vessel
vibrations had stopped. He said he turned and
saw the master and the second mate
16
standing
beside the engine order telegraph (on the other
side of the bridge from the pilot), looking down
at something on the console. He said he asked
them if there was a problem, but got no
response. He said that he did not ask a second
time “because they didn’t answer me the first
time.” He reported that he then looked at the
engine rpm indicator and saw that engine rpm
movement of vessels around Algiers Point is controlled by
several Coast Guard-operated and maintained traffic lights,
including Gretna light at 96.6 miles AHP and Governor
Nicholls light at 94.3 AHP.
14
For the purposes of this report,
automated
propulsion control system
and related terms will be used to
refer to all main engine control, monitoring, and alarm
systems and subsystems.
15
The main engine was equipped with protection
devices that could slow down or stop the main engine
depending on the severity of the problem. See the “Main
Engine Description” section of this report for information
about the engine and its protective devices.
16
The second mate had come on duty at the noon
watch to replace the third mate who had been on duty when
the ship left the anchorage.
had dropped from about 70 to about 30,
indicating to him that the vessel had experienced
a significant reduction in engine power.
The master and the second mate said that
they also noticed that the ship’s normal operating
vibrations had stopped, and they observed that the
main engine rpm indicator showed a drop to
about 30 rpm. The master said the pilot “blurted
out, ‘What has happened?’” and he (the master)
thought he had answered the pilot by saying
there had been a reduction in main engine
power. The master said it was not clear to him
why engine rpm had dropped. He said he
instructed the second mate “to call the
engineroom to inquire about what happened,
what’s going on. I asked the second mate to
demand them to increase speed right away.” The
second mate said that he carried out the master’s
order immediately.
The pilot stated that when he realized that the
vessel had lost power, he “jumped” out of his
chair and called the Governor Nicholls Light
operator on VHF channel 67. He said that as he
made the call he was looking out the bridge
windows and was aware that the vessel was
swinging to port and toward the docked ships
along the left descending bank. The pilot told the
Governor Nicholls light operator that his ship had
lost power and that the operator should alert
everyone in the harbor.
17
The pilot said that, after calling the light
operator, he ordered hard starboard rudder as the
ship continued to swing to port. The helmsman
responded to the order by applying hard
starboard rudder, but the new rudder setting did
nothing to alter the vessel’s direction, and the
pilot began sounding the danger signal using the
ship’s forward whistle. He said he wanted to
attract the attention of the cruise ships and
public along the left descending river bank. The
pilot stated that he ordered the master on at least
two occasions to have someone stand by the
17
Information regarding radio transmissions using
VHF channel 67 is based on audio recordings made by the
tugboat
Lockmaster
, located on the side of the river
opposite the Poydras Street wharf. The
Lockmaster
was
also able to provide a videotape of radar images of the
Bright Field
as it approached and struck the wharf. The
traffic light stations were not equipped to record radio
transmissions.

6
anchors, but he did not hear the master
acknowledge the order. The pilot said he recalled
the master speaking Chinese on the radio and
that the master did not appear to be agitated, but
was “very nonchalant.”
When the pilot noted that the rpm indicator
continued to show a loss of power, he made
another call to the Governor Nicholls light
operator. He told the operator to warn the cruise
ships and gaming and excursion vessels that
were moored along the left descending bank.
The Gretna light operator advised the pilot that a
tugboat 1 mile upriver was coming to his aid.
The chief engineer on duty in the engine
control room
18
(figure 3) stated that,
immediately before the engine lost power, an
audible alarm sounded. He said he then looked
at a computer screen in front of him and saw a
visual alarm and an indication of a loss of
pressure in the lubricating oil system. (See
figure 4.) He said he looked at the analog main
engine lubricating oil pressure gauge and saw
that the system was rapidly “depressurizing”
below normal levels. He said he then noticed
that the main engine automatic slow down light
was on, and he noticed that main engine noise
was decreasing. He reported that he also
observed that engine rpm had dropped from 72
to between 30 and 35. He said that, as he turned
to the electrical switchboard behind him to
determine why the No. 2 lubricating oil pump
had not started automatically, the pump started.
He said that, except for the low rpm, everything
seemed to him to be back to normal almost
immediately.
According to the chief engineer, he was
about to call the bridge when the second mate
called him. He said that the second mate asked
him why the main engine was slowing down and
told him to increase the speed immediately, that
they were transiting the bridge at that time. The
chief engineer reported that the second mate
spoke to him in a normal tone of voice, without
18
At the time of the accident, Coast Guard regulations
did not require that engineering spaces be manned during
transit of the Mississippi River. Although the
Bright Field
was classed for unattended operation of machinery spaces,
company regulations required that the chief engineer and
two other engineers be on duty in the engine control room
whenever the vessel was entering or leaving a port.
repeating his message. The chief engineer said
he thought the second mate was concerned
about speeding up passage of the vessel beneath
the bridges. He said he did not know the nature
of the situation on the vessel’s bridge.
The chief engineer told the second mate that
he did not know the reason for the sudden drop
in the No. 1 oil pump pressure, but since the No.
2 pump had already come on line, the
pressurization problem was solved. Neither the
master nor the second mate attempted to clear
the trip condition and restart the engine, and
thus restore rpm, from the bridge controls. The
chief engineer and the second mate mutually
agreed to transfer engine control to the engine
control room, and the chief engineer began the
process of restoring engine power. He said that
engine rpm quickly reached about 52 rpm, after
which rpm continued to increase to about 60.
According to alarm logs, main engine power
was restored to the vessel at 1408, about 2
minutes after the logs indicated that the main
engine had tripped.
In postaccident testimony, the master was
asked if it had been necessary to transfer engine
control from the bridge to the engine control
room during the emergency. He said, “Under
normal circumstances, speed increase can be
done from the engine [control room] more
quickly.” The master was asked why the engine
control room had requested that engine control
be shifted from the bridge to the engineroom.
He said that it was “because the engineering
department [didn’t] realize the sense of urgency
or [that] there [was] any sense of urgency on the
bridge.” He said engine control room personnel
were not initially notified of the emergency
situation but were told later when the allision
19
was unavoidable even if vessel speed were
increased.
The pilot stated that at this time he was
devoting his attention to sounding the danger
signal to alert the moored ships along the left
descending bank and the Riverwalk complex
and that he was not immediately aware, nor was
19
In marine usage,
allision
refers to a moving ship
striking a stationary ship or other stationary object.

7
Figure 3 -- engine control room layout showing
reported positions of crewmembers when engine power
reduction occurred.
Bright Field
0DL Q#(QJLQH
*DXJHV
7HUDVDNL#0RQLWRUV
0DLQ#(QJLQH
&RQWUROV
(QJLQH HU·V
:RUNVSDFH
'HVN
6HFRQG#(QJLQHHU
&KLHI#(QJLQHH U
7KLUG#(QJLQHHU
(OHFWULFDO#6ZLWFKERDUGV#)#0RWRU#&R QWUR OOHUV
)25: $5'
(QJLQHHULQJ#FRQWURO/#PRQLWRU/#DQG#DODUP#FRQVROH
0DLQ
(QJLQH
5HPRWH
&RQWURO
&LUFXLWV
$2&
Figure 4 -- Engineering control, monitor, and alarm console

8
he made aware by the mate or the master, that
vessel power had been restored. The pilot said
that he was not aware of what, if any, actions
the master or the crew were taking to restore
power. The master’s orders to the second mate
and the second mate’s conversations with the
chief engineer were in Chinese.
The vessel continued to swing to port and
toward the left descending bank. The pilot told
the master to prepare to drop anchors and
ordered the main engine full astern. The vessel’s
bell logger tape, which continuously captures
data and prints it out in 30-second intervals,
recorded that the full-astern order was made
from the bridge at 1409.5 and answered by the
engine control room at 1410.0. The chief
engineer stated that he reversed the engine and
ran the shaft speed to 20 to 40 (fluctuating) rpm
astern.
The pilot stated that, shortly thereafter, he
ordered the anchors dropped. The master said
the pilot ordered only the port anchor dropped,
that he concurred with that order, and that
though he did not acknowledge the order to the
pilot, he attempted to carry it out. The master
said that he attempted to call the carpenter on
the forecastle using the handheld radio. The
carpenter, who was standing by the anchors,
said that he could not hear radio transmissions
from the master because the danger signal was
still being sounded on the ship’s whistle, which
was located about 20 feet above his station on
the bow. The master said he made repeated
unsuccessful attempts to contact the carpenter
but did not ask the pilot to suspend the sounding
of the danger signal. The pilot stated that he
stopped sounding the signal only long enough to
make short radio transmissions to the traffic
light operators to urge them to call the New
Orleans Riverwalk complex and “tell the people
to get away from the dock.”
The master stated that he rushed out to the
port bridge wing and waved his arms to attract
the carpenter’s attention. When he realized that
the carpenter did not see him, the master went
back inside the bridge. Once back inside,
intermittent communications were established
between the master and the carpenter. By the
time reliable communication was established,
the ship had moved farther toward the wharf,
and the master said he believed that dropping
the anchor at that time would cause the ship to
take a sharp turn to the left and perhaps strike
one of the vessels docked there. He said he
therefore told the carpenter not to drop the
anchor. The master said that after the ship had
moved a little farther, he again contacted the
carpenter and told him to drop the anchor to
keep the ship from striking the docked vessels.
The carpenter said he turned the brake wheel to
let go of the port anchor and then ran from the
bow to avoid being injured in the imminent
allision. Postaccident review of an amateur
videotape of the allision indicated that the
anchor did not drop prior to impact.
According to statements of the pilot and
crewmembers, the pilot did not ask either the
master or second mate if the vessel’s power had
been restored or if the anchors had been
dropped, and no one volunteered that
information. The pilot said he had not felt any
engine vibrations, though he expected to. He
said, “When that big engine turns, you feel it.”
The master said the vibrations caused by the
engine when it started in reverse while the ship
was still moving forward were obvious. No
further communications were reported between
the pilot and master or the pilot and the second
mate before the allision.
Meanwhile, the cruise ship
Enchanted Isle
was docked at the Erato Street wharf on the left
descending bank of the river. Passenger
embarkation had begun about 1230, and about
200 passengers were on board. Crewmembers
aboard the cruise ship did not (and were not
required to) monitor VHF channel 67 and
therefore did not hear any radio announcement
from the traffic light operator regarding the
Bright Field
. They did state that they heard the
vessel’s danger whistle. The third officer said he
was on the bridge as the
Bright Field
passed
under the Crescent City Connection Bridges and
that he knew the vessel was in trouble when he
heard its whistle blow for the fifth time. He
stated that he ran out onto the outside deck and
saw the
Bright Field
passing his ship on a direct
path to the Riverwalk area. The ship’s master,
who had also heard the
Bright Field’
s whistle,
reached the bridge as the
Bright Field
went past.
The officers activated the public address system
and placed the bridge on standby to close the
watertight doors. The third officer said that he
and the master called for the forward dock lines

9
to be tightened to protect against gangway
displacement as the
Bright Field
bow wave
struck the vessel. They also notified the
gangway watchman of a possible river surge and
sent two crewmen to watch over the gangway
and report any trouble back to the bridge.
According to the third officer, the
Bright Field
was clear of the
Enchanted Isle
throughout the
accident sequence.
Moored about 150 to 200 feet downriver
from the stern of the
Enchanted Isle
was the
cruise ship
Nieuw Amsterdam
. The ship had
begun embarking passengers about 1330, and an
estimated 200 to 300 passengers were on board
at the time of the accident. The crew did not
(and was not required to) monitor VHF channel
67. The second officer said he was standing
behind the port-side radar when his attention
was drawn to a ship on the river sounding an
emergency alarm. The second officer reported
that he could not immediately determine which
vessel was sounding the alarm, so he and the
chief officer went out to the port side bridge
wing (the vessel was docked with its starboard
side toward the wharf) and saw the
Bright Field
passing under the Crescent City Connection
Bridges. They said they stood and watched the
Bright Field
as it headed toward their ship and
the Poydras Street wharf area. They entered the
wheelhouse to warn the on-duty third officer.
The
Nieuw Amsterdam
’s on-duty third
officer said he also had heard the multiple
whistle signals and had watched the
Bright
Field
as it passed under the bridges with its bow
pointing toward his vessel. He said that the
Bright Field
appeared to be about 1/2 nautical
mile away and moving at 8 to 10 knots. Based
on his observations of the
Bright Field’
s
direction of travel and the whistle sounding, he
said, he assumed the vessel was experiencing
steering or engine failure. He immediately
warned the master, who was in his stateroom
directly behind the bridge.
The
Nieuw Amsterdam
’s master instructed
the on-duty officer to tell the security officer at
the gangway to stop the embarkation of
passengers. The on-duty officer was then to
place the bridge on standby, close the watertight
doors, and activate the public address system.
The master instructed the second and third
officers to go to the stern of the ship with radios
and to evacuate the Lido deck aft, then clear the
decks on the port side and monitor the situation.
The crew said that after 2 or 3 minutes it was
apparent that the
Bright Field
would not strike
the
Nieuw Amsterdam
. The master and the on-
duty officer followed the progress of the
Bright
Field
from the port wing bridge. They assessed
the situation and determined that the
Bright
Field
would miss the
Nieuw Amsterdam
by
approximately 50 meters (164 feet).
The first mate of the gaming vessel
Queen
of New Orleans
, which was docked at the
Poydras Street wharf with its bow less than
1,000 feet downriver from the stern of the
Nieuw Amsterdam
, had overheard the
Bright
Field
pilot’s call to the traffic light operator on
VHF channel 67 (although the vessel was not
required to monitor the frequency) and had
immediately begun emergency evacuation of the
637 passengers and crewmembers aboard the
vessel.
20
Meanwhile, the excursion vessel
C
reole Queen
, which had been docked at the
Canal Street wharf downriver from the
Queen of
New Orleans
, was in the process of pulling
away from the dock with 190 passengers and
crew on board. The master said he heard the
pilot of the
Bright Field
radio the Governor
Nicholls light operator and report, “I’ve lost
everything. The ship is heading toward the
passenger vessels.” The master said that he
returned the vessel to the dock and ordered an
emergency evacuation.
According to the results of Safety Board
surveys, patrons and employees of the
Riverwalk Marketplace along Poydras Street
wharf and the adjacent Julia Street and Canal
Street wharves were unaware of the meaning of
the warning whistles from the
Bright Field
.
Several harbor police officers did recognize the
warning whistles and tried to clear the area.
While they did so, some marketplace patrons
and staff members noticed the
Bright Field
heading toward them, and large numbers began
to flee. Many individuals sustained injuries
during the evacuation. The harbor police were
able to move most of the crowd away from the
expected impact area. Many of those in the area
20
For a detailed discussion of all the vessel
evacuations, see the “Survival Aspects” section of this
report.

10
said that they did not know what was happening,
and because they had had so little advance
notice of a potential hazard, they did not have
the opportunity to obtain information from mall
employees or security officers.
About 1411, the port bow of the
Bright
Field
struck the Poydras Street wharf at a
location between the docked
Nieuw Amsterdam
and
Queen of New Orleans
. (See figure 5.) The
vessel struck the wharf at what witnesses said
was a 40- to 45-degree angle, went into the
wharf up to the end of the forecastle deck (about
50 to 60 feet), and then made a sideways
movement. The bow portion of the vessel
scraped and collapsed portions of the buildings
on the Poydras Street wharf, including a portion
of the Riverwalk Marketplace shopping mall, a
condominium parking garage, and part of the
Hilton Riverside Hotel. The ship came to rest
against the wharf with its stern about 200 feet
from the stern of the
Nieuw Amsterdam
and its
bow about 70 feet from the bow of the
Queen of
New Orleans
. (See figure 6.) The pilot ordered
the engine stopped, after which several tugboats
arrived to hold the ship against the dock. About
3 minutes had elapsed from the time the pilot
made his first emergency call to the Coast Guard
light operator until the ship struck the wharf.
Injuries
The accident resulted in 4 serious and 58
minor injuries to persons in the Riverwalk area,
aboard the
Queen of New Orleans
, or aboard the
excursion vessel
Creole Queen
, which was
docked near the
Queen of New Orleans
. (See
table 1.)
Vessel Damage
After striking the wharf, the bow of the
Bright Field
grated along the concrete and steel
wharf structure for a distance of about 600 feet.
The allision damaged the port side of the bow.
The hull of the vessel sustained two horizontal
gashes about 100 feet long that penetrated the
port side of the ship and extended down the port
side from the fore peak (bow) ballast tank and
into the No. 1 cargo hold. Both the breached
fore peak tank and the No. 1 cargo hold flooded.
A diver found a 100-foot section of the forward
hull resting on the river bottom adjacent to the
Poydras Street wharf. Total damages to the
Bright Field
were estimated to be about $2
million. (See figure 7.) The vessels that had
been docked in the allision area did not sustain
significant damage.
Other Damage
The One River Place condominium
building, located on the Poydras Street wharf,
sustained damage to its valet parking garage.
Residents of the building were evacuated
because of a loss of power and water. The
Riverwalk Marketplace, a mall with 100 stores,
3 restaurants with outdoor seating, and a large
wharf walkway, sustained damage to more than
350 feet of its wharf frontage. About 10 percent
of the mall shops and restaurants were affected.
The New Orleans Hilton Riverside Hotel, part
of which was situated on the Poydras Street
Table 1 -- Injuries Sustained in Bright Field Allision
1
+0,74+'5 4KXGTYCNM"#TGC 3WGGP"QH"0GY"1TNGCPU %TGQNG"3WGGP 7PMPQYP 6QVCN
(#6#. 22222
5'4+175 34326
/+014 38 32 5 4; 7:
010' 52247
616#. 42 34 6 53 89
1
Table
based on the injury criteria (49 CFR 830.2) of the International Civil Aviation Organization, which the
Safety Board uses in accident reports for all transportation modes.

11
N
$/*,(56
3RLQW#
0LOH #<717
0LOH #<8
)HUU\
7HUPLQDO
0,66,66,33,
5LYHU#)ORZ
7R#*XOI#RI
0H[LFR
)HUU \#
7HUPLQDO
&UHROH
4XHHQ
:ROGHQEHUJ
3DUN
:RUOG#7UDGH
&HQWHU#EXLOGLQJ
1121#+LOWRQ
5
L
Y
H
U
Z
D
O
N
4XHHQ#RI#1HZ
2UOHDQV
1HZ#2UOHDQV
&RQYHQW LRQ#)
([KLELWLRQ
&HQWHU
&UHVFHQW#&LW\
&RQQHFWLRQ#%ULGJHV
0LOH
<81:
&
$
1
$
/#
6
7
1
-DFNVRQ#6TXDUH
)UHQFK#4XDUWHU
7
R
X
O
R
X
VH
#
6
W
:K
D
U
I
%LHQYLOOH#6W1
:KDUI
&DQDO#6W1
:KDUI
3R\GUDV#6W1
:KDU I
-XOLD#6W1
:KDUI
(UDWR#6W1
:KDUI
7XJ#/RFNPDVWHU
/RFDWLRQ
1LHXZ#$PVWHUGDP
(QFKDQWHG
,VOH
%
U
L
J
K
W
#
)
L
H
O
G
%
U
L
J
K
W
#
)
L
H
O
G
Fi
g
ure 5 -- Path of Bri
g
ht Field (not to scale)
$
T
XD
U
L
XP


13
Figure 7 -- Damaged Bright Field being towed away from Poydras Street wharf en route to repair
facility, January 6, 1997

14
wharf, sustained damage to 40 of its 1,600
rooms. Total damages to all facilities were
estimated to be about $18 million. (See figures 8
and 9.)
Crew Information
The Pilot
-- The
Bright Field
pilot, age 46,
had been a NOBRA pilot for about 17 years. He
began his maritime career in 1969 when he
started working on the Mississippi River during
college summer vacations. He served as a
deckhand aboard the
Delta Queen
, a
paddlewheel passenger vessel, and as a
deckhand and mate aboard other passenger
vessels, including the
Mississippi Queen
and the
Natchez.
He also worked for a barge line
operating on the Illinois River between St. Louis
and Chicago.
In 1975, the pilot graduated from a 2-year
program at the National River Academy in
Helena, Arkansas. The program consisted of
periods of 2 months of classroom instruction
followed by 2 months on a river vessel. He
obtained his first Coast Guard license, an inland
mate’s license, in 1975. He was commissioned
by the New Orleans Baton Rouge State Pilots
Commission as a pilot on January 16, 1980. At
the time of the accident, he was a licensed river
master and first class pilot. The most recent
renewal of his license had been on May 5, 1995.
The pilot said that he had piloted on most of
the vessel types transiting the Mississippi River.
He said he navigated primarily foreign flag
vessels anywhere from the New Orleans general
anchorage to Baton Rouge. The majority of
these were deep-draft vessels, although he said
he occasionally worked a seagoing tug and
barge. He said he averaged about 7 vessel
assignments per week, totaling between 200 and
300 ships each year. He stated that he had not
attended any ship simulator training, and he
believed that only one NOBRA pilot had
attended such training. He said he had not
received any bridge resource management
(BRM)
21
training and was, in fact, unfamiliar
with the term and the concept.
21
Bridge resource management entails effective use of
all available resources to achieve safe operations.
The pilot stated he had been involved in
three previous accidents. In 1983, the vessel he
was piloting struck a bridge when a
crewmember raised a boom too high. The
second event occurred when the vessel he was
piloting lost steering shortly after he came
aboard. The vessel moved hard to starboard and
hit a ship launch dock. The third event took
place in spring 1996, when the pilot was
working on board a vessel that lost rudder
control and struck the river bank.
For the 4 days prior to the accident, the pilot
said, he had kept essentially the same
sleep/wake schedule, arising shortly after
daylight, about 0700, and retiring between 2230
and 2300. He reported that he had slept well the
night before the accident, did not have any sleep
abnormalities, and did not suffer from any
illnesses. He said he was not sick and that he
had taken no medications on the day of the
accident.
The Master
-- The
Bright Field
master, age
35, had been in the maritime industry for 14
years. He began as an able seaman before
becoming an apprentice officer. He then
progressed from third, to second, to first, to
chief officer, and then to master. He had been a
master for a little more than 1 1/2 years and had
served on three different ships. He said he had
been master of the
Bright Field
for about 15
weeks at the time of the accident (since August
25, 1996). During his time with the
Bright Field
,
he had spent about 3 months at sea and about 1
month in port. He said he had been to New
Orleans twice before, in 1983 and 1989;
however, this was his first trip as master. He
said he had never, on any vessel, experienced a
reduction in engine rpm of the kind that
occurred just prior to this accident.
The master attended the Dalien Maritime
Academy in China for 4 years and graduated in
August 1982. His training involved more than
40 deck officer-related courses. It also included
computer-based simulator training in ship
handling and maneuvering. He said he had
received additional simulator training on two
occasions at the Qingdao Mariner’s Training
School. The first occasion involved radar
plotting and ship handling to qualify for his
radar observer’s endorsement. The second
involved the handling of large vessels and

15
Figures 8 and 9 -- Postaccident scenes

16
occurred after he had passed his master’s
examination.
The master held a People’s Republic of
China Marine Certificate of Competency, which
certified that he was qualified to be a master of
ships of 1,600 gross tons or more. The most
recent endorsement of that certificate had been
on April 20, 1995. He also held a Republic of
Liberia license certifying his competence as a
master and radar observer on oceangoing vessels
of any gross tonnage. The most recent
endorsement of that license had been on October
3, 1996. Both licenses are valid for 5 years.
The master indicated he had received
training that emphasized coordination among
the bridge team, including the pilot. He said his
training covered the duties and responsibilities
of each individual and stressed the need to be
able to communicate with one another and assist
one another in the performance of their duties.
He said the training also stressed the integration
of the various responsibilities.
The master noted that, since he had held the
position of master, he had overruled pilots on
four occasions. On this trip he said,
I…instructed the carpenter not to drop
the anchor, which in effect…overruled
the pilot, because the pilot [had]
instructed [me] to drop the anchor. [I]
instructed the carpenter not to drop the
anchor because [it] would [cause the
Bright Field
to] swerve towards the
passenger ship. That, in effect, is a way
of overruling the pilot.
The master said he did not confer with the
pilot about the change in the timing of the drop-
anchor order because there was “no time.”
The master reported that he began to learn
English when he entered the maritime academy.
He characterized his English language skills as
“not bad among Chinese,” though he noted that
his ability to read the language was better than
his ability to speak it. He said he did not have
any difficulty understanding the pilot on this
trip.
The master stated that he was required to be
available 24 hours a day but that his normal
schedule involved going to bed at midnight and
arising at 0700 each day. He said he had kept
this schedule on the night before the allision,
arising about 0715 after a complete night’s
sleep. He reported that he was not suffering
from any long-term illnesses and that he was not
sick and took no medications on the day of the
accident.
The Chief Engineer
-- The
Bright Field’
s
chief engineer, age 34, began his maritime
career in 1979. He studied marine engineering at
the Jimei Maritime School, graduating in 1982.
He said he had been sailing aboard ships as an
engineer since his graduation. He said he had
been a chief engineer for 4 years, had been with
his current employer for 1 month, and had been
chief engineer aboard the
Bright Field
for 3
weeks prior to the allision. He came aboard the
Bright Field
for the first time on November 21,
1996, to replace the vessel’s previous chief
engineer (see below), who had been relieved of
duty upon the vessel’s arrival in New Orleans.
The chief engineer stated that he had served
on ships with both more and less automated
engineering equipment than the
Bright Field
and
that he was comfortable with the
Bright Field
’s
automation. He also said he had received
training on automated ship systems at the Dalien
Maritime Academy in 1993 and that the last
ship he served on before the
Bright Field
was
equipped with a similar system. While aboard
the
Bright Field
, he had been underway on short
transits on four occasions for a total of 11 hours.
During those occasions he said there were no
engine casualties or automation problems,
although various main engine repairs had been
made while the ship was at anchor during the 3
weeks he had been aboard.
The chief engineer held a People’s Republic
of China Marine Certificate of Competency,
which certified that he was qualified as a chief
engineer of ships of 3,000 kw (kilowatt, or
4,023 hp) propulsion power or more. The most
recent endorsement of that certificate had been
on October 27, 1993. He also held a Republic of
Liberia license certifying his competence as a
chief engineer on motor vessels of any
propulsion power. The most recent endorsement

17
of that license had been on May 23, 1995. Both
licenses are valid for 5 years.
The chief engineer reported that his normal
work day began at 0800 and ended at 1700. His
normal sleep schedule was to go to bed at 2300
and arise at 0700. In the 2 days prior to the
allision, the
Bright Field
was at anchor, and the
engineer was involved in some repairs. On
December 12, the turbocharger was repaired.
Work began in the evening and was completed
at 0220 the following morning, December 13.
The chief engineer said he then went to bed and
got up shortly after 1000. That night he went to
bed before 2300 and was awakened just after
0600 on December 14 by the air cooler
technician, who needed his signature. He said he
remained awake, but he did not actually start
working for the day until about 0920.
The chief engineer reported that he was not
suffering from any long-term illnesses and that
he was not sick and had taken no medications on
the day of the accident.
The Previous Chief Engineer
-- The
vessel’s previous chief engineer had joined the
Bright Field
in April 1996. He left the vessel in
New Orleans on November 21, 1996, after being
fired for what a company representative said
was his failure to comply with company orders
about the maintenance and operation of the
Bright Field’
s engineering plant.
Vessel Information
Four vessels were docked near the point at
which the
Bright Field
struck the wharf. The
Enchanted Isle
was docked at the Erato Street
wharf, and the
Nieuw Amsterdam
was docked at
the Julia Street wharf. The gaming vessel
Queen
of New Orleans
was docked at the Poydras
Street wharf in front of the Hilton Riverside
Hotel. The excursion vessel
Creole Queen
was
docked at the Canal Street wharf.
Bright Field
--The
Bright Field
, a bulk
cargo carrier with seven cargo holds, was built
in 1988 by Sasebo Heavy Industries Co. Ltd., of
Japan. At the time of the accident, the ship was
owned by Clearsky Shipping Company, a
Liberian corporation, and operated by Cosco
H.K. Shipping Company, of Hong Kong. The
Liberian-registered vessel was 735 feet long,
weighed 68,200 deadweight tons, and had a
maximum breadth of 106 feet.
The
Bright Field
was classed
22
by Det
Norske Veritas (DNV) for periodically
unattended machinery space. When the
Bright
Field
was delivered, the original owners elected
to have the unattended machinery space en-
dorsement include specifications for preventive
maintenance and routine testing of automatic
propulsion system components, and the
procedures were verified periodically by DNV.
The current owner of the vessel elected not to
continue the preventive maintenance
endorsement of the original class certification.
The vessel was equipped with an IHI Sulzer
RTA62 slow-speed, five-cylinder, two-cycle,
turbocharged, reversible diesel engine
manufactured by Ishikawajima-Harima Heavy
Industries (IHI) of Aioi, Japan. The 9,655-brake
hp (7,200 kw) engine was directly coupled to a
24-foot-diameter, four-blade, bronze propeller
capable of driving the vessel to a speed of 15.5
knots at sea speed.
23
A change from ahead to
astern required that the engine be stopped and
restarted with shaft rotation in the opposite
direction. A high-pressure compressed-air
system was used to start the engine in either
direction and also to stop its rotation during a
change from ahead to astern or vice versa.
The
Bright Field’
s engine was fitted with
protective devices (alarms and shut downs),
sensors (pressure, temperature, etc.), and
automatic control equipment. In support of
unattended machinery operation, the vessel was
equipped with engine controls located on the
bridge.
The
Bright Field
was configured as a
conventional bulk carrier with an aft
engineering plant and accommodation house.
The navigation bridge was fitted with a chart
table, navigation equipment, and an automatic
22
6JG" CRRNKECDNG" &08" TWNGU" KPEQTRQTCVGF" VJG
+PVGTPCVKQPCN" #UUQEKCVKQP" QH" %NCUUKHKECVKQP" 5QEKGV[IU
*+#%5+"WPKHKGF"TWNGU"CPF"VJG"
International Convention for
the Safety of Life at Sea
(SOLAS),
%JCRVGT"33/3."2CTV"'0
23
Because of the relatively rapid river current on the
day of the accident, the
Bright Field
was traveling at an
effective speed that exceeded its rated sea speed.

18
radar plotting aid (ARPA)
24
in its after part.
Facing toward the bow, forward of the chart
table to starboard of centerline, was the engine
control console with engine order telegraph. To
the left of the console on the centerline was the
helm control console, comprising the helm, gyro
compass, and magnetic periscope compass.
Forward of the console and suspended from the
overhead was a rudder angle indicator and
engine order indicator. Below the forward
bridge windows was a gyro repeater, radar, VHF
marine radio, and manual buttons for the ship’s
whistles.
Although not required by U.S. or Interna-
tional Maritime Organization regulations, the
vessel was equipped with a course recorder. In-
vestigators determined that, at the time of this
accident, the unit was inoperative because of
leaking graph recording pens. Examination of
the course recorder paper determined that the
unit had probably been out of service for some
time. When in working order, the unit records
the ship’s gyro heading over time.
The vessel was equipped with an engine
telegraph logger that automatically recorded
engine telegraph orders (date and time) from the
bridge and acknowledgments of the orders from
the engine control room. The logger also noted
whether the engine was being operated from the
control room or wheelhouse. The time units
were recorded in hours, minutes, and half
minutes. The unit did not record the ship’s
actual engine rpm.
Automated Propulsion Control System
-- The
automated propulsion control system aboard the
Bright Field
used components from a number of
manufacturers, the primary two being IHI,
which provided the main engine control system,
and Terasaki, which provided the engineering
plant monitoring, alarm, and recording systems.
Most remote control functions affecting the op-
eration of the main engine, including the
automatic engine trip features, passed through
the IHI control system. Dual independent
Terasaki computers and monitors received sig-
nals from sensing probes on engineering plant
equipment and provided a status report,
24
ARPAs are computer-based devices that process
radar signals and display selected navigation information.
including operating and fault conditions.
Conditions falling outside the acceptable oper-
ating ranges were alarmed to appropriate
watchstanding and engineering personnel.
Sasebo Heavy Industries, the ship’s builder,
assembled and connected the various
components of the automated propulsion control
system, including the bridge and engineering
remote control consoles.
The
Bright Field’
s automated propulsion
control system provided for operation of the
main engine through use of either electro-
pneumatic controls from the wheelhouse or
pneumatic controls from the control room. The
engine could be controlled from the bridge using
a single maneuvering lever, which also acted as
an engine telegraph transmitter. Although the
bridge controls allowed the
Bright Field
engineroom to be unattended, company policy
required that the engine control room be
attended during operation in restricted waters
such as the Mississippi River. Although each
operating location was equipped with certain
engine function controls that were not available
at the other location, the main engine could be
started, stopped, reversed, accelerated, or
decelerated from either the wheelhouse or the
control room. Both control locations could
provide main engine throttle control over the
vessel’s two speed ranges: maneuvering mode
(from dead slow speed of 30 rpm to full speed
of 56 rpm) and sea mode (speeds up to the
maximum of 72 rpm).
During normal operations, the rate at which
the rpm of the
Bright Field’
s main engine could
be increased was subject to limitations imposed
by two independent components of the
automated propulsion control system: an
acceleration-limiting program and a scavenging
air pressure
25
limiter.
The automatic acceleration-limiting
program could be activated when the engine was
being operated in wheelhouse control. The
program allowed engine rpm to increase only
gradually, in accordance with a programmed
(variable) acceleration rate. The wheelhouse
control operator could activate a switch to
25
Scavenging air
is that air used to evacuate exhaust
gasses from the engine’s cylinders after combustion.

19
bypass this program when engine speed needed
to be increased quickly. The acceleration-
limiting program was automatically bypassed
when the engine was being operated from the
engine control room.
The scavenging air pressure limiter
functioned to reduce main engine exhaust
emissions. Overriding the limiter injected more
fuel into the engine, thereby increasing engine
rpm at a slightly faster rate. The limiter was
automatically overridden whenever wheelhouse
controls were moved to “crash (emergency)
ahead” or “crash astern.” Also, a crash
maneuvering pushbutton on the engine control
room console enabled engineering personnel to
override the scavenging air pressure limiter if
necessary. According to the second engineer,
the crash maneuvering pushbutton was used
only on the orders of a bridge officer, and such
an order was not given on the day of the
accident.
Transfer of engine operating control to or
from the wheelhouse and engine control room
required communication and coordination
between bridge and engine control room
personnel. Transfer of propulsion control was
physically initiated by the engineer in the
control room, who first matched control settings
in the control room with those on the bridge,
then set a selector switch to the desired mode.
Transfer of control was completed when a
crewmember in the wheelhouse pressed a button
on the bridge to acknowledge the transfer.
According to the
Bright Field
chief engineer,
the transfer normally required 20 to 30 seconds
from the time of the initial decision to make the
transfer until the changeover was accomplished.
This time was confirmed in postaccident testing.
Audible and visual alarms on the bridge and
in the engine control room were designed to
activate in the event of the following emergency
conditions: start failure (wheelhouse only),
emergency manual stop, automatic emergency
trip, automatic slowdown, low control air
pressure, low starting air pressure, control
power failure, telegraph power failure, and
automatic failure of wheelhouse controls (auto
control failure).
Automatic engine slowdown interrupts and
automatic engine trip due to high cooling water
temperature could be overridden without the
fault having been corrected. The other main
engine trips, including trips resulting from low
lubricating oil pressure, required that the faults
be corrected before engine operation could be
resumed.
Engine Lubricating Oil System
-- The main
engine lubrication oil system circulated 30-
weight high-detergent oil from the 14-cubic-
meter (about 3,700 gallons) sump located in the
main engine foundation. A suction line picked
up the oil from the sump and delivered it to two
separate oil lines. These oil lines passed the oil
through wire mesh basket strainers before
delivering it to two (designated as No. 1 and No.
2) high-capacity (180 cubic meters, or 47,550
gallons, per hour) lubricating oil pumps. (See
figure 10.) Each pump was capable of boosting
the oil pressure to approximately 4 bar.
26
The
discharge piping from each pump met at a
26
One bar is equal to .995 kg/cm
2
or 14.5 psi.
Figure 10 --
Bright Field
No. 1 (left) and No. 2
lubricating oil pumps

20
common header, from which the oil passed
through an oil cooler and a second filter. In the
second filter, the oil was passed through 16 fine-
mesh cylindrical strainers. At this point, the
system pressure would have dropped by
approximately 1/2 to 1 bar. Various oil
temperature and pressure sensors monitored the
condition of the oil and signaled the status to the
automated control system. After being
circulated through the engine, the lubricating oil
drained back into the crankcase sump, where the
cycle began again. A separate lubricating oil
purification system drew warm oil from the oil
sump, passed it through a centrifugal separator
where water and contaminants were removed,
and then returned the cleaned oil to the main
engine sump.
The chief engineer stated that the standard
configuration for maneuvering the
Bright Field
in restricted waters included remote engine
control from the wheelhouse, the No. 1
lubricating oil pump running, and the No. 2
lubricating oil pump on standby. If the
automated propulsion control system detected
main engine lubricating oil pressure below 2.5
bar, it was designed to sound and display an
alarm in the engine control room, on the bridge,
and in various locations in the accommodation
spaces. If the pressure dropped below 2.4 bar, a
pressure-activated changeover switch would
signal the automated control system to start the
standby oil pump. If the pressure dropped below
about 2.3 bar, the control system would, after a
brief time delay, trip (shut down) the main
engine.
Cruise Ships
-- The cruise ships at the Julia
and Erato Street wharves were normally moored
at this location on weekends to disembark and
embark passengers and to load supplies. The
cruise ship
Enchanted Isle
was owned by
Almira Enterprises, Inc., and operated by New
Commodore Cruise Lines, Inc. The vessel, built
in 1958, was 574 feet long and was 13,681 gross
tons. It was powered by a steam turboelectric
propulsion system. Maximum capacity was
1,198 persons.
The
Nieuw Amsterdam
, moored at the Julia
Street wharf, was owned by Hal Antillen, Inc.,
and operated by Holland America Line
Westours, Inc. The 704-foot, 16,027-gross-ton
vessel was built in 1983 and was powered by a
direct-drive diesel engine.
Gaming and Excursion Vessels
-- The
Queen of New Orleans
was owned by Hilton
New Orleans, Inc., and New Orleans
Paddlewheels, Inc., in an association known as
Queen of New Orleans Joint Venture. The
vessel operated from a dock located at the
Poydras Street wharf, on the riverfront behind
the New Orleans Hilton Riverside Hotel and
Riverwalk Marketplace. The vessel conducted
eight scheduled 90-minute cruises each day. The
vessel left its docking facility at the wharf every
3 hours, beginning each day at 0245 and ending
at 2345. Passengers were allowed on board for
gambling 45 minutes prior to and 45 minutes
after each cruise.
The six-deck, 1,470-gross-ton, 245-foot-
long vessel was built in 1993. It was powered by
a Sternwheeler Propulsion System paddlewheel.
Capacity was 300 crew and 1,500 passengers,
for a total capacity of 1,800. The master of the
vessel stated that the vessel had four decks
accessible to passengers. The first three decks
were all gaming areas; the fourth had a forward
café and an aft gaming area. On a normal day,
about 20 percent of the passengers would be on
the first deck. The most crowded deck would be
the second deck, with about 40 percent of the
passengers. About 30 percent of the passengers
would be on the third deck, with only about 10
percent on the fourth deck. At the time of the
accident, 637 persons were on board, including
14 marine crew, 96 gaming personnel, 38
security, nongaming, and miscellaneous
personnel, and 489 passengers.
The
Queen of New Orleans
master stated
that, on the day of the accident, the vessel was
not scheduled to leave the dock. Under normal
operations, if the river stage is “8 feet and
rising,” the vessel remains at the dock. New
Orleans Paddlewheels, Inc., has stated that the
vessel:
Does not leave the dock for regularly
scheduled cruises during foul weather,
including rain, thunderstorms, showers,
hail, fog and mist and wind conditions
in excess of 12 mph. Additionally, the
vessel does not sail during seasonal high
river stage when the Governor Nicholl’s

21
traffic light is in operation.
27
Finally, the
Queen of New Orleans
remains at dock
during port closures issued by the
Marine Safety Office. When the vessel
is dockside, the vessel remains open for
business and passengers are permitted to
remain on board.
According to the Board of Commissioners
of the Port of New Orleans (Dock Board), the
provisions of the Dock Board’s Emergency
Management Checklist and Guidelines were
applied to the
Queen of New Orleans
gaming
vessel and its shoreside terminal as part of a
permit process. The facilities and operations
were reviewed by a Dock Board consultant prior
to approval of the permit and found to be in
compliance with the guidelines.
The 3-deck, 397-gross-ton
Creole Queen
, a
1,000-passenger-capacity paddlewheel excur-
sion vessel, was 190 feet long and 40 feet wide.
It normally departed the Canal Street dock for
two daily sightseeing trips and one nightly
dinner cruise. The overnight mooring location
for the vessel was the Poydras Street wharf ad-
jacent to the office of New Orleans
Paddlewheels, Inc., the vessel’s owner. The
berth was destroyed as a result of being struck
by the
Bright Field
. After the accident, the
overnight mooring location was moved to the
Canal Street wharf.
Waterway Information
According to information provided by the
U.S. Army Corps of Engineers, the Mississippi
River has a Federal project depth of 45 feet from
over the bar at Southwest Pass thence to the head
of the passes and to mile 233.4 AHP, or about
135 miles above New Orleans. Various areas of
the Federal project are under constant
maintenance dredging. Southwest Pass has a
recommended draft limit of 45 feet.
According to records supplied to the Safety
Board by the Corps of Engineers, between 1983
and 1996, mean monthly water temperatures in
27
The company has told the Safety Board that since
this policy was developed, the traffic lights have been
placed in full-time operation; consequently, the policy is
now interpreted to refer to those times (high water stage)
when the traffic lights are actually controlling river traffic.
the Mississippi River ranged from a low of 43.2
°
F in January to a high of 83.3
°
F in August.
Mean water temperature over the period for the
month of December was 49.6
°
F.
River Stage
--
On average, high river stage
occurs in April and the low river stage in
October. At New Orleans, the extreme
difference between high and low stage is 17
feet; the mean difference is about 8 feet. At
several places in the lower part of the river,
counter currents or eddies often are found near
the banks. This occurrence is especially
pronounced in the area of Algiers Point.
Records maintained by the Corps of
Engineers indicated that the Carrollton gauge at
mile 102.8 AHP on December 14, 1996, read
12.5 feet (above a datum at New Orleans) and
was falling. Based on this reading, the Corps of
Engineers’ best estimate of the current below the
Crescent City Connection Bridges in the area of
the accident on December 14, 1996, was 4.5 mph.
At times of extremely high river stage, the
Corps of Engineers has the option of opening
the Bonnet Carré Spillway, which, by diverting
1/4 million cubic feet of water per second
through the spillway, lowers the river by
approximately 4 feet while reducing the speed
of the current. According to the Corps of
Engineers, the spillway, located about 33 miles
above Canal Street, was built in 1932 to protect
communities downstream of the spillway from
floods, and to lower river stages generally, by
discharging floodwaters into Lake
Pontchartrain, then into the Gulf of Mexico.
According to the Corps of Engineers, under
normal operating conditions, opening the
spillway is a complex task that requires about 36
hours to complete. Prior to the
Bright Field
allision, the spillway had been opened seven
times since its construction, the last time in
1983.
28
Vessel Traffic Control
-- The only
operational vessel traffic control system serving
28
During what the Coast Guard termed
“unprecedented high waters on the Mississippi River” in
early 1997, the Bonnet Carré Spillway was opened for the
eighth time on March 17, 1997, to lower the water level
and combat strong river currents. The spillway remained
open until April 18, 1997.

22
the Mississippi River in the New Orleans area is
a series of traffic lights operated by the Coast
Guard. When the river reaches 8 feet on the
Carrollton gauge on the rising stage, and until
the gauge reads 9 feet on a falling stage, the
movement of all tugs with tows and all ships,
whether under their own power or in tow (but
excluding tugs or towboats without tows or river
craft of comparable size and maneuverability
operating under their own power) in the vicinity
of Algiers Point is governed by the Coast
Guard’s Governor Nicholls and Gretna traffic
lights. The lights are visible throughout the
entire width of the river and flash once every
second. A green light displayed ahead of a
vessel (in the direction of travel) indicates that
Algiers Point is clear and the vessel may
proceed. A red light displayed ahead of a vessel
(in the direction of travel) indicates that Algiers
Point is not clear and the vessel is not to
proceed.
Port Information
29
More than 6,000 oceangoing ships and
120,000 barge and tows travel through the Port
of New Orleans
30
each year. The port is
primarily a general cargo port. The frontage for
deep draft vessels within the port limits includes
approximately 34 miles along the riverbanks.
The city of New Orleans is the major
commercial area within the port limits. The Port
of New Orleans has more than 28 miles of
public and private wharves and related facilities.
The public docks can handle as many as 85
ships at a time.
Most of the wharves along the New Orleans
waterfront are public facilities under the control
of the Dock Board. The Dock Board consists of
members selected by the Governor of Louisiana
from a list of nominees compiled by 18 business
and civic associations. The Dock Board
maintains the depths of vessel berths adjacent to
its public wharves from the face of the wharf to
29
Information obtained from United States Coast Pilot
5, from the Dock Board, and from other local and national
reference sources.
30
The Port of New Orleans extends along both sides of
the river from mile 80.6 AHP to mile 115 AHP, and
encompasses the city of New Orleans, several parishes or
the river frontage of those parishes, and a number of
smaller communities.
100 feet into the river and assigns vessel berths
at its public wharves. The Coast Guard is
primarily responsible for control of navigation
in the river, and the Corps of Engineers is
primarily responsible for approving new
structures in or on the river.
Subject to the above Federal jurisdictions,
the Dock Board regulates activities related to
maritime commerce within the Port of New
Orleans and administers, controls, and regulates
the public wharf facilities in the port. About 3/4
of the wharf frontage is owned by the Dock
Board and operated by private operators under
occupancy agreements from the board.
Above New Orleans, the Mississippi River
is used by oceangoing vessels to Baton Rouge,
about 135 miles above Canal Street in New
Orleans. The river channel between New
Orleans and Baton Rouge for the most part is
deep and clear. Facilities on the Mississippi
River above New Orleans to Baton Rouge
include private and public terminals for
handling oil and other products on both sides of
the river.
The Erato and Julia Street wharves, adjacent
to the Poydras Street wharf, were used for
docking cruise ships from the Holland America,
Carnival, and New Commodore cruise lines, as
well as U.S. Navy ships and, during annual
Mardi Gras
, additional tourist ships, some of
which were used as hotels. The wharf area had
two passenger terminal buildings, a parking lot,
and harbor police facilities. This wharf area was
accessible only when cruise ships were at berth
and was the only open public area not managed
by a commercial tenant. Port of New Orleans
Harbor Police officers were detailed to the area
and monitored police radios. In the event of an
emergency, the harbor police officers provided
evacuation direction and assistance in the cruise
terminal area. The remainder of the Port of New
Orleans public areas were under the control of
the renters or lessees.
Dredging
-- The Dock Board is responsible
for dredging New Orleans Passenger Terminal
(passenger/cruise ships) and Riverwalk piers to
a distance of 100 feet out from the pier face. On
December 11, 1996, maintenance dredging was
completed in the Riverwalk Marketplace and
New Orleans International Terminal areas. The

23
Dock Board specified that the dredging would
extend to a 33-foot project depth. The passenger
terminal was dredged only to a depth sufficient
to accommodate the cruise ships that docked
there. At the time of the accident, the depth was
sufficient to accommodate the
Enchanted Isle
,
which had a draft of 28 feet. The docking area
of the
Queen of New Orleans
had not been
dredged since 1994 and had been left to silt in to
afford the vessel protection from ramming by
deep-draft vessels. With the silting, water depth
in the docking area was about 15 feet in average
river stage conditions. Because of the dredging
and the high river stage that existed on
December 14, 1996, the river was 45 to 48 feet
deep alongside the Poydras Street wharf in the
area of the Riverwalk Marketplace at the time of
the accident.
The Wharf Area
-- According to the Dock
Board, the Canal, Poydras, and Julia Street
wharves were constructed early in this century.
The wharves have been renovated or rebuilt
several times since their original construction,
but always on the same “footprint.” All of the
substructure and first level decks of the wharves
were designed and built, and are currently
owned, by the Dock Board. In 1977, the
International RiverCenter (IRC) constructed a
cruise ship terminal on the first level of the
Upper Poydras Street wharf. The terminal was
built in conjunction with the development of the
first phase of the Hilton Hotel. In 1983, the IRC
completed the riverside expansion of the Hilton
Hotel, which was constructed on old warehouse
piers on the river side of the levee flood wall.
No additional footings or wharf extensions were
erected beneath or beyond the original piers at
the site of the Riverwalk complex.
In the early 1980s, the Louisiana World
Exposition (LWE) selected the Upper Poydras
Street, Julia Street, and Erato Street wharves as
locations for the world’s fair’s riverfront
attractions. The last full year of cargo operations
at these wharves was 1981. In the LWE’s lease
agreement of July 1982, the Dock Board agreed
to discontinue cargo operation and assignment
of lay-up vessels at the Julia, Poydras and Erato
Street wharves between May 1 and November
15, 1984. The Dock Board’s lease with the
LWE required that the first 15 feet of the
wharves be kept unobstructed and inaccessible
to the public. Existing structures on the Julia
Street, Poydras Street, and Erato Street wharves
were significantly modified by construction of
facilities for the world’s fair, however, the
wharf deck profiles were not changed.
In 1986, the Rouse Company developed the
Riverwalk mall on portions of the Lower
Poydras, Upper Poydras, and Julia Street
wharves. The Rouse Company leased the land
rights from the IRC and the city of New
Orleans. The Rouse Company was required to
obtain construction permits for the Riverwalk
Marketplace from the city of New Orleans and
the New Orleans Levee Board. Rouse was
granted a consent agreement from the Dock
Board to construct and operate the Riverwalk
Marketplace. The Dock Board reviewed the
Riverwalk mall plans to determine the extent to
which the development might affect Dock Board
activities.
The One River Place condominium parking
garage was constructed above the lower Poydras
Street wharf and above the Riverwalk
development. The condominiums were
completed in 1989. One River Place was given a
lease agreement from the Dock Board to
construct and operate the condominiums. One
River Place was required to obtain all
appropriate city building permits.
In 1993, the Julia Street wharf cruise ship
terminal was opened, replacing the original
terminal constructed by the IRC. Also in 1993,
the Queen of New Orleans Joint Venture
widened a part of the Poydras Street wharf by
50 feet and constructed a boarding tower on the
wharf to accommodate a riverboat-style gaming
vessel. (See figure 11.) The widened wharf and
the addition of a boarding tower were permitted
by the Army Corps of Engineers, the Dock
Board, and the city of New Orleans. No barriers
were constructed outboard of these structures.
The construction of wharves extending into
the navigable waters of the United States is
subject to approval and issuance of a permit by
the Corps of Engineers. The Corps of Engineers
relies on the Coast Guard for any navigational
safety concerns that such constructions may
raise.
Federal Jurisdiction
-- While the Coast
Guard is responsible for promoting the safety of
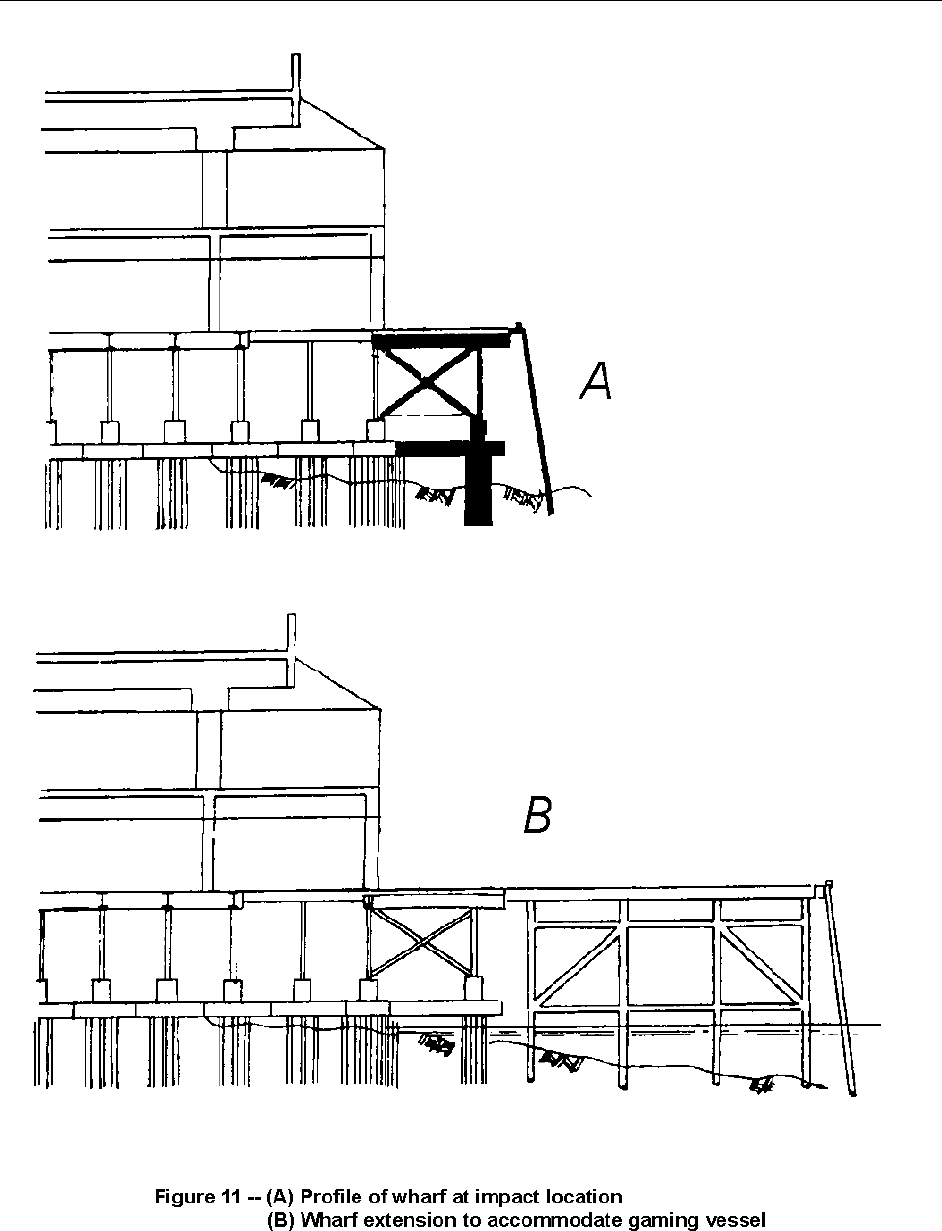
24

25
life and property on the navigable waters of the
United States, the Corps of Engineers has final
authority to approve any structure built on or in
the navigable waters of the United States,
including the Mississippi River. A permit from
the Corps of Engineers is required to situate a
structure in or on any navigable waterway.
Under the
Rivers and Harbors Act of 1899
, the
Corps has jurisdiction over the establishment of
harbor lines and anchorages and the
maintenance of clear passage along navigable
waterways. A permit is required to construct
piers, wharves, jetties, permanent moorings,
permanently moored floating vessels, or any
other permanent or semipermanent obstacle or
obstruction.
Meteorological Information
At the time of the accident, winds were from
the east at 6 knots; clouds were scattered;
visibility was 7 miles; the temperature was 70
°F.
31
Toxicological Information
Postaccident alcohol and drug tests were
conducted after this accident on the pilot and
nine crewmembers who were on duty at the time
of the accident.
32
Testing was ordered for
crewmembers assigned to the noon watch. The
ship’s carpenter, who was acting as anchor
watch at the time of the accident, was not
assigned to the noon watch and was not tested.
The crew’s tests were conducted by a
specimen collection and testing company
retained by the ship’s agent. The breath tests,
using a portable testing device taken aboard the
ship, began at 2036, 6 hours and 25 minutes
after the accident. The last three tests done were
those of the helmsman at 2208, the master at
2235, and the chief engineer at 2241. These tests
were conducted 7 hours 57 minutes, 8 hours 24
minutes, and 8 hours 30 minutes, respectively,
after the accident. The results of all nine tests
31
As reported from the Naval Air Station, Belle Chase,
Louisiana.
32
The master, second mate, helmsman, bridge lookout,
chief engineer, second engineer, third engineer, electrician,
and motorman.
showed 0.00 percent blood alcohol
concentration (BAC).
The same collection and testing company
collected urine specimens from the nine
crewmembers between 2030 and 2230. The
specimens were sent to a Federally approved
testing lab in New Orleans and tested for the
presence of five categories of illicit drugs
specified in Coast Guard and Department of
Transportation regulations.
33
The specimens
were negative for the five drugs for all the tested
crewmembers.
The Safety Board requested a portion of the
specimens that remained after the lab completed
its testing. Those portions were forwarded to the
Center for Human Toxicology (CHT) in Salt
Lake City for additional testing. The second
testing confirmed that none of the five groups of
illicit drugs, nor any other drugs, were present in
the specimens. In addition, tests for urine
alcohol concentration were negative for all
specimens. Traces of caffeine and/or smoking
byproducts were the only chemicals found in
some specimens.
Urine and breath specimens for postaccident
alcohol and drug testing were obtained from the
pilot about 1 1/2 hours after the accident (at
1537 and at 1550, respectively). Results showed
a BAC of 0.00 percent and were negative for the
five groups of illicit drugs tested. Additional
testing requested by the Safety Board was
conducted on a portion of the urine specimen by
CHT. Caffeine was the only drug found in the
pilot’s specimen.
Coast Guard postaccident drug and alcohol
testing regulations (46 CFR Parts 4 and 16 and
33 CFR Part 95) require specimen collection to
occur “as soon as practicable following an
accident.” The chronology of specimen
collection in this accident (based on
recollections of the individuals involved) is as
follows:
1530 Ship’s agent learns of accident from the
vessel charterer.
33
The drugs specified in 49 CFR Part 40 are
marijuana, cocaine, opiates, amphetamines, and
phencyclidine.

26
1600 Coast Guard investigator on board ship.
Pilot not aboard. NOBRA was called to
ensure pilot was tested. NOBRA states
that testing was in progress. Investigator
looks for, but finds no evidence of
alcohol or drug impairment among crew.
1630 Ship’s agent representative on board.
Ship’s attorney on board.
1700 Coast Guard Marine Safety Office
(MSO) investigator orders ship’s
attorney to test crew for drugs and
alcohol.
1730 Ship’s agent general manager on board.
1834 Specimen collection and testing company
contacted by general manager when he
learns that the Coast Guard was
expecting the ship to call the drug testing
company.
1955 First of two collectors arrives at scene.
2010 First collector arrives on board ship after
difficulty getting past road blocks.
2030 First specimen taken.
2235 Second collector on board.
2245 Breath testing and urine specimen
collection complete.
Survival Aspects
Bright Field
-- The vessel master said the
crew was trained to respond to a particular
emergency alarm that is sounded in case of a
fire, a pollution incident, or other emergency.
The response normally entailed reporting to the
main deck. The master stated the most recent
fire and boat drill held aboard the
Bright Field
,
in accordance with international and Republic of
Liberia rules, was on November 17, 1996. He
said fire and boat drills included the sounding of
the emergency alarm and were normally held
weekly.
Enchanted Isle
-- The Port of New Orleans
Harbor Police arrived at the
Enchanted Isle
gangway a few moments after the
Bright Field
struck the wharf and requested that passenger
embarkation be stopped. Embarkation was
delayed 4 to 5 minutes as the river surged and
the situation was assessed. According to
witnesses, the gangway moved up and down
briefly with the swells, but no passengers were
on it at the time.
Nieuw Amsterdam
-- After the
Bright Field
impact, the second officer of the
Nieuw
Amsterdam
radioed the bridge that the
Bright
Field
had stopped moving and was
approximately 50 meters from the stern of the
Nieuw Amsterdam
. He said later he recalled
seeing tugboats arrive within moments to keep
the
Bright Field
stable against the wharf. He
said he reported to the bridge by radio that the
Bright Field
no longer posed a danger to the
Nieuw Amsterdam
, after which he returned to
the bridge. Upon receiving the radio call, the
third officer and the master assessed the
situation and returned the ship to its normal
operations.
At the Safety Board’s request, the master of
the
Nieuw Amsterdam
distributed a
questionnaire among the ship’s passengers.
While the actual number of passengers who
received the questionnaire is unknown, 137 of
them responded. Their responses are the source
of the information that follows.
Numerous passengers who were on the
Nieuw Amsterdam
at the time of the accident
observed the
Bright Field
as it passed by the
ship before hitting the wharf. These passengers
were on the Lido deck, port side. They said they
heard the vessel’s whistle, then noticed its
direction and speed. As the
Bright Field
passed
the
Nieuw Amsterdam
, most of the passengers
ran aft on the Lido deck, observed the
Bright
Field
strike the wharf, and watched the
emergency responders arrive.
Several passengers were on the
Nieuw
Amsterdam
gangway at the time the
Bright
Field
was approaching the Poydras Street wharf.
One couple first noticed the
Bright Field
as it
passed under the bridge because it was
repeatedly sounding its whistle, and they
became aware that the vessel was experiencing
problems because of the angle of its approach.
When they and other passengers were about
halfway up the gangway, ship personnel
instructed them to turn around, exit the

27
gangway, and return to the terminal. After the
Bright Field
struck the wharf, cruise terminal
employees instructed them to go into the
terminal for their own safety.
Another couple was on the dock when they
heard the
Bright Field’
s whistle, but they did
not understand its significance. They observed
harbor police scooters driving past them with
lights and sirens on. After the accident, cruise
terminal employees directed them to return to
the terminal, where they remained until they
boarded the
Nieuw Amsterdam
about 1/2 hour
later.
Other passengers were in the port terminal
when the
Bright Field
struck the wharf. They
were instructed to remain against the far side of
the terminal and became aware of an emergency
when they heard the
Bright Field’
s whistles,
observed harbor police officers moving toward
the wharf, and saw people begin “streaming” out
of the Riverwalk Marketplace. Although most
responding passengers recalled that emergency
responders arrived quickly, others recalled that
some time elapsed before emergency personnel
arrived.
Queen of New Orleans
-- The first mate on
the
Queen of New Orleans
(figure 12) stated that
he was monitoring channel 67 when he heard
the call from the
Bright Field
pilot to the
Governor Nicholls Light operator. He said he
immediately notified the master, who was on the
aft portion of the main deck. The master stated
that, when he approached the stairs to the
pilothouse (on the main deck forward), he noted
the
Bright Field’
s location and speed. He radi-
oed the first mate and instructed him to
immediately inform the deckhands
to prepare
the gangway for evacuation. The master said
that, as he continued up the stairs to the pilot-
house, he observed that the
Bright Field
was
heading directly toward the Poydras Street
wharf. He said he radioed the mate to begin the
emergency announcements over the loudspeak-
ers. According to representatives of the vessel’s
owners, the first mate initiated the first emer-
gency evacuation announcements at 1410:48.
The master, entering the pilothouse at the end of
the first emergency announcements, rang the
general alarm bell at 1411:22. The first mate
made several more emergency evacuation
announcements, after which the master in-
structed him to radio security and have them call
911. The master then told the mate to instruct
the chief engineer to prepare the engines for
getting underway, after which the chief engineer
started the engines.
The ship’s director of security and
surveillance said that he was on the second deck
when he heard the announcement instructing the
passengers to leave the vessel by the gangway.
While moving toward the bow of the vessel, he
began instructing gaming personnel to leave the
vessel after the passengers. He said that at the
bow of the second deck, he was blocked by a
crowd of passengers trying to evacuate over the
gangway. He said he looked out toward the
wharf and saw the
Bright Field
headed toward
his vessel. He said he immediately went out a
side door, then went around the crowd and
began to distribute life jackets and help the
passengers off the vessel. He stated that it was
not normally his responsibility during an
emergency to distribute the life jackets;
however, most of the team leaders, who were
responsible for distributing life jackets, were
assisting passengers in exiting the gangway or
were caught behind the crowd trying to evacuate
the vessel. In addition, the team leaders were
having difficulty reaching the life jackets at the
gangway because of the crowd. During
emergency drills, the passengers were usually
divided into different “refuge areas” and were
not all in the gangway area at the same time.
A nonoperating crewmember recalled
hearing the announcement to evacuate. As she
and the passengers evacuated from all three
decks, they merged together on the second deck,
where the gangway was located. She said that
she did not hear any announcements regarding
life jackets. The master said that he had not
made such an announcement because the vessel
was not scheduled to cruise that day. The
employee said that she saw the deckhands
obtaining life jackets, but that many passengers
were not wearing them because they were
running, and the deckhands were telling them to
keep moving. The crewmember said she did
recall hearing a horn blowing a few times, but
she said she heard this all the time on the river.
She recalled that “everyone was in a panic”
because they did not know what was going on
until they went outside and saw the
Bright Field
heading toward their vessel.

28
Figure 12 -- New Orleans Paddlewheels, Inc., gaming
vessel
Queen of New Orleans
$
*
)
(
'
%
&
3LORWKRXVH
%ULGJH#'HFN
7H[DV#'HFN
+XUULF DQH#'HFN
%RLOHU#'HFN
0DLQ#'HFN
*DQJ ZD\#/RFDWLRQ
+ROG#'HFN
*
)
(
'
%
&
$

29
Another employee, who was on the stern of
the second deck, recalled hearing the evacuation
announcement, after which he began instructing
passengers to proceed to the gangway. As he
began moving forward, he said he heard the
whistle from the
Bright Field
.
He recalled
helping one wheelchair-bound passenger out of
the casino area, over the gangway, and to the
elevators of the hotel. He said he then returned
to help clear the casino floor of passengers and
moved to the bow of the vessel, where he began
distributing life jackets to passengers and
assisting those passengers who were panicking.
The only means of egress from the
Queen of
New Orleans
during the evacuation was a single
gangway from the second deck to a stairway and
elevator structure of the Hilton Hotel and the
wharf. When the
Bright Field
struck the wharf,
the vessel’s bow wave caused the
Queen of New
Orleans
to rise 4 to 6 feet. A deckhand called
the pilothouse and informed the first mate that
the gangway was “bouncing,” or rising up and
down, approximately 2 feet. According to
testimony of the master, the gangway plates
were “jumping” up and down for about 10
seconds. The master instructed the first mate,
who ordered the deckhands to stop the
evacuation. After about 10 to 15 seconds of
“bouncing,” the gangway stabilized again. The
evacuation resumed until the gangway again
began to bounce. The master again instructed
the deckhands to stop the evacuation, raise the
gangway, and report to their mooring stations.
Upon hearing this announcement, the
security director, who said he was not sure what
a mooring station was, assumed the instructions
were for the operating crew. He said he and a
few other crewmembers instructed the
passengers to “get back” and “run to the back of
the boat.” When the crowd became aware that
the
Bright Field
was heading toward the
Queen
of New Orleans
, people began to run toward the
stern of the vessel.
Following this call, the first mate went to
the bow of the second deck to assist the crew,
who had not yet raised the gangway because it
had “restabilized again.” Crewmembers
continued the evacuation from the gangway at
this time. The mate observed a steady flow of
passengers evacuating the gangway, which
again began “bouncing.” At this point, the
gangway was rising approximately 1 to 2 feet
above its normal position. The mate stopped the
evacuation again by stepping in front of the
passengers and physically blocking their path
from the vessel. After several seconds the
gangway again settled, and the evacuation
resumed. At this point, the
Bright Field
had
stopped moving down the wharf, coming to rest
about 70 feet from the bow of the
Queen of New
Orleans
. According to the master, between 70
and 80 percent of the passengers had been
evacuated. According to New Orleans
Paddlewheels, security videotapes from the
Queen of New Orleans
showed that about 90
percent of the passengers had been evacuated
when the
Bright Field
stopped moving, about 70
feet from the bow of the
Queen of New Orleans
.
Once all the passengers had left the vessel,
the master instructed several deckhands to go to
the dock and assist in crowd control and
emergency response. Vessel security instructed
the remaining gaming personnel to exit the
vessel, and only operating crew remained
onboard. At the same time, the first mate
instructed some deckhands to prepare the
lifeboats to launch. Deckhands were also
instructed to conduct a search of the vessel to
verify that all the passengers had been
evacuated. Another deckhand was instructed to
search the river for any signs of a person
overboard. Three gaming and security personnel
were sent to the front of the hotel to direct the
emergency responders.
Meanwhile, the master radioed the 24-hour
medic and sent him to the dock to provide
medical assistance to the injured. A medic,
contracted from a local ambulance service, was
aboard the
Queen of New Orleans
at all times to
provide medical assistance to passengers and
crew. The master called 911, and then instructed
the first mate to send several deckhands to the
Creole Queen
to offer assistance.
Questionnaires were sent to 74 persons who
had been either in or near the Riverwalk
Marketplace when the accident occurred or who
were among the passengers and crew of the
Queen of New Orleans
or
Creole Queen
at the
time of the allision.
34
A total of 12 responses
34
Injury reports were the only available sources for
identifying individuals who may have been on board the

30
were received from individuals who said they
had been aboard the
Queen of New Orleans
when the
Bright Field
struck the wharf. All of
them said they had boarded the vessel between
1300 and 1400. Nine of the passengers did not
recall receiving any information concerning
what to do in the event of an emergency and did
not recall observing any safety information
placards when they boarded the vessel. Seven of
these passengers did not receive a life jacket
when evacuating the vessel. Each of these
passengers recalled first learning about the
emergency when they heard the announcement
from the first mate over the public address
system.
Almost all of the injuries (generally limited
to fractures, abrasions, contusions, lacerations,
and back or cervical strains) occurred when the
passengers were pushed, shoved, or trampled
during the evacuation. One passenger recalled
that the crowd was “out of control, stampeding
like wild animals, pushing, shoving, and
screaming.” Another passenger said she saw
people running and yelling, trying to get out by
the stairwell. “I even saw one man take off
running and jump, trying to walk on people’s
shoulders to get out,” she said. She said that
“getting to or out of an exit to land was
impossible,” and that she was not aware of an
alternate escape route from the vessel.
Another passenger believed she would never
be able to get to the dock and decided to move
to the stern of the vessel and “pray for the best.”
As she began to move aft on the starboard side
of the vessel, she said, she heard a man on the
dock yelling for her to jump. She replied that
she could not jump; however, when she turned
and saw the
Bright Field
still heading in the
direction of her ship, she climbed over the rail
and jumped to the wharf. She sustained pelvic
and lower back fractures and was hospitalized
for 6 days.
Queen of New Orleans
or the
Creole Queen
at the time of
the accident or who may have been inside or near the
Riverwalk Marketplace when the
Bright Field
struck.
Crewmembers of the two ships were identified through
company documents. Other than crewmembers, the only
individuals who received Safety Board questionnaires were
those who had reported being injured during or subsequent
to the accident sequence.
Several passengers commented that the
vessel crew also seemed to panic and did not
appear to be trained for an emergency of this
type. One passenger said she observed some of
the crew running to get off the vessel along with
the passengers. She said she perceived that there
was “no order and no one seemed in charge”
during the evacuation.
According to New Orleans Paddlewheels,
Inc., the comments of these passengers do not
correspond to the surveillance videotape
showing the evacuation. Company officials said
the passengers may have seen some
crewmembers leaving the vessel during the
evacuation, along with the passengers; however,
these were the crewmembers who were not
assigned to assist in the evacuation. The
company said crewmembers with evacuation
responsibilities remained aboard the
Queen of
New Orleans
and provided assistance
throughout the evacuation. The company said
that its security videotape “clearly shows
passengers responding to announcements
immediately, orderly, and no one running.” The
Safety Board has reviewed the tape and did not
observe, in the locations of the vessel shown,
any of the passengers falling or being
“trampled” or knocked down. The videotapes
appear to show passengers exiting the vessel in
an orderly manner without apparent panic.
Creole Queen
-- The master of the
Creole
Queen
was monitoring two handheld radios, a
company radio with two channels and another
radio tuned to VHF channel 67. The main radio
in the wheelhouse also monitored channel 67.
The master stated that, at approximately 1400,
he instructed the deckhands to remove the lines
for the vessel’s second cruise. As the deckhands
let go of the lines and the master began using
the bow thruster to move the vessel away from
the dock, he heard the call from the
Bright Field
pilot to the Governor Nicholls Light operator.
As the master began to maneuver the vessel
back to the dock, he radioed his first mate and
instructed him to go starboard on the main deck,
look upriver, and report his observations. The
first mate reported back, “he’s headed straight
for the Riverwalk.” The master instructed the
first mate to “put the gangway down and begin
an evacuation.”

31
The first mate and a deckhand had gone to
the gate on the deck of the
Creole Queen
to
open it for the gangway. The first mate climbed
ashore and began to lower the gangway while
other deckhands tied up the vessel. Once the
vessel was secure, the gangway was positioned
for the passengers to begin evacuating. The first
mate said he positioned himself on the dock side
of the gangway as the deckhands, on the vessel
side of the gangway, helped the passengers
evacuate.
At this time, the master began making
emergency evacuation announcements to the
passengers. He recalled announcing,
Ladies and gentlemen, this is the
captain. Please exit the boat using the
gangway. Please do not panic. Please
exit the boat using the same entrance as
when you boarded. This is an
emergency. Please exit immediately.
The passengers began evacuating, and the
master rang the general alarm bell. Meanwhile,
the master could hear the
Bright Field’
s whistle
getting closer, but his view of the vessel was
obstructed by the
Queen of New Orleans
.
The first mate observed that the
Bright
Field’
s bow wave caused the
Queen of New
Orleans
to rise up “as if it were out on the ocean
and hit by a wave.” He said he called to the
deckhands to stop the evacuation of the
passengers. The master said he used the public
address system to caution the passengers to
“watch the gangway.” The master estimated that
at that time half of the passengers had evacuated
the
Creole Queen
and were waiting on the dock.
The bow wave and undertow from the
Bright
Field
pulled the
Creole Queen
away from the
dock, and the gangway began to slip aft along
the deck. The deckhands stopped the
evacuation; however, three passengers were still
on the gangway at the time. As the boat rose up,
it “was sucked out” away from the wharf, and
the gangway dropped off the
Creole Queen
and
down toward the water. The three passengers on
the gangway fell into the river between the ship
and the wharf.
The deckhand and some passengers who
were on the dock began to crank up and
reposition the gangway so that the evacuation
could be continued. Meanwhile, a passenger on
the main deck threw a life buoy and a child-size
life jacket to the three passengers in the water.
The first mate, from the dock, told the passenger
where to find an adult life jacket, and the
passenger then threw an adult jacket into the
water. The first mate then instructed a
crewmember on board to retrieve the ladder
from the rescue boat on board and to place it
over the side of the
Creole Queen
. Two of the
passengers in the water climbed the ladder and
entered the vessel. The third passenger, a 61-
year-old man, suffered a hip injury when he fell
into the water, and he was unable to climb over
the railing and into the vessel. The first mate
climbed onto the vessel from the dock and
assisted the crewmember in easing the passenger
into a Stokes Basket. They then pushed the
basket from the vessel over to the dock. While
this was underway, the master was attempting to
reposition the vessel to the fallen gangway. As
he was maneuvering the vessel, he continued to
make emergency announcements to the
passengers until the gangway was re-positioned
and the evacuation could be resumed.
Once the evacuation was complete, the
master requested, via the company radio to the
Queen of New Orleans
’s first mate, that the 24-
hour medic be dispatched to assist some of the
injured
Creole Queen
passengers. The mate on
the
Queen of New Orleans
told him that the
medic was already assisting the injured from the
Queen of New Orleans
. The master later told the
Safety Board that one of the problems he
encountered during the accident was the length
of time it took for emergency medical
technicians to arrive on scene. He recalled that
after he made this complaint to another person
after the accident, he was informed that the
delay in ambulances responding to the dock
where the
Creole Queen
was moored was due to
damage done by the
Bright Field
to the normal
emergency response access route to the wharf.
Three respondents to the Safety Board
questionnaire were individuals who said they
had been on the
Creole Queen
at the time of the
accident.
35
One passenger recalled boarding the
35
Questionnaires were sent only to the three
Creole
Queen
passengers who had reported being injured in the
accident. All three individuals responded.

32
vessel at 1310 and receiving information
concerning emergency procedures. He stated
that, about 1315, the first mate announced that,
if the passengers were required to immediately
evacuate the vessel, they should follow the
instructions announced over the public address
system. This passenger considered those
instructions of great value because the
evacuation was not a typical situation; it
involved little time to don life preservers, form
groups, or disembark to the pier or lifeboats. He
observed placards posted on the salon and
observation decks that provided emergency
information regarding the location of life jackets
and the procedures for donning them.
A couple, a 61-year-old man and 59-year-
old woman, both sustained injuries when they
fell into the water when the gangway collapsed.
They said they boarded the
Creole Queen
about
1350, and they did not recall receiving any
information about what to do in the event of an
emergency, nor did they observe any placards
that provided this information. The female
passenger recalled the master announcing they
were returning to the dock to disembark, and the
male passenger recalled six to eight repeated
calls for “abandon ship.” They observed people
on the Riverwalk running toward the Spanish
Plaza. The male passenger recalled that
passengers were confused when they heard
“abandon ship”; they were unsure whether to
jump into the water or remain on board, and the
crew was shouting, “get the life preservers,
where are the life preservers?” He recalled that
it seemed “like a continuous shouting match”
while the crew was attempting to find life
jackets and the three passengers remained in the
water.
Riverwalk Marketplace
-- In a letter to the
Safety Board, a couple said they were in a café
on the second level of the marketplace when
they heard the
Bright Field’
s whistles. The
husband got up from the table and went to the
window to see what was happening on the river.
When he had almost reached the window, the
Bright Field
struck the wharf, then broke
through the window of the cafe. Patrons seated
near the window “ran screaming and running
out of the café.” The man and his wife said they
heard a waitress yelling “get out” twice as they
ran to the restaurant doors. They turned around
and watched the ceiling and floor above crash
down and fold over the entire room, as the
Bright Field
continued to crash through the cafe.
They immediately left the area to evacuate the
mall.
As they attempted to go up to another level,
“the only route out of the mall [away from the
direction of the river],” they ran into a
“bottleneck,” a large crowd attempting to use
the escalators to reach the higher floors to
evacuate. As they were climbing up the “down”
escalator, they said, they feared a gas explosion
because they smelled gas. When they made it up
to another mall level, many mall customers on
the upper floors were still shopping, unaware of
the accident. At this time, the couple noticed
that they had not yet heard any alarms or public
address announcements, even though it had been
several minutes since the vessel struck the cafe.
They encountered security guards who did not
allow them to use emergency exits to evacuate.
They said they believed they were “strictly on
our own. The mall management apparently had
made no disaster plans for its merchants and
customers; if such plans existed, they were a
complete failure.”
The Safety Board received responses from
15 individuals who said they were either patrons
or employees of the Riverwalk Marketplace
when the accident occurred. One patron recalled
that she was on the first level of the Riverwalk
Marketplace, alongside the wharf, when she
heard the
Bright Field’
s whistle sounding. She
believed that the noise was “normal river noise”
and did not take notice. She then heard people
begin screaming “run,” and “get out.” She said
she turned around and saw the
Bright Field
coming into the wharf area. She said that, when
she turned to run out of the store, she was
knocked down by the crowd. She tried several
times to get up, and was repeatedly knocked
down. After the wharf was struck, a security
guard came to assist her, and he helped her out
of the store and over to a triage area. She was
taken to the hospital and admitted for blunt
abdominal trauma.
A family was shopping in a mall grocery
store at the time of the accident. They said they
heard the
Bright Field’
s whistles but did not
know the whistles were a warning signal. They
thought that a vessel was arriving, so they went
to the glass window on the wharf to watch the

33
Bright Field
approaching the dock. They said
they did not know that they were in danger until
they realized the vessel was not docking but was
actually striking the wharf. They said the store
clerk did not appear to be aware of what the
ship’s warning whistles meant and did not know
that the store should be evacuated.
As the vessel struck the wharf, the family
turned to flee the store. As the customers were
running, the store was collapsing behind them
and the roof began falling in. As the collapsing
walls shifted furniture, the doorway became
blocked, and they could not escape until the
falling ceiling shattered the front glass display
window. When they attempted to leave the mall,
by going up to the third floor, they could not go
up the escalators because there were too many
people exiting the same way. One of the family
members hit the stop button on the “down”
escalator, and they went up to the third floor via
that escalator. They said that when they left the
front of the Riverwalk Marketplace, they were
not given instructions on which way to evacuate.
Not until they were leaving the marketplace did
they see a police officer, and they did not
observe any other emergency responders.
Overall, the family recalled that there appeared
to be a lack of preparedness for an emergency
evacuation and that crowding was a problem in
finding an exit away from the damaged wharf.
Another couple was in a restaurant on the
wharf when they saw other people screaming
and running out of the mall. They did not hear
an emergency whistle from the
Bright Field
or
general mall emergency announcements; they
did hear a fire alarm ringing after the
Bright
Field
struck the mall shops. The couple were
injured when they were knocked down and
“trampled” by shoppers who were fleeing the
mall. The couple recalled the activities of the
mall personnel relating to visitor safety as
“poor,” both during and after the accident. They
recalled that the police and Coast Guard arrived
immediately, and that the fire department
arrived about 10 minutes later.
Riverwalk Marketplace has provided
videotapes to the Safety Board which company
officials say “show the mall being evacuated
within a matter of minutes with virtually no
significant personal injuries suffered by any of
the persons evacuated.” The Safety Board
viewed the tapes, which showed various
locations in the mall during the allision
sequence. The tapes were recorded by security
cameras using a loop system that recorded
frames from all camera locations on a single
tape. Continuous footage from a single location
was not available, and the frames from the tape
loop were made at intervals of about 4 seconds.
These videotapes do not appear to show patrons
being “trampled” or knocked down during the
evacuation.
In addition to providing videotapes to the
Safety Board, Riverwalk Marketplace also has
stated that public safety officers did block
certain emergency exits in accordance with
protocol and the evacuation plans and
procedures. “To allow individuals to exit freely
from any exit they chose might have placed
them in greater peril,” the company said. As for
the smell of gas reported by the patrons, the
company said that a member of the Marketplace
engineering department was on the wharf just
prior to the accident, saw that the allision was
inevitable, and immediately shut off all utility
service to the mall, including natural gas, to
prevent an explosion. The company said that
fire alarms did not sound prior to the allision
because of the absence of any alert or warning
prior to impact. The security central monitoring
station printouts showed the fire alarms
sounding at 1411:42 and 1414:11.
Hilton Riverside Hotel
-- When the
Bright
Field
struck the Hilton Riverside Hotel, the
public safety dispatcher received several 52 F
(fire) activation alarms, and housekeeping
called to inform the dispatcher that a vessel had
struck the riverside hotel. The dispatcher
notified the local fire and police agencies and
called the Director and Assistant Director of
Public Safety and Security. The hotel
Emergency Disaster Procedures Plan was put
into effect and the hotel emergency response
team was notified. The security supervisor on
duty received a call that a possible fire
emergency had occurred in the riverboat casino;
when he arrived in the hotel lobby, he
“discovered that a panic crowd was running
away from the area.” He instructed officers to
calm the crowd down and clear the lobby. He
attempted to use the radio to communicate with
other officers, but when the vessel struck the

34
building, it knocked out the power and,
therefore, communication capabilities. So he
instructed the officers in the lobby to assist him
in evacuating guests from the riverside building.
Meanwhile, a security officer who was
returning to his post from lunch was in the
Riverwalk parking lot when he was met by a
large crowd that informed him that a freighter
had hit the Riverwalk and many people by the
stairs in the rear lot were injured. He ran to the
location and observed people “falling down the
stairs and bleeding.” He attempted to stop the
people from running but to no avail. He found a
person with a cellular phone and called 911 to
report the emergency. He then assisted the
injured until the emergency medical services
arrived. He was then assigned to assist with
traffic control.
Another security officer, who was in front
of the hotel, heard a call from another officer
that a possible fire emergency had occurred on
the riverboat casino. He ran, along with other
officers, to the area and observed that a large
ship with heavy damage to the front section was
“docked” near the casino riverboat and that a
section of the Riverwalk mall and the hotel had
collapsed. They attempted to radio the security
supervisor on duty, but all communications had
been lost due to a power failure in the riverside
hotel building. So, the officers proceeded to the
damaged area of the hotel to evacuate everyone
from the building. They encountered the
emergency response team on the fifth floor as
they were responding to a report of a trapped
female guest.
This emergency response team consisted of
the security, maintenance, and engineering
departments. When the
Bright Field
struck the
hotel, the maintenance person on duty was
headed to the first floor when the building began
to shake violently. The engineering supervisor
was in the carpenter shop when he was notified
by the dispatcher that a vessel had struck the
building. He, the housekeeping supervisor, and
the maintenance person on duty, along with
hotel security officers, conducted a floor-by-
floor search of the hotel. A housekeeper
informed them that a female guest was trapped
in her room. They attempted to open the front
door to the room; however, it was blocked by
collapsed ceiling damage from the freighter’s
allision. They had to use a claw hammer to
break in the hallway wall to reach the guest. The
team was able to open a large hole in the wall of
the fifth floor, and the trapped guest was
evacuated from her room by 1425. According to
the emergency response team, the guest stated
that “there was no one else in room 5085 and
that she did not think that she was injured.”
Meanwhile, other members of the emergency
response team completed the evacuation search
by 1418, when the New Orleans Fire and Police
Departments arrived at the hotel. Another
intensive search of the hotel was conducted by
separate groups of local response agencies and
the hotel emergency response team.
At 1435, the Director of Security arrived at
the hotel, and set up a command post with the
fire, police, and harbor police inside of Kabby’s
restaurant. A printout of the occupied guest
suites was delivered, and all departments
verified the number and locations of their
employees. Once this information was collected,
a third search of the building was conducted. No
other guests were found trapped in their rooms.
According to Hilton Riverside Hotel, no
employees of the hotel were injured during the
Bright Field
allision. The riverside building was
completely evacuated. The engineering
department had notified the security director
that the team secured all utility lines, including
gas and electrical lines, and placed the building
on the back-up generator; power and
communications were restored once this
generator was hooked up to the repeater.
Emergency Response
Port of New Orleans Harbor Police
--
Harbor police officers were the first responders
on scene. They initiated rescue efforts
immediately, ordered emergency units, and
broadcast a description of the incident via police
radio. The harbor police were responsible for
immediate scene stabilization, traffic control,
pedestrian control, and support for the New
Orleans Fire Department. A triage center was
established at a Riverwalk Marketplace security
post, and emergency medical services units were
staged near the rear apron roadway. The
Medical Center of Louisiana’s Charity and
University campuses were notified of the
incident and designated as the primary treatment
facilities. The director of public safety and

35
security for the Port of New Orleans authorized
the request for additional enforcement and
rescue assistance from several surrounding
parish police and sheriff’s departments and from
the Louisiana State police. For the first 48 hours
after the accident, all available harbor police
officers and six recruits were called in to
provide security in both interior and perimeter
areas of the Poydras, Julia, and Canal Street
wharf area.
Coast Guard Group New Orleans
-- The
on-duty officer at Coast Guard MSO New
Orleans was notified of the accident at 1420 by
the Gretna traffic light operator. The initial
report indicated possible persons in the water
and significant damage to the
Bright Field
and
Poydras Street wharf buildings, resulting in
other casualties. At 1421, the MSO on-duty
officer designated Coast Guard Group New
Orleans as the search and rescue mission
coordinator. Group New Orleans requested an
immediate search and rescue response
detachment from Coast Guard Station New
Orleans to search for possible persons in the
water.
At 1422, the Mississippi River was closed at
mile 96 AHP in the vicinity of the accident. At
1430, a Coast Guard helicopter was dispatched
by the search and rescue coordinator to pick up
a rescue swimmer and report to the scene of the
accident. The MSO on-duty officer notified both
the captain of the port (COTP) and the chief of
port operations of the accident. At 1435, the
MSO notified the office of the commander of
the Eighth Coast Guard District.
The MSO chief of port operations
immediately went to the scene. After consulting
with the incident commander, he assessed the
damage and began searching for leaking fuel or
other dangerous conditions. He observed that
the ship was not secured to the wharf, and he
directed crewmembers and firefighters to attach
bow mooring lines.
At 1445, the MSO emergency response
team arrived and boarded the vessel, and the
Coast Guard on-duty officer also dispatched fire
and hazardous materials teams to the scene. At
1447, the helicopter was on scene and searching
the river for persons in the water. At 1550, two
Coast Guard infrared search teams were
dispatched to help search for persons in the
debris of the collapsed Poydras Street wharf. At
1750, the Coast Guard received an update that
no fatalities had been confirmed and that 100
injuries had been reported. All search and
rescue activities were terminated at 1000 on
December 16, 1996.
Louisiana Office of Emergency
Preparedness
-- About 1500, the Louisiana
Office of Emergency Preparedness responded to
the
Bright Field
accident, dispatching the
assistant director and the chief of operations to
the scene to offer State support and assistance.
At approximately 1630, a request was made for
light sets for possible night operations. The
Louisiana Army National Guard provided lights
later that evening.
Police Departments
-- The New Orleans
Police Department assisted the harbor police in
stabilizing the scene, controlling traffic and
pedestrians, and supporting the New Orleans
Fire Department in this accident. The initial call
was received at 1414 to assist the Harbor Police
Department with “unknown trouble...large
crowd of people running inside...possible
building cave in.”
New Orleans Fire Department
-- The
initial call to the fire department dispatcher was
received at 1413. The initial response was a
first-alarm response. When the incident
escalated into a three-alarm response, more than
40 units and 110 people responded. The fire
department established an incident command
system to oversee operations, evacuate the
affected areas, remove the injured persons,
triage and treat the injured, search for and
rescue trapped persons, control natural gas leaks
and utilities, and make arrangements for
perimeter security through the New Orleans
Police Department, the Coast Guard, and the
Port of New Orleans Harbor Police.
New Orleans Department of Health and
Emergency Medical Services
-- The New
Orleans Health Department, Emergency
Medical Services Division, assessed injuries,
treated and transported the injured to local
hospitals, and coordinated additional treatment
and transportation with area private providers.
The initial call was received at 1414 by the
Levee Board police dispatcher, and the first

36
emergency medical services responder arrived
on scene at 1417.
Emergency Preparedness
Riverwalk Marketplace
-- According to
Riverwalk Marketplace figures, approximately
13,500 persons visit the mall daily. The
Riverwalk Marketplace had a mall
emergency/catastrophe plan in place that
included emergency procedures and maps
indicating the locations of sprinkler systems and
zones, fire extinguishers and standpipes, smoke
detectors, chemical and hazardous materials
storage, main entrance feeders and disconnects,
gas shutdowns, water mains, and primary and
secondary emergency exits. Each emergency
exit from the Riverwalk Marketplace was
marked by a lighted sign with the words
“Emergency Exit” in white letters on a red
background.
The emergency procedures instructed mall
employees to first call the local fire department
in the event of an emergency, and then follow
up with calls to the management office. A
command post, if necessary, was to be
designated, and the emergency manager was to
determine, along with fire department officials,
whether to evacuate the mall.
The “Emergency Organization Guidelines”
in the
Mall Security Plan
manual listed
procedures for security officers on duty at the
time of an emergency. This manual provided a
separate emergency evacuation plan for each
level of the marketplace and specified duties and
responsibilities for security officers, dispatchers,
and public safety supervisors during an
emergency evacuation.
In documents provided to the Safety Board
on November 13, 1997, the Riverwalk
Marketplace stated that the Riverwalk policy
“is, and always has been,” that the senior
manager on duty at the time of any event is
responsible for determining whether to evacuate
the mall, or certain portions of the mall. In the
absence of the management, the senior security
supervisor on duty has the authority to call for
an evacuation of all or part of the mall,
depending on the circumstances. The decision to
evacuate is based upon an evaluation of the
safety threat posed to patrons and employees in
the mall. The company said that, once the
decision to evacuate is made, evacuation is
commenced prior to the arrival of firefighters or
police on the scene. Notification of the fire or
police departments, as necessary, is made
instantaneously and coincidentally with the
decision to evacuate the mall.
The company said that, for an emergency
involving a vessel striking the wharf, specific
emergency instructions were based on the
severity of the allision. Immediate procedures
were to contact the harbor police, identify the
damage to the wharf as major or minor,
immediately report the accident to a supervisor,
determine if city services were needed, and
begin safety measures.
New Orleans Hilton Riverside Hotel
-- The
employee manual of the New Orleans Hilton
Riverside Hotel details the procedures to be
followed during a fire or other emergency.
Included in the manual are the duties and
responsibilities of the hotel emergency response
team; the hotel management; the security
department; and the engineering, front desk,
bellstaff, catering, and housekeeping personnel.
The emergency directions include
notification of the fire department,
establishment of a command center, detailing of
evacuation procedures, and notification of
Hilton Hotel headquarters management. Sample
emergency announcement messages are
provided, as are crisis communication
guidelines for on-duty management personnel.
The decision whether to evacuate the hotel
is to be made by the senior manager on duty
prior to the arrival of fire or police officials. The
decision is to be based on the threat of injury to
hotel guests and employees, the extent of the
emergency, and the need to remain in control of
the evacuation while fire or police officials
assess the emergency. The New Orleans Hilton
Riverside Hotel did not have a section in the
emergency procedures or evacuation plan
manual that covered a vessel striking the wharf.
Queen of New Orleans
-- The
Queen of
New Orleans
Emergency Evacuation
Procedures in Moored Conditions
manual
provided instructions for evacuation routes,
including alternates, in the event of an

37
emergency. Each deck had a different escape
route for a specific number of passengers, based
on the number of persons permitted on that deck
and the space available for the exits. All primary
and alternate deck exit routes led to the
gangway located at the bow of the second deck.
This 12-foot-wide gangway led to a stairway
and elevator structure, then into the New
Orleans Hilton Riverside Hotel, or down to the
wharf. The master stated that the time was
insufficient during the
Bright Field
accident to
use the procedures outlined in the manual.
The
Safety and Vessel Operation Manual
for the
Queen of New Orleans
provided safety
information for the operating crew and other
personnel working on the vessel. It included
details concerning the evacuation of the vessel,
a description of the sounding of the alarm bells,
and an explanation of each alarm. It also
described the responsibilities of each
crewmember and specified the refuge area,
muster area, and designated team leader for each
position. According to the manual, the
nonoperating crew were responsible for
mustering passengers, warning passengers,
directing them to refuge areas, assisting them
with life jackets, keeping order in the stairways
and passageways, and generally controlling the
movement of passengers and maintaining their
safety.
Safety Briefings
-- Based on company
documents and the master’s statements, the
Queen of New Orleans
broadcast a vessel safety
videotape on two 27-inch television monitors in
the Hilton Hotel lobby and on one 27-inch
monitor on the boarding structure ramp. The
monitors in the hotel lobby were positioned just
below the ceiling on the wall adjoining the wall
through which a door led to the boarding ramp.
The monitor screens were visible to persons
passing through the door to the ramp if they
looked up and to the right. The boarding ramp
monitor was centered overhead at a point about
halfway up the ramp. The safety videotape
played continuously on the monitors and
demonstrated the donning of a life jacket and
the dangers of the river.
Before each cruise, a safety announcement
informed the passengers of the appearance and
locations of the boxes containing life jackets.
According to the master, an oral announcement
about life jackets was not made prior to the
Bright Field
accident because the vessel was not
scheduled to leave the dock. He stated that the
vessel is “an extension of the dock when we’re
not underway.”
In responding to Safety Board
questionnaires, a number of passengers on board
the
Queen of New Orleans
on the day of the
accident, some of whom had been on the vessel
several times before, did not recall ever having
noticed the video monitors.
Signage
-- The
Queen of New Orleans
had
emergency, safety, and life jacket signs posted
in various locations throughout the vessel.
According to the master’s testimony, the vessel
had overhead signage, including lighted
overhead exit signs at every exit door, directing
passengers to the exits of the vessel. The master
stated that he did not recall any signage near the
floor at designated exits that provided exit
instructions. He said signs were posted
throughout the vessel advising passengers which
level they were on and how to get to other
levels.
The information placards were covered with
thin, clear laminate and attached to the light-
colored bulkheads. An emergency evacuation
placard and casino station bill were posted on
the first and second decks, and three station bills
and an emergency evacuation placard were
posted on the hold deck. Life jacket placards
were found on the inside of the cover of all life
jacket boxes. The placards displayed
instructions for donning life jackets, along with
a photo displaying a properly donned life jacket.
An emergency evacuation placard and station
bill were posted on the fourth deck; a station bill
and emergency evacuation placards were posted
on the third deck. According to 46 CFR 199.80
(8)(c), vessel emergency instructions “must be
posted in each passenger cabin and in spaces
occupied by persons other than crew, and must
be conspicuously displayed at each muster
station.”
Emergency Egress
-- The
Safety and Vessel
Operation Manual
described both “dry” and
“wet” evacuations. The wet evacuation involved
putting passengers into the water with life
jackets and other emergency equipment. Dry
evacuations involved assisting passengers to

38
embarkation areas where they would disembark
via an emergency evacuation ramp/slide. The
location of this ramp/slide was not shown on the
vessel diagram in the manual, and no other
reference to the equipment was made.
According to company documents, at the time
the vessel was under construction, the owners
experimented with the slide, but they were not
satisfied with its safety and performance;
therefore, the slide was not incorporated into the
vessel design. According to the company, three
portable emergency gangways were maintained
aboard the vessel at all times and were designed
to be used in the event the main gangway
became inoperable.
Drills
-- According to the company, fire drills
for the
Queen of New Orleans
operating
crewmembers were held twice per week, one per
crew, with active participation mandatory. At
least weekly, each marine crew participated in
rescue boat drills in which the rescue boat davit
and motor were tested and the boat was lowered
into the water. To facilitate documentation and
management of the drills, a safety team leader
was designated for each area of the vessel. The
safety team leader assisted the master with
coordination and control of the drills. First aid
and CPR training were required for all security
supervisors, mates, masters, engineers, and lead
deckhands.
According to the master, the deckhands
participated in fire and emergency drills, and the
evacuation drills were incorporated into the
safety and security meetings. Detailed minutes
of the safety meetings were not kept, although a
brief description was included on special safety
and fire drill forms. During these meetings,
deckhands were instructed in the handling of the
flow of passengers through the vessel during an
emergency. The master stated that the
passengers “have to get out of the casino
themselves or walk out themselves, and then we
can direct them to the exit of the vessel.”
Security crew were instructed to assist in the
evacuation procedures as well. The master said
that passengers were not involved in the weekly
drills, so the crew had not practiced physically
moving passengers.
According to the master, the gaming staff
did not take part in the regularly scheduled
evacuation training. Instead, the safety team
leaders participated in the drills. Two safety
team leaders were assigned on each level of the
casino except on the fourth and first levels,
where there were few passengers and where one
team leader was assigned. The security staff was
involved with the safety meetings, as were
supervisory gaming employees. These
supervisors were instructed to inform the
remaining gaming staff about the content of the
meetings. According to the master, no formal
procedure existed for verifying that this
information was being relayed to gaming
employees. The master said he had randomly
checked gaming employees to verify that they
knew of the nearest safety equipment, knew
which exits to use, and knew how to don a life
jacket.
Creole Queen
-- The
Creole Queen
operations manual covered emergency
evacuations, emergency egress, and firefighting
procedures. The station bill section of the
manual required that a life jacket demonstration
be given before each cruise. The station bill also
included instructions regarding the sounding of
the vessel’s whistle and ringing of the general
alarm for emergency situations such as fire,
abandon ship, man overboard, and dismissal
from drills. The station bill also included a
description of the duties and responsibilities of
each crewmember during each of these
emergencies.
Inspections, Tests, and Research
Several days after the accident, Safety
Board investigators boarded a fully loaded
vessel that was similar to the
Bright Field
in
size, displacement, and power. During a transit
downriver in high water conditions similar to
those on the day of the accident, the pilot did
not use full speed to maneuver the ship.
Safety Board investigators boarded the
Bright Field
shortly after the accident to
examine shipboard systems. Because the
Bright
Field
was still alongside the damaged wharf at
this time and could not be moved, its direct-
drive engine could not be started during initial
tests and inspections. After conducting a general
survey of the engineering plant, Safety Board
investigators focused their efforts on the
engineering systems most closely associated
with the ship’s propulsion plant and related

39
control systems. These systems included the
steering gear, the main engine and associated
main engine auxiliary subsystems, the
automated propulsion control system, and the
maintenance and management infrastructure for
the vessel’s engineering plant.
Steering Gear
-- The
Bright Field’
s electro-
hydraulic steering gear consisted of a tiller, two
rams, four cylinders, two electric hydraulic
pumps, and an electro-hydraulic control system.
During the investigation, the steering unit was
inspected externally and was operationally
tested by timing the rudder movements in
accordance with SOLAS ’74 steering
performance standards. The
Bright Field’
s
steering system functioned normally.
Main Engine—General
-- Because the main
engine could not be started and run during initial
inspections, the initial survey of the condition of
the engine was based on visual inspection,
testimony of crewmembers, and review of
maintenance and operating documentation.
Visual inspection of the main engine revealed
nothing unusual. The second engineer stated
that the engine’s exhaust gas temperatures ran
abnormally high and that, as a result, the crew
had had to replace pistons and cylinder liners
several times since July 1996. His maintenance
records confirmed this fact. The repairs to the
air turbocharger and air cooler made during the
vessel’s New Orleans port call were an effort by
the vessel owners to correct the problem. The
engineering crew stated that the main engine
operated normally during the trip downriver on
the day of the accident; however, a review of the
Terasaki alarm printout for the early part of the
voyage indicated that the main engine was
experiencing cylinder jacket water cooling
alarms due to low jacket water cooling pump
pressure. The tape also recorded alarms
indicating main engine lubricating oil purifier
malfunction and high second filter pressure
differential. A more detailed review of
engineering reports, including information
received late in the investigation from civil
litigation depositions, is contained in appendix
B. From at least January 1996, the
Bright
Field’
s main engine experienced continued
problems with component failures.
Main Engine Lubricating Oil Sump
--
According to engineering drawings, the engine’s
normal lubricating oil sump level was 14 cubic
meters (about 3,699 gallons) when oil pumps
and machinery were off. With pumps and all
mechanical equipment running, the oil level in
the sump should drop to about 10.3 cubic meters
(about 2,721 gallons). The design plans
indicated that the low-oil-level alarm should be
set to activate at 8.16 cubic meters (about 2,156
gallons). With both lubricating oil pumps and
other machinery off, the oil level for the
Bright
Field’
s main engine lubricating oil sump was
measured by Safety Board investigators at 10.75
cubic meters (about 2,840 gallons). Safety
Board investigators examined the main engine
sump and found that, with pumps and
mechanical equipment running, the
Bright Field
gauge read 8.1 cubic meters (about 2,140
gallons). Investigators tested the
Bright Field
low-oil-level alarm and found that it activated at
about 7.25 cubic meters (about 1,915 gallons).
The chief engineer’s log book recorded that,
upon the
Bright Field’
s arrival at New Orleans
on November 21, 1996, the main engine oil
sump level was 7.5 cubic meters, with the
engine running. At about the time of the allision
on December 14, 1996, the Terasaki monitoring
system recorded a main engine low sump oil
level alarm.
Main Engine Lubricating Oil
Pumps/Motors
-- According to testimony of the
engineers, both No. 1 and No. 2 (electrically
driven) oil pumps were operating at the time of
the allision, and they had not been altered in any
way since the accident. The No. 1 oil pump was
noisy and exhibited a periodic rumbling sound,
as if the pump were cavitating.
36
Lubricating oil
temperature was approximately 56 °C (about
132 °F). Mean discharge pressure was about 2.8
bar, however, both suction and discharge gauges
were oscillating wildly, making it difficult to
obtain a reliable reading. When pump No. 2 was
stopped, the system pressure dropped to about
2.3 bar. Pump No. 2 was tested and operated
satisfactorily.
36
The pump
cavitates
when numerous vapor bubbles
form in the oil. Subsequent collapsing of the bubbles can
produce a distinctive rumbling sound in a piping system.

40
Investigators opened and examined both oil
pump basket strainers and found them intact and
clear. The No. 1 oil pump was restarted, but it
continued to produce only about 2.3 bar. The
pump was examined for possible suction-side air
leaks, but all flanges, seals, and joints appeared
to be intact. The pump was taken to a marine
engineering repair facility for disassembly,
inspection, and testing. Other than minor wear,
no significant defects were found, and all
clearances were within manufacturer’s
specifications. The pump was reassembled and
reinstalled in the
Bright Field
.
During additional testing witnessed by
Safety Board investigators about 2 weeks later,
the No. 1 oil pump was again examined, started,
and found to be running quietly. Suction
pressure was -0.3 bar, and discharge pressure
was about 4 bar by local gauges. The pump
pressure relief valve was found to be operating
in accordance with the manufacture’s
specifications. The following day, investigators
reexamined the oil pumps and found high noise
levels associated with both pumps, including the
“cavitation-like” sound. No obvious leaks were
found in the flanges and openings on the
suction-side piping, and both pumps generated
rated (4 bar) pressure. Close inspection of the
No. 2 oil pump discharge stop check valve
revealed that the stem was jammed in the valve
yoke, and the valve would not manually close
and seat. The “check” feature of the valve
appeared to function correctly when subjected to
back pressure. Both oil pumps evidenced
noticeable vibration and noise for the remainder
of the vessel’s stay in New Orleans, and the
cause of the abnormal operation could not be
determined with certainty.
Main Engine Lubricating Oil System
Second Filter/Strainer
-- The second
filter/strainer was designed for working pressure
of about 4 bar and a working oil temperature of
45 °C (about 113 °F). The filter was equipped
with two pressure switches. One switch
monitored differential pressure across the filter
and activated an automatic backwash system (to
clean the strainer) if the pressure differential
reached a certain level. The other switch was
designed to activate an alarm in the event of a
differential pressure drop across the filter
greater than 0.9 bar.
On December 17, 1996, Safety Board
investigators recorded second filter/strainer inlet
and outlet pressures of 3.4 and 2.4 bar,
respectively, with the lubricating system still
running in the same condition, including an oil
temperature of 56 °C, as at the time of the
accident. A high-differential-pressure alarm did
not sound. Safety Board investigators
determined that the differential pressure alarm
had been set at 1.3 bar.
Safety Board investigators opened and
examined the second filter and found that the
installation was consistent with design
drawings. No visible debris buildup or blockage
was found. The filter was cleaned, reassembled,
and tested with new oil. The differential
pressure was found to be approximately 0.7 bar.
The filter manufacturer recommends that the
second filter/strainer be opened and cleaned
every 6 months. No record was found in the
second engineer’s maintenance log to indicate
that the filter had been cleaned between late
July and December 1996.
Main Engine Lubricating Oil Purifier
--
The
Bright Field
third engineer told the Safety
Board that the lubricating oil purifier was
supposed to run continuously (whether or not
the engine was running), drawing oil from the
engine oil sump, removing water and sediment
from it by centrifugal action, and then returning
the cleaned oil to the sump. Because the purifier
functioned with warm oil only, an auxiliary
boiler was needed to heat the oil when the
engine was not running. The
Bright Field
chief
engineer, in a December 9, 1996, letter to the
vessel owner, stated that the purifier had not
been used because the auxiliary boiler had been
inoperative. At some point during the vessel’s
stay in New Orleans, and prior to the accident,
the auxiliary boiler was repaired, and the
lubricating oil purifier was restarted.
On January 3, 1997, Safety Board
investigators were present when the oil purifier
was stopped, cleaned, and restarted. On January
6, 1997, the purifier began to alarm due to loss
of water seal. When the purifier was opened and
examined on January 10, 1997, investigators
found heavy contamination from an asphalt-like
substance.

41
Automatic Main Engine Lubricating Oil
Trip Function
-- According to statements from
the chief engineer and other engineering
crewmembers, the normal practice for the
Bright
Field
while operating in restricted waters was to
have the No. 1 lubricating oil pump running and
the No. 2 pump on automatic standby and that
the vessel was operating in this configuration on
the day of the accident. On January 4, 1997,
Safety Board investigators tested the oil pump
automatic changeover feature by reducing the
lubricating oil pressure sensed by the device.
During these tests, the pressure switch failed to
activate the standby pump. While investigators
were conducting tests of other system
components,
Bright Field
engineering
crewmembers examined and further tested the
pressure switch. When Safety Board
investigators retested the pump changeover
feature a few days later, the switch functioned
and started the standby pump automatically. The
original pressure switch was removed from the
vessel for laboratory testing. Test conclusions
were that, “the contact resistance is abnormally
high,” and could, under certain conditions,
“cause a problem; i.e., giving erroneous …or
faulty readings.”
Alarms, Indicators, and Recorders
--
Safety Board investigators examined wheel-
house and control room engineering alarm lights
and found that the wheelhouse automatic slow-
down alarm light was burned out. In tests of the
wheelhouse and control room audible and visual
alarms using the manufacture’s test plan, the
system worked as designed.
The Terasaki monitoring and alarm system
was designed to record and print out alarm
conditions and propulsion control system events
that were activated by the automated system.
Manual actions taken by the operating crew
were displayed on video monitors in the engine
control room, but no printed record was made of
those actions. The alarm log printout for the day
of the accident showed engine trip due to low
oil pressure at 1406. The printout did not
indicate automatic starting of the No. 2
lubricating oil pump.
Investigators compared lubricating oil
pressure readings displayed on local analog
gauges with those recorded by the Terasaki
system. While the analog gauges displayed the
same readings, the monitoring and alarm system
recorded pressures that were higher than the
gauge readings by about 0.3 bar.
Remote Engine Control Tests
-- On
January 5 and 10, 1997, with representatives of
IHI, the
Bright Field
engineering and navigation
crew, and the Coast Guard in attendance, Safety
Board investigators observed testing of the
remote engine control using an IHI simulation
plan dated December 29, 1996. Control was
successfully shifted between the wheelhouse
and the control room, and the control room
answered all telegraph commands from the
wheelhouse. No unexplained anomalies were
noted at either control station. Similar tests were
later conducted with the vessel underway, and
all controls worked as designed. In testimony,
neither the chief engineer nor the chief
electrician could explain the two engine-starting
anomalies experienced by the vessel on
December 14 on the downriver voyage. During
testing, the problem could not be reproduced.
Preventive Maintenance
-- The
Bright
Field
was provided with owners’ instructions,
dated August 28, 1995, that described
requirements for periodic (based on engine
hours) inspection and repair of the vessel’s main
engine, auxiliary, and electrical equipment
(exclusive of equipment associated with the
automated propulsion control system). On
October 25, 1995, the owners, concerned about
“frequent cylinder liner cracks in the past 1 or 2
years,” instituted additional operating policy for
the maintenance of the
Bright Field
main
engine. Safety Board investigators were unable
to find evidence that the vessel’s crew(s)
complied with the periodic maintenance
requirements developed by the owner.
Reports and Recordkeeping
--
Engineering personnel on the
Bright Field
maintained several types of records that were
reviewed by investigators. The second
engineer’s daily log book recorded work done
on the vessel’s machinery. The log was
translated by the second engineer each month
and sent to the owner with other vessel reports.
The owner received periodic telexes from
the master documenting the severity of
engineering problems, delays in scheduling
resulting from the engineering problems, and

42
the inability of the engineering crew to make
permanent repairs. See appendix B for a detailed
chronologies of engineering problems
referenced in the monthly engineering reports
and in the master’s telexes to the
Bright Field’
s
owner.
Main Engine Lubricating Oil Testing and
Analysis
-- The
Bright Field’
s lubricating oils
were supplied by British Petroleum (BP) on
long-term contract. BP also periodically
processed oil samples provided by the owner for
test and analysis.
In a January 20, 1996, analysis of a
Bright
Field
main engine bearing oil sample, BP found
a reduced flash point and recommended
corrective action. Analysis by BP of an August
24, 1996, sample showed increased viscosity
and reduced flash point. BP oil analysts
concluded that the oil was contaminated by fuel
oil leaking from the main engine. The report
recommended immediately replacing the main
engine lubricating oil and correcting the fuel
leak. The second engineer stated that he
changed the main engine lubricating oil on
November 5, 1996, after the main engine
alarmed and went into emergency slowdown
because of a high density of oil mist in the
crankcase. The second engineer stated that he
suspected fuel oil contamination of the
lubricating oil system.
The engine manufacturer recommended to
the
Bright Field’
s owners in November 1996
that the engine oil be tested as soon as possible
to check for contamination by water and fuel.
The sample was drawn by the chief engineer on
November 20, but was not tested by BP until
June 1997. BP analysis of the oil indicated
elevated water content and viscosity compared
with BP’s oil specifications and the engine
designer’s recommended range of acceptable oil
properties. The analysis also recorded elevated
insolubles due to combustion byproducts
entering the lubricating oil.
A December 18, 1996, sample collected by
the
Bright Field’
s chief engineer was tested by
Saybolt, Inc. The analysis indicated excessive
water content and high viscosity when
compared to a clean sample of the BP oil.
Saybolt reported that the oil sample also
contained a significant amount of suspended
particulates. Additional analysis of lubricating
oil samples collected by Safety Board
investigators and analyzed by JET-CARE
International, Inc., confirmed elevated viscosity
and water content in excess of BP and Sulzer
specifications.
Spare Parts and Calibration Tools
-- The
second engineer’s maintenance record and
telexes from the master noted that spare parts
for the main engine, auxiliary boiler, water
maker, and other engineering equipment were
either in short supply, of poor quality, or not
available at all. According to the records, the
lack of readily available spare parts meant that
engineering personnel had to reuse worn or
damaged parts that could be made serviceable.
Calibration tools necessary to set the timing of
the main engine fuel pump were missing and
could not be located.
Sulzer Inspection
-- A representative of
New Sulzer Diesel, the designer of the
propulsion diesel engine, had inspected the
engine shortly after the
Bright Field
arrived at
New Orleans in November 1996. He identified
several sources of possible lubricating oil
contamination and noted the following problems
with the main engine:
•
Cracked cylinder liners;
•
Missing, worn, dirty, carbon-contaminated
components, including piston rings;
•
Clogged cylinder inlet ports and piston
cooling passages;
•
Clogged, dirty, damaged components to
charge air receiver; water leaks observed;
•
Fuel oil pump drain clogged and leaking
fuel oil into main engine lubricating oil
sump (recommended testing oil as soon as
possible);
•
Missing main engine turbocharger filters
and dirty internals;
•
Control air system valves clogged with
condensation;
•
Worn, loose, misaligned fuel oil pumps and
linkages.

43
Chief Engineer’s Assessment
-- On
December 9, 1996, the new chief engineer
corresponded with the
Bright Field’
s owners,
confirming the seriousness of engineering
problems observed by the Sulzer technician in
late November and indicating the status of
repairs. He reported the following:
•
Scavenging box showed serious accumula-
tion of sludge and carbon with blocked air
vents;
•
Charge air cooler separation panels pol-
luted, blocked, and rusted;
•
Scavenging box nonreturn air valves
blocked with sludge;
•
Missing, loose, worn piston rings; spare
piston rings of low quality;
•
High-pressure fuel oil pump residue
discharge pipes blocked, leaking fuel oil
into lubricating oil sump;
•
Cracked, welded cracks in No. 2 cylinder
liner; renewed piston head (only 360 hours
of operation since this cylinder liner was
last pulled);
•
No. 5 piston rings replaced;
•
Control air system contaminated;
•
One Terasaki computer monitor out of
commission; second monitor distorted;
•
Auxiliary boiler out of commission; fuel oil
pump not working and numerous plugged
(with debris) tubes from lack of
maintenance; main engine’s main bearing
lubricating oil not being purified;
•
Abnormal main engine cylinder cooling;
•
Smoke exhaust from main engine dark
because of problems with turbocharger
and/or charge air cooler;
•
Improper main engine fuel oil injection
timing;
•
Serious noise and vibration from both main
engine lubricating oil pumps;
•
Numerous auxiliary pumps, engines, and
motors not working or working poorly.
Safety Board investigators examined the
engineering plant following the accident and
determined that the vessel had sailed on
December 14, 1996, with the following
uncorrected engineering conditions:
•
Severe noise and vibration in both main
engine lubricating oil pumps;
•
Defective Terasaki monitoring equipment;
•
High differential pressure across the second
filter;
•
Poorly calibrated sensors (automated pro-
pulsion control system); and
•
Main engine lubricating oil quality and
quantity that did not meet specifications.
Tests, Reports, and System Calibration
--
The chief electrician’s log book reflected
electrical work completed, tests conducted,
problems encountered, and electrical machinery
(cranes, winches, motors) used each day. The
reports were translated by the chief electrician
and included with the vessel’s monthly reports.
(See appendix B for a record of problems
associated with the automated propulsion
control system.)
The chief electrician also conducted
quarterly testing of engineering safety devices,
such as alarms and sensors, and submitted a
report on their operation to the owner. The
quarterly testing did not evaluate the condition
of engineering safety control devices, such as
the pressure switch for starting the standby
lubricating oil pump. Also excluded were the
trip and slowdown set points. The chief
electrician stated that neither he nor the chief
engineer tested the calibration of the automated
propulsion control system set points.
The
Bright Field
was originally delivered
with a complete DNV-approved set of
automated propulsion control system test
procedures for periodically validating the
operability of the control system. The
Bright
Field’
s engineering crew stated that they were

44
unaware of any test procedures and did not
regularly test or calibrate the system. The
engineering crew could not produce a set of
automation test procedures. Copies of post-
delivery automation test procedures were found
in the crew’s library.
Technical manuals covering each
component of the automated propulsion control
system were on board the
Bright Field
. Most of
the manuals were found in the staterooms of
individual engineering officers.
Computer Simulation
-- The Vehicle
Performance Division of the Safety Board’s
Office of Research and Engineering digitized
and analyzed data retrieved from a video made
by the tugboat
Lockmaster
as the vessel’s radar
tracked the
Bright Field
. Engineers attempted to
compute vessel motion parameters; however, the
radar data were of low resolution and did not
provide an accurate depiction of the
Bright
Field’
s movement. The Safety Board contracted
with the Corps of Engineers to perform an
engineering computer simulation to determine
the path of the
Bright Field
during the accident
sequence. The simulation was based on
computer modeling of the
Bright Field
and the
Mississippi River at the accident site. Because
of the limited number of parameters available
upon which to base the simulation, the Corps of
Engineers simulation results were also
inconclusive.
Other Information
Port Risk Analysis and Management—
Coast Guard
-- The Coast Guard, under the
Ports and Waterways Safety Act of 1972
, was
charged by Congress with monitoring,
managing, and communicating risk in all U.S.
ports and taking actions to maintain risk at an
acceptable level. The act empowers Coast Guard
COTPs to monitor the risk levels in their port
areas and maintain “an acceptable level of risk.”
The Coast Guard
Marine Safety Manual
defines
the elements of waterways risk assessment to be
considered by the COTP as vessel properties,
waterway properties, cargo properties, and
environmental conditions.
General port risk management is the
responsibility of the Coast Guard’s Office of
Marine Safety and Environmental Protection,
which is charged with protecting the public, the
environment, and United States economic
interests by preventing or mitigating the effects
of marine accidents and incidents. According to
the “Program Principles” section of the Office
of Marine Safety and Environmental
Protection’s
1996 Performance Report
,
37
risk
management is the “business” of the office. The
report states:
Preventing low probability-high
consequence events, such as major loss
of life on passenger vessels, and
medium and major oil spills, is a
cornerstone of our risk management
approach. To improve our decision
making, we need to strike a balance,
allowing field commanders to employ
existing risk analysis tools for routine
risk management decisions, while
establishing a formal program policy for
high level risk analysis projects, such as
comprehensive port risk models.
Appendix III of the report, “Risk
Management & Risk Analysis,” defines risk as
“the probability of suffering a degree of harm
from one or more hazards.” The document
quantifies this definition with the formula:
RISK = Probability x Consequence
The document states that the risk equation
implies that some risks are greater than others
and that risk management involves choices
about “how, and to what degree, we will try to
reduce the probability and/or consequences of a
potentially harmful event.” The document states
that a complete risk management process
includes
risk analysis
,
risk management
, and
risk communication
.
Risk analysis
, according to the document, is
the process of systematically identifying,
estimating, and ranking risks according to their
probabilities and consequences. From that
ranking of risk, a risk-ranking matrix (figure 13)
can be developed. The document states that the
37
The 1996 report on the office’s progress toward
goals contained in Commandant Instruction 16000.2
(series),
Business Plan for Marine Safety and
Environmental Protection
.

45
Office of Marine Safety and Environmental
Protection’s overall risk management strategy
using this matrix is to select the higher risks that
can be influenced and try to reduce their
frequency and/or consequence in order to
minimize their contribution to overall risk in the
waterway.
Risk management
, according to the
document, is the systematic selection of options
for treating different risks. “Options may
include measures aimed at reducing the
probability and/or consequences of particular
risks, eliminating risks, shifting risks in space
and/or time, or tolerating risks.”
The document defines
risk communication
as the “continuous, two-way process of
communicating with stakeholders
38
about the
risks associated with [the] system of concern.”
Port Risk Analysis and Management—
Other Stakeholders
--
During the past 20 years,
various stakeholders in the greater New Orleans
port area have commissioned numerous risk
assessment and reduction studies.
38
Stakeholders
refers to parties of interest, from both
public and private sectors, in the Port of New Orleans area.
Lower Mississippi River Safety Study
--
The
objective of this 1981 study by Louisiana State
University was to develop recommendations
concerning the way in which communications,
electronics surveillance, aids to navigation, and
traffic management could best be used to
enhance river safety and protect the
environment. The study identified problems
among port and waterway uses, determined
traffic patterns and volume in the area,
synthesized accident data from the Coast Guard
and other sources, identified areas of hazard
created by natural and artificial conditions and
structures on the river, surveyed those who use
the river to ascertain their opinions about river
safety and what was needed to improve it, and
developed a prototype system to enhance river
safety.
Louisiana World Exposition
-- Prior to the start
of the 1984 world’s fair, LWE officials prepared
an environmental impact statement that
addressed safety concerns associated with
marine accidents. An analysis of vessel
incidents between January 1973 and September
1981 revealed that only one vessel had struck
the Julia Street wharf during that period, with no
injuries reported. The Poydras, Julia, and Erato
Street wharves were determined to be the areas
least associated with vessel strikes.
/RZ
&RQVHTXHQFH
0HGLXP
&RQVHTXHQFH
+LJK
&RQVHTXHQFH
+LJK
3UREDELOLW\
0H GLXP
3UREDELOLW\
/RZ
3UREDELOLW\
Fi
g
ure 1
3
--
C
oast
G
uard risk-rankin
g
0DMRU#3DVVHQJHU
9HVVHO#&DV XDOW\
0DMRU#2LO#6SLOO

46
LWE officials recognized that fair structures
and activities could adversely affect safe
navigation along the Mississippi River. For
example, fair officials were concerned that
nighttime illuminations, including fireworks
displays, could interfere with the night vision of
mariners. To minimize these risks, the LWE
requested that the COTP establish a “safety
zone,” within which the Coast Guard would
regulate marine traffic when the fair held special
events on the river. The safety zone was
established, and mariners received notices from
the Coast Guard cautioning them to navigate
vessels with extreme care in the vicinity of the
world’s fair.
The Dock Board refused to allow the
berthing of barges and houseboats at the Julia,
Erato, and Poydras Street wharves during the
fair. The Dock Board rejected the LWE’s
request to place exhibit pavilions (that would be
expected to have large numbers of visitors) on
floating barges moored along the river.
39
The
Dock Board did permit the mooring of tall ships,
oceangoing passenger vessels, large
sternwheelers, and visiting foreign warships in
the area.
International RiverCenter
-- Prior to the
expansion of the Hilton Hotel, the IRC was
required to obtain construction permits from the
city of New Orleans, the Corps of Engineers,
and the New Orleans Levee Board. The Dock
Board required that the plans be submitted for
review and executed a lease with the IRC for the
development. The Dock Board reviewed the
plans to determine the extent to which the
development might interfere with Dock Board
activities.
According to the IRC, during the time when
the IRC was negotiating a lease with the Dock
Board, the Dock Board advised the IRC that
vessels had had allisions with wharves within
the Port of New Orleans, but that no allisions
had occurred at the Lower Poydras Street wharf.
The IRC representatives were shown
photographs of the allisions at other wharves.
39
Information regarding activities of the Dock Board
during the fair was provided by the Dock Board and
confirmed by a former Dock Board chief executive officer.
These photographs, according to the IRC,
“depicted only minimal damage.”
An IRC official was not aware of any
preconstruction risk assessments that were
carried out in connection with the Hilton Hotel
expansion in the early 1980s, and the IRC was
unable to provide the Safety Board with any
other information regarding previously
completed risk assessments regarding their
properties built on the river side of the levee.
The damaged properties, including portions of
the Riverwalk Marketplace mall, the
condominium parking garage, and the Hilton
Hotel are being rebuilt on the same footprint. No
physical barriers against accidents involving
river traffic have been constructed at this
location.
New Orleans Aquarium of the Americas
--In
1987, before construction of the Aquarium of
the Americas, the Audubon Institute contracted
for a risk analysis for construction of the
aquarium on the riverfront outboard of the
levee. The contractor was asked to assess the
safety risk from marine traffic at the site of the
proposed Riverfront Park, including aquarium
structures and park area. The scope of work
included a study of 20 years of Port of New
Orleans records documenting damage to
waterfront facilities at and near the site of the
proposed Riverfront Park, as well as the
potential consequences of an allision of a vessel,
barge tow, or boat with Port of New Orleans
wharves such as the Bienville Street wharf,
where the proposed aquarium was to be located.
The report concluded that vessels and tows
moving downriver, with the current, have less
water moving across the rudder, rendering them
less maneuverable and their pilots less able to
adjust to emergency situations. This hazard
increases with higher river stages, which deliver
faster currents. The study concluded that, if an
outbound ship or tow were to lose steering,
power, or control, or if it were to become
slightly out of shape to navigate the bend around
Algiers Point, the Bienville Street wharf area
would be less likely to be damaged, since the
downriver current would probably carry the
vessel past this area. Vessel damage would more
likely occur in the areas of the Governor
Nicholls, Esplanade, or Mandeville Street
wharves, which are located in the Algiers Point

47
bend of the river, about 3/4 mile below the
Bienville Street wharf. According to the report,
because Bienville Street wharf is high in the
bend, it faced low risk of being struck by an
outbound vessel.
A Port of New Orleans review of records for
1967 through 1987 indicated that the Bienville
and adjacent Toulouse Street wharves had
received no major vessel strikes; however,
major vessel strikes had occurred along the
wharves at and downriver from Governor
Nicholls Street.
Analysis of wharf damage from ship, barge,
and tow strikes revealed that such damage rarely
penetrated beyond 25 to 50 feet inward of the
fender line. The shock from such an accident
could be felt for a distance along the wharf; but
the impact load was not sufficient to
compromise the overall stability of the wharf.
The report concluded that any major
structure located 100 feet or more from the edge
of the wharf would not be in danger from river
marine traffic. The report recommended that the
area within 50 to 100 feet of the wharf be
considered a buffer zone that, while open to
pedestrian traffic, should be free of building
structures. The report stated that this buffer zone
could be most effectively isolated from the inner
wharf area by a motion control joint, installed
parallel to the fender line, that would reduce any
vibrations from a ship strike.
Gaming Vessel Risks and Background
-- In
1991, the Dock Board initiated a series of
planning initiatives related to riverboat gaming.
These initiatives included commissioning the
Coast Guard and the Louisiana State University
National Ports and Waterways Institute to
conduct a navigation risk assessment. The Dock
Board also contracted with a safety consultant to
review the safety of Dock Board properties and
to develop guidelines for gaming vessel
operation. The consultant’s study addressed
public-safety aspects of riverboat gaming,
focusing on fire protection, police response, and
emergency medical services. It focused
particular attention on ways of ensuring that
gaming vessels had adequate access and egress.
The Coast Guard COTP determined that
about 350 incidents of steering and power loss
were reported annually in the COTP-NOLA
zone.
40
The COTP requested that the Dock
Board provide a navigational risk assessment in
preparation for berthing the riverboat gaming
vessels. The Dock Board contracted with the
National Ports and Waterways Institute, in
cooperation with the George Washington
University, to conduct the risk assessment that
went beyond the scope of the Coast Guard’s
request to consider a wide range of safety
aspects along the Mississippi River. The
assessment incorporated input solicited from
waterway users, including local pilots. The
study did not address the high-capacity
passenger cruise ships that use the Julia or Erato
Street wharves as bases of operations.
Phase I of the study, completed in July
1994, concluded that the addition of gaming
boats to the Mississippi River increased both the
probability of a marine casualty and the
potential impact of such a casualty. While the
increase in the probability of an incident was
comparatively small, the increase in potential
injuries and loss of life was large in relation to
casualties involving nongaming vessels. The
study determined that the increased risk was
primarily a function of the operating
environment, not of the vessels themselves. The
study asserted that restricting the conditions
under which gaming vessels may cruise could
reduce, but could not eliminate, the risk.
Accident data (figure 14) for the Port of
New Orleans from 1983 through 1993 (a total of
166 rammings along the left descending bank
between miles 91 and 101 AHP) were analyzed
and the results tabulated to identify a mooring
area for gaming vessels of “lowest historical
allisions on the left bank.” The study stated, “It
should be noted, however, that no area of the
left bank downbound was completely free of
allisions during the eleven year period.”
The phase I report made the following
recommendations:
•
Gaming vessels moored on the left
descending bank of the Mississippi River
40
The COTP-NOLA zone extends along the
Mississippi River from the Arkansas border to the Gulf of
Mexico.

48
3 8 43 48 53
1 ##$
80%(5 2) //,6,216
0
,/(3267
)
LJ
X
UH
#4
7
#0
0
#
$
OOLV
LR
Q
V
#
LQ
#WK
H
#
0
LV
V
LV
V
LS
S
L#5
LY
H
U#+
WR
WD
O#4
9
9
,#
E
H
WZ
H
H
Q
####
#####
######
#P
LOH
V
#<
4
0
4
3
4
#$
+
3
#+
OH
IW
#G
H
V
F
H
Q
G
LQ
J
#
E
D
Q
N
,#4
<
;
6
0
4
<
<
6
<418
<41<
<514
<6
<615
<619
<61:
<714
<715
<717
<719
<71<
<8
<818
<819
<915
<916
<:
<:16
<:1;
<:1<
<;16
<;17
<;19
<;1;
43414
43319
<:18
<816
6W1#0DXULFH#$YH1
$ODER#6W1
$QGU\#6W1
3RODQG#$YH1
3DXOLQH#6W1
3LHW\#6W1
)
3UHVV#6W1
/RXLVD#6W1
0DQGHYLOOH#6W1
(VSODQGH#$YH1
7RXORVH#6W1
&DQDO#6W1
3R\GUDV#6W1
-XOLD#6W1
(UDWR#6W1#/RZHU
(UDWR#6W1#8SSHU
2UDQJH
0DUNHW
6W1#$QGUHZ#6W1
)LUVW#6W1
+DUERU#3ROLFH27KLUG#6W1
6HYHQWK#6W1
+DUPRQ\#6W1
/RXLVLDQD#$YH1#*/)/(
1DSROHRQ#$YH1#(
1DSROHRQ#$YH1#%
1DSROHRQ#$YH1#$
1DVKYLOOH#$YH1
+HQU\#&OD\#$YH1
*RYHUQRU#1LFKROOV

49
should be moored in the area of lowest
historical accident rate (Poydras Street to
First Street);
•
Gaming vessels should remain moored
during periods of low visibility, high winds,
or high river stage;
•
The potential for protecting the moored
gaming vessel by allowing berths to silt in
should be investigated;
•
Fully equipped rescue craft capable of
handling the volumes of passengers should
be available, either through the public sector
or by contracts with the private sector;
•
Contingency and disaster management plans
should be developed, and routine
preparedness drills should be held;
•
The issue of providing emergency egress
from passenger vessels to other vessels, to a
dock, or to a river bank should be
investigated. The objective must be to
remove passengers when underway or
moored during a crisis without having
persons resort to leaping into the water.
The phase I study reported expert opinion
that “high river stage was an important factor in
river casualties” and stated that this opinion was
supported by casualty data. According to that
data, casualties (allisions and collisions) show a
seasonal trend, with the high water months of
February, March, April, and May experiencing
two to three times the number of casualties as
the low-water months of July through October.
The phase I study did not determine the
frequency with which high-risk events were
likely to occur and thus could not provide an
overall estimate of risk for the port.
The phase II study developed methods to
further quantify the risk levels and thus enable
an evaluation of the overall risk, as well as risk
reduction, due to the mitigation measures
identified in phase I. A simulation of the Port of
New Orleans integrated the expert assessments
of phase I using available data, and simulation
results were validated against historical casualty
statistics. The simulation estimated that 2.24
vessels incidents per month could be expected in
the port area from miles 80 to 106 AHP and
that, of these incidents, 0.75 incident per month
could be expected between miles 90 and 95
AHP.
41
The phase II report reached the following
conclusions regarding gaming vessels:
•
The probability of occurrence of an incident
at high river stage is 10 times greater than at
low river stage;
•
A 25 percent increase in traffic in the river
would result in a 37 percent increase in the
number of vessel incidents that could be
expected.
One phase II study recommendation for
minimizing the risk of high-capacity passenger
vessel operation in the Port of New Orleans was
the following:
The Coast Guard and the Port of New
Orleans should ensure that response
plans and resources are adequate to deal
with a casualty involving a high-
capacity passenger vessel. Although the
probability of an incident involving one
of these vessels can be minimized, the
only way to minimize the potential
impact of such an event is to invest in
the resources and planning required to
effectively respond to such a casualty.
In 1993, the Governor’s Task Force on
Maritime Industry,
which addresses safety
issues on the Mississippi River and Mississippi
River—Gulf Outlet, formed a Marine Safety
Committee to address the issue of gaming
vessels berthing on the Mississippi River. The
committee was to solicit and promulgate
suggestions from local mariners regarding
protection of the areas in which gaming vessels
would be operating. The committee was later
subsumed into the Coast Guard Passenger
Vessel Safety Committee and other groups
formed by the Port of New Orleans to address
the issue of minimizing casualties from a
collision between a deep- or shallow-draft
vessel and a gaming vessel. This committee
functioned as an advisory group to the
41
Mile 95 AHP is at the approximate location of the
allision.

50
Governor’s Task Force and made the following
suggestions:
•
Assign a rescue boat to the immediate
vicinity of the gaming vessels and equip it
for handling a large number of passengers in
case of a casualty;
•
Station in the area a fully equipped fire boat,
which could be utilized as an additional
rescue boat;
•
Install a weather and river monitoring sys-
tem;.
•
Assign a dedicated communications marine
radio channel to be used by vessels
transiting the area;
•
Post and otherwise publicize notices to
mariners advising of this controlled zone;
•
Conduct joint Coast Guard, harbor police,
fire department, and police department
emergency preparedness drills;
•
Establish a fire and rescue station equipped
with a helicopter pad to provide rapid
evacuation in case of a casualty;
•
Ensure that all vessels are in full compliance
with classification society and Coast Guard
requirements;
•
Meet with all gaming interests to review
designs and recommendations of safety
programs.
One member of the advisory group
recommended that the area from the Crescent
City Connection Bridges to Canal Street be
allowed to silt in, forming a barrier 150 to 200
feet into the river to prevent deep-draft ships
from reaching the moored gaming vessels.
Operation Safe River
-- In January 1994, Coast
Guard Group New Orleans, together with the
New Orleans Port Authority Harbor Police, the
Crescent River Port Pilots Association, the City
of New Orleans Office of Emergency
Preparedness, and the Southeast Louisiana
Search and Rescue Organization, conducted a
joint search and rescue exercise on the
Mississippi River between the Crescent City
Connection Bridges and Algiers Point. The
exercise area included the section of the river
where gaming vessels were planned to berth and
operate. The exercise simulated a major marine
incident in the Mississippi River involving a
high-capacity passenger vessel. Weather
conditions during the exercise included an air
temperature of 40 °F and a water temperature of
34 °F. This real-time exercise demonstrated that,
during daylight hours with the resources
available, only 20 to 30 percent of people in the
water could be expected to be rescued.
Based on the results of this exercise and the
large number of vessel casualties—particularly
bridge allisions—that had occurred during 1993-
94, the Eighth Coast Guard District
implemented Operation Safe River to improve
safety on the Lower Mississippi River. The
operation initiatives called for a higher standard
of care by mariners and ordered COTPs to take
a harder line on enforcement and penalty
sanctions. The operation also included
initiatives to review the riverboat gaming vessel
program, focusing on the number of vessels and
their docking sites, as well as ferry vessel safety
pertaining to manning and operation.
According to Coast Guard officials,
initiatives developed as a result of Operation
Safe River have resulted in the following:
•
An extension of the regulated navigation
area for barge fleeting, resulting in a
reduction in barge breakaway incidents
because of improved barge fleeting
operating practices;
•
Improved reporting of vessel power and
steering losses by river pilots, and an
increase in the number of incidents in which
a pilot refuses to sail vessels with
navigational or engineering deficiencies;
•
Increased awareness by owners and
operators of their responsibility for safe
navigation in the river, resulting in a
reduction of incidents of vessel power or
steering loss;
•
Better adherence by owners and operators to
river draft requirements, resulting in a
reduced number of mid-channel groundings;
and

51
•
Year-round operation of the Algiers traffic
light.
Changes Made Since the Accident
--
Several steps were taken after the
Bright Field
accident to enhance safety in the Port of New
Orleans area.
River Front Alert Network
-- The Coast Guard
and the Dock Board, on March 11, 1997, agreed
to a memorandum of understanding establishing
a River Front Alert Network to provide early
warning of potential shipping disasters in the
area of the Port of New Orleans. The River
Front Alert Network is an 800 MHz emergency
radio alerting and communications system
installed at the Coast Guard’s Governor
Nicholls traffic light control tower and the Port
of New Orleans Harbor Police Department. The
system links the Governor Nicholls light, the
Harbor Police Department, the Delta Queen
Cruise Terminal, the Riverwalk Marketplace,
the Hilton Hotel, One River Place condomini-
ums, and the Aquarium of the Americas.
The River Front Alert Network is designed
to provide a capability to directly notify the Port
of New Orleans Harbor Police Department and
Port of New Orleans property tenants of a
potential threat caused by vessels navigating in
the vicinity of Algiers Point. Under the
memorandum of understanding, the alert signal
is initiated by the Governor Nicholls light
operator, who contacts the harbor police
dispatcher and the security officers of the
riverfront properties whenever an abnormality
or irregularity that could affect the riverfront
properties is identified or reported by a vessel in
the Algiers Point regulated navigation area. The
light operator is to transmit a short warning
message over the network describing the
situation. The dispatcher and the security
officers are to monitor the situation on the
marine radio and make their own judgments
about the appropriate response at their
properties. The network system is to be
activated as early as possible to provide the
maximum advance notice to the riverfront
properties. Once the situation is no longer a
threat, an “all clear” message is to be initiated
by the light operator.
Under the memorandum, the Dock Board is
responsible for installing and maintaining the
River Front Alert Network system hardware,
including system design, maintenance, support,
problem identification, and repair. The Port of
New Orleans is responsible for coordinating a
program to regularly test the network, including
the scheduling, participation, conduct, analysis,
and corrective action required to ensure the
system is functioning properly. The harbor
police are to implement standard operating
procedures defining the actions to be taken
when the network is activated during a possible
emergency incident, situation, or condition. The
port is to coordinate with the property tenants to
define the emergency actions to be taken when
the network is activated.
According to documentation provided by
the Dock Board on November 3, 1997, the board
has worked with the property tenants who
participate in the River Front Alert Network to
develop and implement standard operating
procedures for emergency evacuations. The
Dock Board reports that property tenants within
the River Front Alert Network zone have
updated their emergency plans to incorporate
the network alarm system and to provide
instructions for security officers to follow in the
event the Coast Guard light operator activates
the River Front Alert Network radio. Under the
updated procedures, security officers are to
listen to the broadcast from the Coast Guard
light operator, monitor VHF channels 16 or 67,
visually assess the situation on the river, and on
the basis of this information, determine whether
to order an evacuation of the property. The
security officers are authorized to initiate an
evacuation immediately based on the nature and
immediacy of the apparent river danger. Upon
determination that an evacuation is necessary,
security officers are to make public address
announcements of the evacuation and
implement those evacuation procedures that
have been established for their particular
locations.
New Notices, Rules, and Operating Regulations
--
In January 1997, the New Orleans COTP
identified passenger vessels deemed to be at risk
from allisions and issued written COTP orders
directing these vessels to (1) maintain a constant
bridge watch whenever passengers are
embarked, (2) maintain a constant monitoring
watch on VHF-FM channel 16 or other
appropriate emergency and bridge-to-bridge

52
radio frequency, and (3) be able to alert
passengers and other crewmembers and have the
ability to direct initial action in the event of an
emergency.
Also in January 1997, the New Orleans
COTP issued a notice that on vessels of more
than 1,600 gross tons, the anchors are to be kept
ready for immediate release and that, while the
anchor watch is in effect, effective
communications are to be provided between the
bridge and the foredeck.
On March 21, 1997, the commander of the
Eighth Coast Guard District issued temporary
rules applying new operating requirements to
self-propelled vessels of 1,600 gross tons or
more operating in the Mississippi River between
the South and Southwest Passes and mile 233.9
AHP. According to the Coast Guard, the new
requirements were prompted by the
Bright Field
accident and by subsequent unprecedented high
water levels in the river, which had led to “a
marked increase in vessel accidents.” These
temporary rules were extended twice; the
second extension was set to expire on October
31, 1997.
Before the expiration of the temporary rules,
the Coast Guard, on October 30, 1997,
published the new requirements as an interim
rule (33 CFR Part 165) in the
Federal Register
.
Interested parties have until December 29, 1997,
to comment. In its discussion of the rule, the
Coast Guard stated that the new requirements
were needed to “protect vessels, bridges,
shoreside facilities, commercial businesses and
the public from a safety hazard created by deep-
draft vessel operations along the Lower
Mississippi River.” The Coast Guard noted that
during 1995 and 1996, more than 300 self-
propelled vessels of 1,600 gross tons or greater
experienced loss of power, loss of steering, or
engine irregularities while operating in the
Mississippi River. It stated that the new rules
would enhance safe navigation of the river by
requiring that masters and engineers take
measures to minimize the risk of steering
casualties or engine failures/irregularities.
Under interim 33 CFR 165.810(e),
passengers vessels with one or more passengers
on board that are anchored or moored in the
Lower Mississippi River below mile 233.9 AHP
are required to keep a continuously manned
pilothouse,
42
and to
monitor river activities and marine VHF
emergency and working frequencies of
the port so as to be immediately
available to take necessary action to
protect the vessel, crew and passengers
in the event that an emergency radio
broadcast, danger signal or visual
indication of a problem is received or
detected.
Under interim 33 CFR 165.810(f), self-
propelled vessels of 1,600 gross tons or more
operating in the regulated area are to comply
with the following:
(1)
The engine room shall be
manned at all times while un-
derway in the RNA [Regulated
Navigation Area].
(2) Prior to embarking a pilot when
entering or getting underway in
the RNA, the master of each
vessel shall ensure that the ves-
sel is in compliance with 33
CFR Part 164 [specifying tests
of steering gear, internal vessel
control communications, emer-
gency generators, storage
batteries for emergency sys-
tems, and main propulsion
machinery, ahead and astern, all
of which are to be completed
prior to entering or getting
underway in U.S. navigable
waters].
(3)
The master shall ensure that the
chief engineer has certified that
the following additional oper-
ating conditions will be
satisfied so long as the vessel is
underway in the RNA:
(i) The main propulsion plant
is in all respects ready for
42
The rule exempts ferryboats and small passenger
vessels of less than 49-passenger capacity from this
requirement to maintain a manned pilothouse.

53
operations including the
main propulsion air start
systems, fuel systems,
lubricating systems, cooling
systems and automation
systems;
(ii) Cooling, lubricating and
fuel oil systems are at
proper operating tempera-
tures;
(iii) Automatic or load limiting
main propulsion plant
throttle systems are oper-
ating in manual mode with
engines available to im-
mediately answer maneu-
vering commands; and
(iv) Main propulsion standby
systems are ready to be
immediately placed in
service.
Steering Loss Study
-- After the
Bright Field
accident, a number of maritime, port
community, and public stakeholders in the Port
of New Orleans began to work together to
address mutual concerns. One result was a study
of propulsion and steering losses experienced in
the Lower Mississippi River, which was
expanded as a national issue for the Coast
Guard’s Navigation Safety Advisory Council
(NAVSAC). In April 1997, the NAVSAC
Navigation Equipment Committee concluded
that loss of propulsion and steering by vessels
while navigating the Mississippi River is a
national problem and that the nature of these
incidents is of great concern to all stakeholders.
The committee is exploring solutions, regulatory
and nonregulatory, that can be implemented to
help prevent steering and propulsion casualties.
Another area of concern to stakeholders was
development of objectives for a vessel traffic
system (VTS) for the Lower Mississippi River.
After the
Bright Field
allision, an ad hoc
committee produced in January 1997 a
“foundation of needs,” which addressed a
number of government, industry, and public
objectives for improved river safety. According
to the Coast Guard, it has designated the Lower
Mississippi River as the location of a
demonstration project for a new “silent” VTS
system that is expected to begin limited
operation in mid-1998. Under the silent VTS
system, vessels will be equipped with
transponders that will transmit a wide range of
vessel description and position information that
can be displayed on computer screens aboard
any vessel in the area. The system will provide
instantaneous and positive vessel information
while reducing VHF radio traffic.
Ship Drill Alarms
-- Immediately following the
Bright Field
accident, the president of the Port
of New Orleans issued a letter to the cruise line
owners at the Julia Street wharf asking them to
suspend the sounding of their ships’ whistles
during drills in order to avoid confusion about
the source and meaning of the whistle. The
letter requested that the cruise lines suspend the
drills and whistle soundings until they have
departed the Julia Street wharf. In addition, the
Port of New Orleans revised its general rules
and regulations to read:
No vessel, whether a cruise ship or an
excursion boat, shall sound a distress,
fire or emergency alarm as part of its
preparation drills while it is docked at
or near the Board’s wharves from Robin
Street to Governor Nicholls Street
except for such alarms required as part
of a vessel’s quarterly drills required to
maintain U.S. Coast Guard certification.
In the latter event, each vessel shall
notify in advance of such, the
surroundings of the Board’s Harbor
Police Department, the Hilton Hotel,
One River Place and the New Orleans
Riverwalk Associates. To the extent that
a vessel needs to familiarize passengers
with the sounds of such alarms as part
of its on-board safety drills, these
exercises should be conducted when the
vessel is either below the Governor
Nicholls Street wharf or above the
Robin Street wharf.
Riverwalk Marketplace Alert System
-- According
to minutes taken during a public Dock Board
meeting on February 6, 1997, the Riverwalk
Marketplace plans to install three cameras that
will monitor and display river traffic to all mall
merchants. The River Front Alert Network

54
provides an alarm to the Riverwalk security
desk, which then monitors maritime activities by
marine radio and visual monitoring. The
security desk determines the appropriate course
of action, including the sounding of evacuation
alarms. In addition, representatives of the
complex proposed the installation of a color-
coded alarm system display monitor that will
notify merchants of the type of evacuation
protocol to follow in the event of an emergency.
According to representatives of the
Riverwalk Marketplace, the public address
system in place at the time of the accident
operated through the mall’s Simplex alarm
system, which used speakers mounted at alarm
locations throughout the mall interior.
Emergency instructions were broadcast through
these speakers. Since the accident, the system
has been modified so that emergency messages
can be broadcast throughout the mall via the
background music system. Riverwalk is
investigating the possibility of a dual strobe-
horn combination alarm system that would alert
the mall tenants, employees, and patrons to the
type of evacuation required under various
emergency scenarios.
In an August 22, 1997, letter to the Safety
Board, a Dock Board official stated that the
Dock Board had encouraged the IRC to widen
the remaining portion of the Upper Poydras
Street wharf by 50 feet to match the portion of
the wharf that was previously widened to
accommodate gaming vessels. The Dock Board
also recommended that silt be allowed to
accumulate under the wharf as an additional
safety factor. The letter noted that the Dock
Board has no authority to compel the IRC to
carry out these modifications.
Vessel Egress
-- The Dock Board, in its
Public Protection and Emergency Management
Guidelines for Gaming Vessels and Berthing
Areas
, states that “a powered mobile elevating
platform suitable for emergency access or
casualty removal from upper decks is
conveniently available in the wharf area.” Also
in its August 22, 1997, letter, the Dock Board
described how the gaming vessel located at the
Poydras Street wharf has complied with the
Dock Board’s guidelines. The letter stated that
the
Queen of New Orleans
had provided an
elevator-equipped gangway and a wharf-
mounted crane.
The same guidelines state that “for
passenger use, at least two regular gangways
leading directly to the wharf are necessary.”
This guidance applies to all three vessels owned
by New Orleans Paddlewheels, Inc., (the
Queen
of New Orleans
, the
Creole Queen
, and the
Cajun Queen
). In its August 22, 1997, letter, the
Dock Board stated that:
The excursion vessels have aluminum
gangways as a secondary means of
egress in addition to their primary
gangways. The Flamingo (
Queen of
New Orleans
) has such emergency
gangways at all levels. The
Creole
Queen
and the
Cajun Queen
have
secondary emergency gangways and
additional gangways are currently on
order.
According to the Dock Board’s letter, both
the board and the Coast Guard require that
riverboat gaming vessels, excursion vessels,
riverfront commercial properties, and
oceangoing cruise ships prepare their own
emergency response plans and conduct related
training and drills. The Dock Board stated that it
had recently reviewed all such plans.
Status of the Queen of New Orleans
--
According to documentation received by the
Safety Board on October 22, 1997, the gaming
license of the
Queen of New Orleans
expired on
September 30, 1997, and the vessel was not
expected to resume operations in the Port of
New Orleans. Arrangements were reportedly
underway to have the vessel moved from the
Poydras Street wharf.

55
General
The following factors were determined not
to have been causal or contributory to the
accident involving the
Bright Field
: weather,
fatigue, malfunctioning of vessel steering gear
or equipment on the bridge, and alcohol or other
drugs. (See “Toxicological Testing” section of
this report for additional information.) The pilot
was properly licensed and certified by the State
of Louisiana and was qualified to serve in his
position. All officers of the
Bright Field
were
properly licensed and certified by the Liberian
government and were qualified to serve in their
positions.
The
Bright Field
was not, nor was it
required to be, equipped with a voyage data
recorder (VDR). (See appendix C.) Had it been
equipped with a fully configured VDR, valuable
information such as the vessel’s exact position,
course, rudder setting, throttle setting, engine
speed, and vessel speed at each point along the
accident track may have been available to
investigators. Such information could have been
used to perform a comprehensive computer
simulation that might have proved helpful in
evaluating engineering and human performance
on the day of the accident.
The major safety issues identified in this
investigation and discussed in this analysis are
the adequacy of the ship’s main engine and
automation systems, the adequacy of emergency
preparedness and evacuation plans for vessels
moored in the Poydras Street wharf area, and the
adequacy of port risk assessment for activities
within the Port of New Orleans. This analysis
also addresses three other issues: the actions of
the pilot and crew during the emergency, the
lack of effective communication (as it relates to
the actions of the pilot and crew aboard the
Bright Field
on the day of the accident), and the
delay in administering toxicological tests to the
vessel crew.
Accident Overview
The event that precipitated this accident, the
sudden and unexpected reduction in engine
power at a critical point in the
Bright Field’
s
navigation down the Mississippi River, was of
relatively short duration. However, the
combination of vessel speed, vessel direction,
river current, and high river stage left little
margin for error in responding to the emergency.
The
Bright Field
struck the wharf in an area
between two docked vessels, missing one of
them by less than 170 feet and coming to rest
only about 70 feet from the other. Thus, by
sheer chance, an allision with an occupied
passenger, gaming, or excursion vessel—and the
associated high risk of numerous serious
injuries—was barely averted. Even so, patrons
of a popular commercial district were placed in
jeopardy when the
Bright Field
struck portions
of shoreside buildings or undermined their
foundation supports. Had this accident occurred
during the evening, at night, or in the morning
hours, most of the hotel rooms that were
destroyed in the accident would probably have
been occupied. It is unlikely that even the River
Front Alert Network would have been able to
awaken the sleeping guests, alert them to the
danger, and evacuate them in time to prevent
serious injury or possible death.
The significant reduction in the
Bright
Field’
s engine power resulted from low main
engine lubricating oil system pressure and the
nonautomatic starting of the backup (No. 2)
lubricating oil pump. With main engine power
reduced and the ship swinging toward the
Riverwalk, the time and options available to the
pilot and crew to avoid an allision were limited.
The options involved pulling ahead and
maneuvering out of danger, slowing and steering
away, or stopping; however, exercising any of
these options would have required more time,
propulsion power, or steering control than were
available to the
Bright Field
in the moments
before the allision. The Safety Board could
therefore not determine whether the pilot or
crew could have done anything to prevent this
accident. The same constraints on power and
ANALYSIS

56
control that hindered efforts to prevent the
accident also may have rendered ineffective the
actions that the pilot and crew did take prior to
the allision. Thus, the final rest position of the
Bright Field
may have resulted from the
combined forces of the ship and the river rather
than from the efforts of the pilot or crew. The
substantial role played by chance in this
accident has important implications for
assessing risk in and around the river, as will be
discussed below.
The investigation of this accident revealed a
history of maintenance and operational
problems associated with the main propulsion
engine of the
Bright Field
. These problems were
known to the vessel’s owners, who did not
correct them in a timely fashion. On the open
sea, in good weather, temporary malfunctions in
the vessel’s main engine may be tolerable;
however, in the close quarters of the Mississippi
River, where safe maneuvering is directly
dependent upon a responsive main engine, a loss
of power can, as it did in this instance, present
an immediate threat to other vessels and to
shoreside facilities.
Complicating the emergency created by the
loss of engine power on the
Bright Field
was the
interaction between the river pilot and the ship’s
master and crew on the vessel’s bridge. At
several points prior to and during the
Bright
Field
emergency, the pilot, master, and crew of
the vessel did not exchange important
information about the nature of the emergency
and its potential outcome. In slightly different
circumstances, the limited communication
between the pilot and the ship’s crew could have
compromised the vessel’s ability to recover
from a threatening situation.
Some of the injuries resulting from the
accident were sustained by gaming and
excursion vessel passengers as they attempted to
escape what appeared to be an imminent
allision. The lack of adequate numbers of
readily available egress routes, in addition to the
lack of effective evacuation procedures and
plans aboard the vessel on which numerous
injuries occurred, contributed to the number and
severity of injuries. The lack of advance
warning to the patrons and employees of the
Riverwalk Marketplace also contributed to the
number of injuries.
This accident demonstrates the risk
represented by heavily loaded, (relatively) high-
speed vessels navigating a twisting waterway
bordered both by populated wharves and
mooring areas for passenger vessels. While the
absolute elimination of all risk associated with
this operating environment would be impossible,
in the view of the Safety Board, opportunities
exist to reduce the risk of vessel collisions and
allisions and to reduce the vulnerability of
shoreside facilities.
Engineering Aspects
Main Engine Shutdown and Restart
--
About 1406 on the day of the accident, as the
Bright Field
was passing under the Crescent
City Connection Bridges, the vessel’s automated
propulsion control system reported low main
engine lubricating oil pressure and main engine
trip (shutdown) due to low lubricating oil
pressure. The chief engineer stated that, when
the alarms sounded, he noted that the lubricating
oil system had depressurized.
The complete shutdown of the main engine
was not immediately apparent to those on the
bridge or in the control room because the
“windmilling” effect as the vessel moved
through the water kept the propeller (and thus
the directly connected engine) turning at about
30 rpm. In fact, the engine probably did not
come to a complete stop before the chief
engineer cleared the fault indication and
restarted the engine. The alarm log printout
indicated that the power reduction was the result
of main engine trip due to low main engine
lubricating oil system pressure.
When Safety Board investigators boarded
the
Bright Field
2 days after the accident, both
the No. 1 and No. 2 lubricating oil pumps were
running. Had the oil pump backup system been
functioning on the day of the accident, and had
it been set to automatic mode, the No. 2 oil
pump would have started automatically when
the system sensed a drop in main engine oil
pressure. The system alarm log printout for that
day, however, did not indicate the automatic
starting of the second pump. Moreover, Safety
Board tests showed that the pressure switch that
would have automatically started the second
pump may have been inoperative on the day of
the accident and therefore would have been

57
unable to effect the changeover, even with the
No. 2 oil pump set on automatic standby. On the
day of the accident, then, either the automated
propulsion control system was not set up for
automatic starting of the standby lubricating oil
pump or the switch that accomplishes the
changeover failed to respond properly to the
drop in system pressure.
During interviews with Safety Board
investigators, no crewmember acknowledged
manually starting the No. 2 pump; however, the
pump could only have been started either
automatically—which would have been
recorded on the alarm log printout—or
manually. The evidence indicates, therefore, that
a crewmember did, in fact, manually start (by
either turning the switch to auto start or by
initiating a manual start on the pump motor
control panel when the changeover switch
failed) the standby oil pump after the
Bright
Field’
s main engine shut down because of low
lubricating oil pressure. The restoration of
sufficient oil pressure allowed the engine to be
restarted.
Lubricating Oil Pump Operation
--
Although the main engine lubricating oil system
pressure with the No. 1 lubricating oil pump
running was consistently observed over a period
of several days after the accident to be about 2.3
bar, the exact cause of the low pressure in the
lubricating oil system could not be determined.
Following teardown, cleaning, adjustment, and
reassembly of the No. 1 lubricating oil pump,
the outlet pressures reached the rated pressure of
4 bar. Shortly after the pump was reinstalled, it
again displayed the vibration and noisy
operation that had been noted in earlier
inspections and that had been reported to the
vessel owners by the chief engineer before the
accident. The source of the vibration and noise
could not be determined; however, the No. 1
lubricating oil pump continued to produce rated
pressure.
According to the system monitor printout, at
1400 on the day of the accident, main engine
lubricating oil pressure was 2.64 bar. Although
system pressure was in the acceptable range, it
was critically close to the system’s low-
pressure-alarm level. This slight differential
between the system’s operating pressure and the
alarm/trip pressure settings (2.5/2.3 bar) was
due primarily to the pressure drop across the
second filter, which resulted when contaminants
in the oil clogged the fine mesh screen of the
second filter’s strainers. This determination is
consistent with the repeated second filter high-
differential-pressure alarms recorded during the
December 14 voyage as well as with the results
of testing of the second filter.
At 1406, the pressure had dropped below
2.3, as evidenced by the protection system’s
tripping the main engine off line. Several causes
of this sudden pressure drop were considered,
then discounted, because they would have
produced outcomes that were inconsistent with
information gathered in the investigation. Those
causes include heavy pump cavitation from
aeration of the lubricating oil; failure of the No.
2 oil pump’s discharge stop check valve, which
would have allowed “backflow” of oil through
the No. 2 pump; a faulty pressure relief valve on
the No. 1 pump, which would have allowed oil
to backflow to the suction side of the No. 1
pump; catastrophic failure of the main engine
lubricating oil system’s piping; and manual
intervention.
Several other possible causes of the sudden
drop in lubrication oil system pressure could not
be discounted. These included the vibration and
noise problem in both oil pumps that had been
noted by the chief engineer weeks before the
accident and was never corrected and the
abnormally low level of lubricating oil in the
main engine sump. Incessant pump and piping
vibration could have precipitated a transient air
leak in the fittings associated with the No. 1 oil
pump. Or the No. 1 oil pump may have become
airbound after pulling in air through the oil
sump suction pipe inlet because of the low level
of oil in the sump. Either condition would have
allowed air to be drawn into the suction side of
the pump, resulting in the rapid oil system
depressurization observed by the chief engineer.
In such an event, unless the standby pump is
started immediately, the depressurization can
result in engine trip; as previously noted, the
No. 2 pump was either not on automatic
standby, or the automatic switching mechanism
failed to operate on the day of the accident.
General Condition of the Bright Field’s
Engineering Plant
-- Safety Board
investigators’ examination of the engineering

58
plant and maintenance records for the
Bright
Field
revealed, as noted earlier, engine
lubricating oil that was not within the allowable
specifications of the oil supplier or engine
designer, excessive differential pressure across
the second oil filter, and uncorrected vibration
and noise from both main engine lubricating oil
pumps. Among other deficiencies identified
were marginal lubricating oil sump level,
incorrectly calibrated sensing devices, reuse of
worn parts, and numerous other problems
associated with the main engine and various
auxiliary systems/machinery. While many of the
deficiencies noted by the New Sulzer Diesel
technician and chief engineer were corrected
before the December 14 voyage, the vessel
sailed with several significant engineering
problems uncorrected.
A review of the vessel’s records dating back
to January 1996 revealed that the engineering
crew responded to recurring engineering failures
with repairs that were sufficient to keep the
vessel operating most of the time. However, the
crew apparently was not able to make
permanent repairs to the vessel’s main engine
and associated engineering systems; as a result,
these problems became a continuing source of
voyage disruptions. In the 3 months prior to the
accident, the
Bright Field
added about 1 month
to its schedule due to delays attributed to
engineering problems.
The crew was not required to use the
automated propulsion control test procedures
that were delivered with the vessel in 1988 or to
periodically test the functional operability of the
automated propulsion control system. The
engineering plant on the
Bright Field
was
equipped with a number of safety devices, and
the chief electrician submitted a report
concerning the status of these devices to the
vessel’s owners quarterly. But the report was
based only on a survey of alarms and sensors.
No one regularly performed operational testing
and maintenance of safety control devices such
as the oil pressure switch that was supposed to
start the standby oil pump in case of a drop in
main engine lubricating oil pressure.
While the
Bright Field’
s owners provided
each vessel in their fleet with general
requirements for periodic testing and
maintenance of the main engine, including
regular analysis of the main engine lubricating
oil, Safety Board investigators determined that
critical main engine components were run until
failure occurred and that periodic preventive
maintenance was not routinely accomplished.
The Safety Board concludes that the
Bright
Field
showed evidence of recurring engineering
problems that affected vessel main engine
reliability, and had all engineering systems been
kept in good repair and regularly tested, the
vessel may not have unexpectedly lost power
during its voyage down the Mississippi River.
The Safety Board believes that Clearsky
Shipping Company should perform a baseline
engineering assessment of the
Bright Field’
s
engineering plant and correct all conditions not
in conformance with manufacturer’s
specifications.
Vessel Owner’s Oversight of the Bright
Field’s Engineering Plant
-- The
Bright Field’
s
owners, Clearsky Shipping Company, received
regular engineering and maintenance reports on
the
Bright Field
and thus had knowledge of the
vessel’s engineering problems. Serious
engineering problems were reported to the
owners as early as January 1996. In addition to
reports from the engineering crew, the owners
had received periodic telexes from the master
documenting the severity of engineering
problems, delays in scheduling resulting from
the engineering problems, and the inability of
the engineering crew to make permanent repairs.
The Safety Board acknowledges that, on at least
one occasion in 1996, the
Bright Field’
s
owners’ representatives visited the vessel
because of concerns about the operation of the
engineering plant. The owners also replaced the
Bright Field’
s chief engineer when the vessel
arrived in New Orleans on November 21
because, they said, the engineer had been
unresponsive to the owners’ orders. The
documented problems with the
Bright Field’
s
engineering plant, however, existed at least as
early as 1995, which predated the arrival on
board of the previous chief engineer. These
engineering deficiencies are indicative of long-
term, recurring problems that cannot be tied to
the competence or job performance of a single
individual.
The Safety Board concludes that the
Bright
Field
owners’ oversight of testing and

59
maintenance of the vessel’s engineering systems
was inadequate and led to unreliable
performance of the engineering plant and
contributed to the shutdown of the main
propulsion engine on the day of the accident.
The Safety Board believes that Clearsky
Shipping Company should institute an
engineering testing, maintenance, repair, and
company oversight program for the
Bright Field
that will ensure safe and reliable operation of
the vessel’s engineering plant.
Communication
Quite by chance, the
Bright Field
came to
rest between two docked ships in a space not
significantly larger than the ship itself. While
the actions of the pilot and crew during the
emergency may have been reasonable, their
actions were not well coordinated. Because a
computer simulation of the accident scenario
was inconclusive, the Safety Board could not
determine how changes in the nature or timing
of the crew’s actions may have affected the
outcome. The Safety Board therefore concludes
that insufficient information was available to
determine whether any actions taken by the pilot
and crew of the
Bright Field
would have been
effective in preventing the allision or mitigating
its effects. The Safety Board also concludes,
however, that at several points prior to and
during the
Bright Field
emergency, the pilot,
master, and crew of the vessel did not exchange
information that under other circumstances
could have prevented or at least mitigated the
effects of the accident.
In the view of the Safety Board, the
performance of the
Bright Field
pilot and crew
could have benefited from effective application
of the principles of BRM, which entails
effective use of all available resources to
achieve safe operations. The Safety Board has
long supported mariners’ use of BRM
techniques and has advocated professional
training in BRM.
Underlying effective BRM is an
understanding that every officer, crewmember,
and pilot on board a vessel is responsible for
acting and for using resources in close
coordination with others on the watch. The
master, pilot, and conning officer use leadership
skills and command authority to integrate the
resources for any given passage or watch. At the
same time, they must convey their receptivity to
operating information that originates with
subordinates. The role of those on the watch is
to perform their assigned tasks responsibly, to
know about or participate in determining the
plans for navigation of the vessel, to be alert to
departures from plans or from the expected
performance of others, and to make those
discrepancies known in time to avert an
operational error. The practice of BRM by pilots
and crew can be handicapped by intercultural or
language differences, but these can often be
overcome by deliberate and clear
master/pilot/crew briefings.
Master-Pilot Briefing at the Anchorage
--
The pilot of the
Bright Field
did not advise the
master of his plans for making the river transit,
including the fact that he intended to operate the
ship at sea speed. Had the pilot offered, or had
the master requested, information on the transit
plans, not only would both men, as well as the
bridge crew, have known when and where to
expect various actions, but the flow of
information could have enhanced coordination
and confidence between the pilot, master, and
crew.
If, for example, the master had asked, or the
pilot had offered, information on the pilot’s
intended transit speed, that issue could have
been discussed, and together they could have
evaluated the operational consequences of
proceeding at sea speed. Navigational situations
can develop at any time for which an increase in
speed (to improve rudder control or avoid
collision) is a viable option, but, when a ship is
already operating at top speed, that option is no
longer available. If the pilot and master had
discussed the intended speed, they could have
reached a consensus on the best way to operate.
Although a discussion of intended actions
can take place at any time during a transit,
predeparture discussions generally provide the
greatest latitude in both time and options. A
predeparture discussion also avoids some of the
practical logistical problems (related to
obtaining another pilot) that could arise if a
serious disagreement occurs between a master
and a pilot once a trip begins. Thus, discussing
and agreeing on transit plans before getting
underway is more efficient.

60
A transit plan should include intended
speeds, areas of high risk due to traffic
concentration, shoreside structures, or river flow
characteristics, and actions to be taken in the
event of various ship power or control
difficulties. According to their statements, each
man felt confident of his own abilities and
assumed that the other was qualified to perform
any duties that might be required. The lack of
discussions between the master and pilot
regarding emergency maneuvering procedures
did not cause this accident. Still, if the actions to
be taken in an emergency had been established,
cooperation and coordination in the emergency
that developed would probably have been
enhanced, tasks could have been clearly
delineated, and orders (such as the order to drop
anchor) could perhaps have been given and
complied with more quickly.
While the pilot was not forthcoming with
information about his transit plans, the master
did not tell the pilot of the inability to start the
main engine from the bridge either at 1055 or
when the same difficulty was encountered at
1110. In each case, engine control had to be
transferred to the engine control room and back,
but this information was not made known to the
pilot. Had the pilot been made aware of the
situation, he and the master could have
discussed options, including the location of
engine control (control room or wheelhouse) or
use of tug escorts. If the pilot and master could
not agree, the pilot could have refused to get
underway from the anchorage.
Language Differences
-- Even though the
ship’s master and crew were Chinese and spoke
their native language among themselves,
interchanges between the crew and the pilot
took place in English. The language difference
between the pilot and the crew does not appear
to have been a significant impediment to
communications on the bridge.
The fact that the crew spoke Chinese among
themselves, however, eliminated an adjunct
source of information for the pilot. For example,
because conversations between master and crew
were in Chinese, the pilot was not aware of the
engine starting difficulties, the content of the
second mate’s conversation with the chief
engineer, or the master’s order to drop the
anchor. Of course, critical operational
information should be clearly stated, and no
operations should depend exclusively on
overhearing a conversation. But the language
differences on the bridge, combined with the
fact that the ship was sailing in restricted waters,
made it even more important that the master and
crew convey all operations-related information
to the pilot. If the master and crew did not take
this initiative, then the pilot should have
specifically requested that he be kept informed
of all activities and conversations on the bridge
affecting vessel operation. Such ongoing
communication did not occur on the bridge of
the
Bright Field
.
Information Exchange During the
Emergency
-- If more information had been
exchanged during the brief period after power
reduction and before the allision, the actions of
the pilot and crew could have been better
coordinated and perhaps more timely. Even
though the eventual outcome would probably
have been the same in this case, in different
circumstances, more effective communication
could have helped avoid or mitigate an accident.
When the pilot noticed the cessation of
vibration in the vessel, he asked if there was a
problem. Even though he stated that neither the
master nor the mate responded, he did not ask a
second time. By not following up and
attempting to determine the exact nature of the
problem, the pilot denied himself information
that may have influenced the nature or the
timing of his navigational decisions and orders.
When the pilot realized that the vessel had,
in fact, lost power, he again did not converse
with the master or mate. Consequently, he was
unaware of what they were doing or could do to
address the problem. Although the master and
the mate were attempting to restore engine rpm,
they did not tell the pilot of their actions.
A limited information exchange took place
among the master, second mate, and chief
engineer. The master instructed the second mate
to call the engine control room and demand an
immediate increase in speed. The second mate
complied. In response, the chief engineer said he
understood what had happened (a sudden drop
in the pressure of the lubricating oil pump), but
not why it happened, and told the second mate
so. He also told the second mate the

61
pressurization problem had already been solved
by the No. 2 pump coming on line. He then
asked if the second mate wanted to switch
engine control from the bridge to the engine
control room. The second mate said yes, and the
transfer of control began.
During the postaccident investigation, the
master explained why engine control was
transferred. He said it was standard procedure to
give the engineroom control whenever a
problem occurred that involved the engine, and
that under normal circumstances, the engine rpm
could be brought up more quickly from the
engineroom. Following this normal procedure
would seem to make sense, since the master
acknowledged that he did not know the nature of
the problem that caused the rpm reduction.
However, the transfer of control takes 20 to 30
seconds and must be completed before engine
speed can begin to be restored.
In this case, since the pressurization
problem had already been corrected, the rpm
could have been restored from the bridge as
quickly as from the engineroom. If that had been
done, the transfer time could have been saved.
However, the second mate apparently did not
recognize the implication of the chief engineer’s
comment, which was that the second engineer
could increase rpm himself. So when the chief
engineer asked if engine control should be
transferred, the second mate agreed. The second
mate was quite likely simply following the
master’s order to have “them” (the chief
engineer and his staff) increase speed. If the
chief engineer had supplied information to the
bridge about the time necessary for him to
assume control and restore engine rpm, this
information may have altered the nature and
timing of the master’s and pilot’s orders.
The second mate also did not immediately
pass on the information about the lubricating oil
repressurization to the master. If he had, the
master may have recognized his option to
increase rpm from the bridge, and the normal
practice of sending engine control to the engine
control room in the event of engine-related
problems may not have been followed, thereby
saving the control transfer time. Likewise, if the
second mate had given the chief engineer
additional information about the direction in
which the ship was headed, the chief engineer
could have made a more informed decision
concerning the options for increasing rpm, such
as activating the crash maneuvering feature or
perhaps not transferring engine control to the
engine control room. After the accident, the
master testified that the engineering crew was
not made aware of the emergency situation until
the allision was unavoidable.
Had the above additional information been
supplied during these exchanges, it may not
have altered the outcome. Nevertheless,
additional information should have been
exchanged to facilitate decisions.
Another information exchange between the
pilot and master affected the order to drop
anchor. During the accident sequence, the pilot
first ordered the master to have someone stand
by the anchors and, later, to drop the anchors.
The orders were heard and understood by the
master, though the pilot was unaware of that
because the master did not acknowledge either
order. The master attempted to carry out the
order to drop anchor, but his radio
communications with the carpenter at the bow
were impeded by the sound of the ship’s
whistle. The master did not tell the pilot of the
communication problem created by the whistle;
instead, he went out to the bridge wing and tried
to attract the carpenter’s attention by waving his
arms. When this effort failed, the master tried
the radio again, finally establishing intermittent
contact. He still did not tell the pilot of his
difficulties.
In the meantime, the pilot did not realize
that he was preventing his own order from being
carried out by continuing to sound the ship’s
whistle. Transmission of the order was delayed
so long that when the master finally reached the
carpenter on the radio, he deemed dropping the
anchor to be an inappropriate order and
countermanded it. By the time the master
decided to drop the anchor, the carpenter could
make only a brief effort to carry out the order
before having to flee to escape injury in the
imminent allision. As a result, and as confirmed
by an amateur video of the accident, the anchor
was not dropped before the
Bright Field
struck
the wharf.
The fact that the pilot issued the order to
drop anchor indicates that he believed that some

62
value, however small, could be gained by
dropping one or both anchors. Had he not
believed that dropping anchors could mitigate
the emergency, he was obligated to relay that
information to the master so the carpenter could
be told to abandon the anchor watch and remove
himself to a safer position. Yet the pilot made
no real effort to determine if his order had been
carried out, even when he saw the master go to
the bridge wing and wave his arms. If he did not
recognize that effort as an attempt to
communicate with the anchor watch, he should
have inquired about the meaning of the master’s
unusual actions at such a critical time.
The lack of information exchange and
feedback on the part of the master is also
notable. For example, he did not tell the pilot
that he had countermanded the drop-anchor
order, only to reissue it a little later. Earlier in
the accident sequence, he did not ensure that the
pilot was fully aware of the actions he was
taking to restore engine rpm. While the pilot
could have inferred the master’s actions from
the rpm indicator, the master should have
removed any ambiguity by advising the pilot of
what he was doing at all times. Likewise the
master could have given the pilot an estimate of
the time it might take to restore engine power. If
he did not know the amount of time needed, he
could have asked the chief engineer. The pilot
could have used each of these pieces of
information as he determined which orders to
issue at what time.
The need to exchange information and
ensure that orders are heard, understood, and
carried out is basic to the operation of any
vessel. These needs are not new and have long
been familiar to mariners; however, they have in
recent years been formalized as central elements
of BRM. The Safety Board concludes that use of
BRM precepts on board the
Bright Field
would
have enhanced the exchange of information and
the coordination of actions among the pilot,
master, and crew during the accident sequence.
The Safety Board has issued several
recommendations concerning BRM since 1991.
Due in part to those recommendations and the
efforts of the Coast Guard, the International
Maritime Organization (IMO) has issued
amendments to its Standards of Training,
Certification and Watchkeeping that
incorporate BRM training for watch officers
effective February 1, 1997. A 5-year phase-in
period (from February 1, 1997) to certify
licensed watch officers will follow. Signatory
countries are to have plans for such training
programs in place by February 1, 1998. All
signatory countries, including the United States
and Liberia (flag of the
Bright Field
), will
require officers of vessels such as the
Bright
Field
to have BRM training. Pilots will not be
subject to the same training unless they hold a
Coast Guard license.
Training in BRM typically includes five
generic categories of knowledge and skill
development: (1) the development and perform-
ance of watch or pilot briefings; (2)
maintenance of situational awareness; (3) identi-
fication of error chains (and error trapping); (4)
implementation of effective bridge/vessel com-
munication; and (5) integration (coordination)
of bridge/vessel resources. In whole or in part,
most of theses elements were missing during the
Bright Field’
s December 14, 1996, voyage.
The Safety Board believes that NOBRA
should encourage its members to participate in
initial and recurrent BRM training that
emphasizes team coordination between the pilot
and crew. The Safety Board further believes that
Clearsky Shipping Company should provide its
bridge and engineroom watchstanding officers
and crewmembers with initial and recurrent
BRM training that includes communication and
coordination between pilots and members of the
bridge and engineroom watches and that
addresses their use of bridge and engineroom
systems.
Emergency Response
After the allision, rescue efforts were
initiated at once, and emergency units were
ordered. The harbor police dispatcher notified
the city of New Orleans Fire, Police, and Health
and Emergency Services Departments. More
than 25 agencies responded; fire, police, and
emergency medical service units arrived on
scene within minutes. After being contacted by
the Gretna light operator, the Coast Guard began
an immediate search and rescue response. In
addition to providing assistance through
multiple city agencies, the city of New Orleans
contacted the Louisiana Office of Emergency

63
Preparedness to provide notification and request
standby for possible assistance.
Passengers aboard the cruise ships and the
gaming and excursion vessels, as well as several
Riverwalk Marketplace patrons, in response to
Safety Board questionnaires recalled the
emergency response as prompt and efficient.
Although initial access to the area was hindered
by damage occurring when the
Bright Field
struck the wharf, the emergency responders
were able to locate and use an acceptable
alternate route to respond to the incident, assist
the injured, and provide crowd control. The
Safety Board concludes that the response to the
Bright Field
accident by local emergency
response agencies was timely and appropriate.
Vessel Emergency Preparedness and
Evacuation Plans
Four vessels were docked alongside the
wharf in the area of the
Bright Field
accident:
the
Enchanted Isle
, the
Nieuw Amsterdam
, the
Queen of New Orleans
, and the
Creole Queen
.
In the view of the Safety Board, the actions of
the captains and crews aboard the cruise ships
Enchanted Isle
and
Nieuw Amsterdam
in the
moments preceding the allision were adequate
for the circumstances. An emergency evacuation
was not attempted because of the limited
amount of time that elapsed from the first
awareness of the emergency until the
Bright
Field
passed clear of the two vessels.
Vessel Evacuation
-- According to Safety
Board surveys of passengers, when the first
mate of the
Queen of New Orleans
made the
initial evacuation announcement, some
passengers did not respond immediately. When
a second announcement was made ordering the
immediate evacuation of the vessel, passengers
and nonoperating crewmembers began running
toward the gangway. About this time, the
Bright
Field
struck the wharf and was continuing to
move toward the bow of the
Queen of New
Orleans
. Even though the bow wave from the
Bright Field’
s approach destabilized the second
deck gangway of the
Queen of New Orleans
several times during the evacuation process,
passengers were not provided with an
alternative means of access to the dock.
According to the
Queen of New Orleans
’
Emergency Evacuation Plan for Moored
Conditions
, the vessel can be exited only from
the bow section of the second deck. The plan
states that to evacuate the vessel in an
emergency, every passenger is to be directed to
this gangway. The owner of the vessel noted
that three portable emergency gangways, which
are designed to be used in the event the main
gangway is inoperable, were aboard the vessel.
The vessel’s emergency evacuation plan,
however, does not refer to these portable
gangways, or provide instructions on how to
make them operable in an emergency, or give
guidance for directing passengers to them. The
evacuation plan also does not take into account
the time needed to alert the crew to take action
or for crewmembers to stage the portable
gangways and ensure their safe operation.
Because the emergency gangways were not used
during the
Bright Field
accident, the only exit
available was the second deck bow gangway.
New Orleans Paddlewheels, Inc., provided
security camera videotapes that show areas of
the vessel being evacuated in what company
officials call “a calm and orderly evacuation.”
The Safety Board did not see, on these tapes,
any passengers sustaining injuries during the
evacuation. Nonetheless, some passengers were
injured, as documented by medical records.
While the Safety Board recognizes that the
number of questionnaire responses was small
relative to the number of passengers aboard the
vessel, the responses are nevertheless
meaningful and illustrate the panic induced
when the crowd was confronted with no means
of escape from a vessel directly threatened by an
oncoming freighter. Furthermore, had the vessel
been filled to its capacity of 1,800 passengers
and crewmembers, the number of persons
unable to evacuate in time could have been
significantly higher. The ensuing panic most
likely would have been more hazardous,
possibly resulting in a higher number of, and
more severe, injuries. The Safety Board
concludes that evacuation of the
Queen of New
Orleans
was hampered, and passenger risk
increased, by the fact that only one gangway
was made available for passenger egress during
the emergency.
The
Creole Queen
, a New Orleans
Paddlewheels, Inc., excursion vessel with a

64
capacity of 1,000 passengers and crew, was
docked astern of the
Queen of New Orleans
. At
the time of the accident, 190 passengers and
crewmembers were aboard. Following the
master’s instructions to evacuate, passengers
exited the vessel across a single dockside
gangway. When the bow wave from the
Bright
Field
passed the
Creole Queen
, the gangway
dropped from the side of the vessel, and three
passengers on the gangway fell into the river.
One passenger was seriously injured; the other
two sustained minor injuries. By this time,
approximately one half of the
Creole Queen
’s
passengers had been evacuated. The remaining
passengers could not exit the vessel until the
gangway was repositioned.
The Safety Board acknowledges the efforts
of the senior officers of both vessels to evacuate
a large number of passengers. Even so, if the
36,000-ton
Bright Field
had struck the
Queen of
New Orleans
, the remaining passengers still on
board the gaming vessel, regardless of the exact
number, would have been in grave danger.
The Safety Board believes that New Orleans
Paddlewheels, Inc., must make better provisions
for all its vessels in the event of an impending
allision or other emergency. Consequently, the
Safety Board issued the following safety rec-
ommendations to New Orleans Paddlewheels,
Inc., on September 5, 1997:
Work with the U.S. Coast Guard to
review the
Emergency Evacuation Plan
for Moored Conditions
of the
Queen of
New Orleans
and amend it regarding
current evacuation procedures and the
number of immediately accessible
gangways and disembarkation locations,
to ensure timely and orderly exiting of
passengers in the event of emergency
evacuation. (M-97-62)
Work with the U.S. Coast Guard to
develop and implement procedures for
evacuation under moored or docked
conditions for all your excursion vessels
to ensure that passengers can exit each
vessel in a timely and orderly manner
should an emergency evacuation be
necessary. (M-97-63)
In a September 29, 1997, letter to the Safety
Board, New Orleans Paddlewheels, Inc., replied
that its emergency evacuation plan for the
Queen of New Orleans
in moored conditions
addresses the evacuation of all areas on
board the vessel. We purposely did not
include portable gangways because they
are to be used only when the primary
evacuation gangway is inoperable. Our
deck crew is regularly trained and
drilled on how to use these portable
gangways in multiple locations.
Portable gangways were not used in this
emergency. The Safety Board is concerned that
the evacuation plan for the
Queen of New
Orleans
does not provide a readily available
additional means of escape that does not require
staging in an emergency. The Safety Board’s
intent in issuing Safety Recommendation M-97-
62 was to prompt New Orleans Paddlewheels,
Inc., to amend the
Queen of New Orleans
’s
Evacuation Plan for Moored Conditions
not
only to enhance evacuation procedures, but also
to address the need to provide for more than one
immediately accessible disembarkation location
to ensure a timely and orderly exiting of
passengers.
Further, although the September 29 letter
states that the deck crew is trained and drilled
on use of the portable gangways, the letter does
not address the training of the nonoperating
crewmembers, who are responsible for assisting
passengers to the egress areas of the vessel
during emergencies. The
Evacuation Plan for
Moored Conditions
provides no guidance on the
use of portable gangways to the numerous
nonoperating crew on board the vessel who are
responsible for directing passengers and
assisting their escape. Moreover, the specific
plan to which all crewmembers are to look for
guidance in responding to emergency situations
does not provide any information on these
gangways or how to guide passengers to them.
Based on the failure of New Orleans
Paddlewheels, Inc., to effectively address these
concerns, the Safety Board classifies Safety
Recommendation M-97-62 “Closed--
Unacceptable Action.” New Orleans
Paddlewheels, Inc., has not responded to Safety
Recommendation M-97-63 concerning the
development of evacuation procedures for

65
moored or docked conditions for all its
excursion vessels. Therefore, Safety
Recommendation M-97-63 remains classified
“Open--Await Response.”
The Safety Board, also on September 5,
1997, issued the following safety recommenda-
tion to the Coast Guard:
Work with New Orleans Paddlewheels,
Inc., to review and amend the
Emer-
gency Evacuation Plan for Moored
Conditions
of the
Queen of New
Orleans
regarding current evacuation
procedures and the number of immedi-
ately accessible gangways and
disembarkation locations, and to
develop and implement procedures for
evacuation under moored or docked
conditions for all New Orleans Paddle-
wheels, Inc., excursion vessels to ensure
that passengers can exit each vessel in a
timely and orderly manner should an
emergency evacuation be necessary.
(M-97-59)
In a November 18, 1997, letter, the Coast
Guard responded that the New Orleans COTP
had already required a review of evacuation
procedures for all high-capacity gaming vessels,
but that the Coast Guard believes this safety
recommendation should be expanded to cover
all passenger vessels operating in the
Mississippi River in the New Orleans area. The
letter stated the Coast Guard’s belief that,
It would be prudent to develop
reasonable, practical and appropriate
evacuation criteria for the different
types of passenger vessels based upon
their type, configuration, passenger and
crew capacity, and the extent which
passengers are normally aboard the
vessel while dockside. To this end, we
have discussed the expansion of this
recommendation with Captain of the
Port New Orleans and will require
further review and development of this
initiative.
The Safety Board is pleased that the Coast
Guard has not only addressed the specific intent
of Safety Recommendation M-97-59 regarding
the
Queen of New Orleans
, but has also
expanded the scope of the recommendation to
cover all high-capacity passenger vessels
operating within the Port of New Orleans. While
the Coast Guard response does not specifically
address evacuation plans for New Orleans
Paddlewheels excursion vessels, the Safety
Board notes that these vessels will be covered
by the evacuation criteria the Coast Guard plans
to develop for all passenger vessels operating in
the New Orleans area of the Mississippi River.
Pending further information from the Coast
Guard regarding the proposed review of
evacuation plans for such vessels, and
specifically those vessels belonging to New
Orleans Paddlewheels, Inc., the Safety Board
classifies Safety Recommendation M-97-59
“Open--Acceptable Response.”
Emergency Drills
-- The company
operating manuals and station bills for both the
Queen of New Orleans
and the
Creole Queen
clearly stated that nonoperating crewmembers
were responsible for distributing life jackets,
keeping order in the stairways and passageways,
and controlling the movement of passengers to
ensure their safety. During the
Bright Field
emergency, however, several nonoperating
crewmembers experienced difficulty in
performing their duties. For example, when the
first mate directed the crewmembers to go to
their mooring stations during the evacuation of
the
Queen of New Orleans
, the vessel’s director
of security did not understand or appreciate the
implications of this announcement. Also,
nonoperating crewmembers did not distribute
life jackets to passengers aboard the
Creole
Queen
during the emergency.
Drills held aboard the
Queen of New
Orleans
had not simulated an evacuation while
moored. Moreover, the drills and training
sessions that were held involved only
supervisory gaming staff, who were expected to
inform other gaming staff crewmembers of their
content. No formal methods were used to verify
whether the nonoperating crewmembers were
advised of the content of the safety meetings or
the nature of drills performed. Unless it requires
accountability for the flow of safety information
from supervisory gaming staff to the rest of the
nonoperating staff, management cannot ensure
that the latter receive safety information that
could be critical in an emergency. The Safety
Board concludes that nonoperating crewmem-

66
bers of the
Queen of New Orleans
and the
Creole Queen
had not received training covering
the full range of emergency scenarios and were
unprepared to properly carry out their
responsibilities in this accident.
As a result of its investigation of a 1994 fire
aboard the small passenger vessel
Argo
Commodore
,
43
the Safety Board issued the
following recommendation to the Passenger
Vessel Association (PVA):
Develop and provide to your members
crew drills for on-board crew emer-
gency procedures/standards that include
preincident planning for a variety of
shipboard emergencies, including fires,
and the deployment of crew resources
for proper response to the emergency
without compromising passenger safety.
(M-95-43)
This recommendation was later placed on
the Safety Board’s list of Most Wanted Safety
Improvements. In 1997, the PVA made available
to the Safety Board its recently published
Training Manual for Passenger Vessel Safety
,
which incorporates a “Non-marine Crew Train-
ing” section that outlines a comprehensive
training program for nonoperating crewmem-
bers. The introduction to this section states that
specialized safety training for nonoperating
employees “makes sense when management
realizes that, more often than not, [these
employees] will be the first person[s] on the
scene in any kind of emergency.”
Based on the PVA’s support for the concept
of comprehensive training for nonoperating
employees and its development of the training
manual, the Safety Board classified Safety
Recommendation M-95-43 “Closed--Acceptable
Action.” The Safety Board notes that New
Orleans Paddlewheels, Inc., which is a PVA
member, has apparently not yet implemented
the training program for nonoperating
crewmembers set forth by the PVA in its
training manual. The Safety Board believes that
New Orleans Paddlewheels, Inc., should, in
43
Marine Accident Report--
Fire Aboard U.S. Small
Passenger Vessel
Argo Commodore
in San Francisco Bay,
California, December 3, 1994 (
NTSB/MAR-95/03).
accordance with the guidance published by the
PVA, require that nonoperating crewmembers
on all its vessels participate in formal
emergency training and drills in the proper
handling of emergencies that have the potential
to affect the persons in their charge. The
company should also maintain written records to
verify nonoperating crew proficiency levels and
skill retention.
Safety Briefings and Signage
-- According
to the vessel master, when the
Queen of New
Orleans
was to remain moored, he did not make
any safety announcements because he believed
the vessel was an extension of the dock when
not underway. The
Queen of New Orleans
broadcast a vessel safety videotape throughout
the vessel’s queuing area; however, a significant
number of passengers on board the vessel on the
day of the accident, some of whom had been on
the vessel several times before, did not recall
ever having seen or heard the safety broadcast.
Because the scheduled cruise had been canceled
owing to the high river stage, no safety briefings
were provided prior to the
Bright Field
accident.
However, the master stated that he had
instructed the engineer to start the engines to
prepare for leaving the dock to avoid being
struck by the
Bright Field
. Had the vessel left
the dock, the master probably would not have
had time to provide passengers with such basic
instructions as the location of life jackets.
The Safety Board concludes that the lack of
effective recurring safety briefings for
occupants of the
Queen of New Orleans
regarding emergency and evacuation procedures
may have contributed to the confusion and panic
reported among passengers and crew during the
vessel evacuation. The Safety Board believes
that New Orleans Paddlewheels, Inc., should
review the existing methods of providing safety
information to boarding passengers and make
the necessary improvements to ensure that all
vessel occupants receive recurring safety
briefings, regardless of whether the vessel is
scheduled to leave the dock.
Emergency instruction placards and sign
aboard the
Queen of New Orleans
were not
conspicuously displayed and were not readily
visible during the emergency. The safety
instructions, printed on plain white paper with
clear laminate, were subject to destruction in an

67
emergency such as that involving fire.
Moreover, the paper on which the instructions
were printed was similar to the color of the
walls upon which they were affixed, negating
their effectiveness in an emergency
characterized by haste, panic, or reduced
visibility. According to a number of the vessel’s
passengers on the day of the accident, they did
not see emergency instruction signage or egress
diagrams.
The Safety Board concludes that the
instruction placards and signage aboard the
Queen of New Orleans
were ineffective in
disseminating emergency instructions and vessel
information to passengers. The Safety Board
therefore believes that New Orleans
Paddlewheels, Inc., should post, on all its
vessels, emergency instructions that are printed
on fire- and heat-resistant material and that are
clearly visible to all passengers both under
normal conditions and during emergencies when
lighting and visibility may be diminished.
Shoreside Emergency Alert and
Response
-- Under River Front Alert Network
procedures established after this accident,
individual riverfront commercial properties
were to make their own determinations about
the proper actions to be taken after receiving
notification of an emergency involving a vessel
on the river. According to evacuation plans that
were initially in effect for property tenants, a
lengthy procedural chain of command was in
place that could delay a decision to evacuate. In
the view of the Safety Board, such a potential
for delay could endanger the employees and
patrons of riverfront properties. Therefore, on
September 5, 1997, the Safety Board issued the
following safety recommendation to the New
Orleans Dock Board:
Develop, as part of the River Front Alert
Network, an emergency evacuation
announcement for broadcast by the
harbor police department dispatcher
using a public address system linked to
river front properties that provides for a
timely and efficient evacuation in the
event of an impending collision or other
emergency. (M-97-60)
Documentation received by the Safety
Board on November 3, 1997, outlining the
actions to be taken in the event of the activation
of the River Front Alert Network appears to
address the Safety Board concerns that
prompted the issuance of Safety
Recommendation M-97-60. Under the specific
evacuation protocols developed for responding
to the activation of the River Front Alert
Network, the procedural chains of command
within each property’s evacuation plans have
been eliminated, and property security officers
have been given authority to initiate an
evacuation immediately upon hearing a River
Front Alert Network broadcast and assessing the
danger. Because these revised evacuation plans
meet the intent of the safety recommendation,
the Safety Board classifies Safety
Recommendation M-97-60 “Closed--Acceptable
Action.”
The River Front Alert Network system did
not require that vessels docked or moored in its
vicinity monitor the alert broadcast from the
Coast Guard traffic light operator to the harbor
police dispatcher indicating a vessel irregularity
or loss of steering in the vicinity of the
riverfront properties. The Safety Board was
concerned that, unless these vessels monitored
the network for emergency broadcasts, vessel
occupants would be subject to delays in
notification similar to those that occurred in this
accident and that contributed to the disorderly
evacuation and numerous injuries. Therefore, on
September 5, 1997, the Safety Board issued the
following safety recommendation to the New
Orleans Dock Board:
Require all vessels which dock or moor
in the area encompassed by the River
Front Alert Network to monitor the
River Front Alert Network radio for any
emergency broadcast to provide maxi-
mum advance notice of an emergency.
(M-97-61)
In a September 15, 1997, reply to the Safety
Board, the Dock Board said that the intent of
this safety recommendation should be met by
the postaccident COTP order requiring that all
large passenger vessels docked in the area have
a manned pilothouse and that they monitor all
emergency and working marine channels. While
agreeing that monitoring working and
emergency radio channels should give moored
passenger vessels advance warning of

68
potentially hazardous situations on the river, the
Safety Board noted that the COTP order
requiring such monitoring was an interim, and
possibly temporary, measure. The Coast Guard
has since published an interim rule that, when
issued as a final rule, will make permanent the
COTP order. In anticipation that the interim rule
regarding manned pilothouses and radio
monitoring will become permanent as 33 CFR
165.810(e), the Safety Board classifies Safety
Recommendation M-97-61 “Closed--No Longer
Applicable.”
Also on September 5, 1997, the Safety
Board issued the following safety recommenda-
tion to the Coast Guard:
Require that all commercial vessels that
operate within the River Front Alert
Network zone participate in the network
and notify the U.S. Coast Guard traffic
light operator whenever they experience
an irregularity or abnormality that could
result in a safety risk to the Port of New
Orleans area. (M-97-58)
In its November 18, 1997, letter to the
Safety Board, the Coast Guard stated that
existing regulations and local marine practice
are now serving to meet the intent of this safety
recommendation. The letter stated that,
[Title] 33 CFR 160.215 requires vessels
to immediately notify the nearest
Marine Safety Office or Group of
hazardous conditions aboard or caused
by the vessel. Currently, the vessels in
the vicinity of the traffic light notify the
traffic light operator who is responsible
to the Marine Safety Office. Through 33
CFR 26.03 or existing Captain of the
Port orders, ALL vessels, including
moored passenger vessels, must monitor
Channel 67 VHF. Therefore, when a
hazardous condition is reported to the
traffic light operator, he activates the
Riverfront Alert Network by calling the
Harbor Police on the Network radio.
The police then notify the impacted
participating facilities and vessels.
Between the Channel 67 notifications
and subsequent Riverfront Alert
Network radio calls, ALL vessels and
facilities are notified.
Based on this response, the Safety Board
classifies Safety Recommendation M-97-58
“Closed--Acceptable Action.”
Toxicological Testing
Two Coast Guard regulations (33 CFR Part
95 and 46 CFR Part 4) require that postaccident
alcohol tests be conducted on the pilot and
Bright Field
crewmembers directly involved in
this accident. Those regulations specify that
marine employers or their representatives are to
ensure that urine specimens (for drug testing)
and breath or blood specimens (for alcohol
testing) are obtained as soon as is practicable
following an accident.
In this case, the self-employed pilot supplied
both breath and urine specimens in a timely
manner. His specimens were negative for
alcohol and drugs.
Bright Field
crewmembers
also supplied breath and urine specimens, and
the results were negative.
44
The Safety Board is
concerned, however, that breath testing, which
is a time-sensitive procedure, was not conducted
in a timely fashion on some
Bright Field
personnel and, in fact, was conducted too late to
have any practical value. Because of the rate at
which humans metabolize alcohol,
45
evidence of
alcohol consumption is usually eliminated from
the body in about 8 hours. For example, an
individual could be legally intoxicated (0.10
percent BAC) at the time of an accident and
have a 0.00 percent BAC about 8 hours later.
Consequently, to produce meaningful results,
testing should occur within that time span.
In this case, tests of the master, chief
engineer, and helmsman were conducted
between 7 hours and 57 minutes and 8 hours and
30 minutes after the accident. Given that amount
of time, it cannot be clearly determined through
these tests whether alcohol had a role in this
accident, although no other information
suggested that alcohol was a factor. On the
contrary, the first Coast Guard investigator
aboard observed the crew by sight, sound, and
44
The results of the alcohol tests on the pilot and nine
crew members showed .000 percent BAC.
45
The elimination rate ranges between about .015
percent and .020 percent per hour.

69
smell for signs of alcohol or other impairment
and found none.
Postaccident testing could have begun
sooner. The ship’s agent learned of the accident
1 hour and 20 minutes after it occurred, and he
and the ship’s attorney were aboard in about 2
1/2 hours. The first Coast Guard investigator
went aboard 2 hours after the accident, and an
hour later (3 hours after the accident), he
ordered the ship’s attorney to have the crew
tested. Either of them could have facilitated
initiation of the testing process. Instead, the
ship’s agent general manager came aboard 3 1/2
hours after the allision and was there for another
hour before he arranged for testing. Tests were
not started sooner because the general manager
erroneously thought the Coast Guard would
make the arrangements. Further delay was
incurred in locating someone to conduct the
tests, which finally began 6 1/2 hours after the
accident. Each of these delays diminished the
value of the tests. Further, by conducting the
breath tests of the helmsman, master, and chief
engineer last, 8 hours or more after the accident,
the value of those tests was essentially negated.
Besides arranging for the testing, the agent
had to decide whom to test. The regulations
state that he should do so by determining who
was directly involved in the incident. The ship
agent’s decision was to test all crewmembers
assigned to the noon watch, which was on duty
at the time of the allision. However, the ship’s
carpenter, who was acting as the anchor watch,
was not tested. He was apparently inadvertently
overlooked for testing because he was not
regularly assigned to the noon watch. Since no
testing of the carpenter was done, no definitive
conclusions can be made about drugs or alcohol
with respect to his activities, though as with the
other crewmembers, no information was
obtained that would suggest that either had a
role.
Arrangements for and timing of the alcohol
testing illustrate several problems. For example,
the Coast Guard investigator was fully aware of
the agent’s responsibilities, but the agent was
not. Time was lost until the agent became fully
aware. Additional time was lost while a
qualified tester was contacted and brought
aboard. Also, the regulations themselves do not
adequately address the physiological need to
conduct alcohol testing within 8 hours if the
results are to be meaningful.
The Safety Board has observed these same
problems in previous accidents, and several
potential solutions exist. One recent accident
involved the vessel
Julie N
, which struck a
bridge support in Portland, Maine, on December
4, 1996. Because the problems and solutions
associated with the timing of postaccident drug
and alcohol testing were explored in a March
13-15, 1997, public hearing on that accident and
will be comprehensively addressed in the Safety
Board’s upcoming
Julie N
accident report, they
are not further discussed here.
Risk Assessment and Risk Management
This accident demonstrates that the many
and diverse stakeholders in the area of the Port
of New Orleans, including the Coast Guard, the
State of Louisiana, the Dock Board, the pilot
organizations, and the owners and operators of
riverfront properties and nearby moored
passenger ships, did not adequately prepare for
or mitigate the risk of a marine casualty
affecting people and property within the Port of
New Orleans. Some of the stakeholders, most
notably the Dock Board, had commissioned
partial risk assessment studies at various times
for the assets in the harbor area. Despite their
limitations (in either geography or scope), these
studies did provide adequate information for the
stakeholders to recognize the possibility of an
accident similar to the one involving the
Bright
Field
.
For example, risk assessment projects
predicted an increase in accidents involving
collisions, rammings, and groundings due to
increased river traffic. The Louisiana State
University risk assessment project, in 1994,
concluded that no sections of the Port of New
Orleans waterfront were free of ship allisions,
including the area where the high-capacity
passenger vessels, gaming vessels, and
riverfront properties were located. Analysis of
accident data for the Port of New Orleans from
1983 through 1993 (a total of 166 rammings
along the left descending bank between miles 91
and 101 AHP) identified a mooring area for
gaming vessels that had seen the fewest
“historical allisions on the left bank.” The study
acknowledged, however, that no area of the left

70
descending bank of the river had been
completely free of vessel strikes during the 11-
year period studied.
Port stakeholders did take risk management
initiatives such as providing barriers and
controls for some of their assets. At the time of
the planning for the Louisiana world’s fair in the
early 1980s, a proposal was made to tie up
barges (exhibit pavilions with large numbers of
patrons or visitors) along the riverfront fair site
at the location now occupied by the Riverwalk
Marketplace. The Dock Board rejected the plan.
The Audubon Institute, as a result of a
preconstruction risk assessment in 1987,
decided to construct the Aquarium of the
Americas some 100 feet behind the levee so that
it would be safe from vessel strikes. More
recently, the mooring areas for the gaming,
excursion, and ferry vessels were silted in to
possibly protect these vessels from ramming by
other ships.
Despite this history of some sensitivity to
risk within the port area, the Riverwalk
complex, including the condominium garage
and the Hilton Hotel Riverside, were
constructed on old warehouse piers on the river
side of the levee. This location offered no
“crush zone” that could absorb the impact of a
marine ramming, and despite the fact that the
piers themselves were not built to withstand
being struck by a heavy vessel, no physical
barriers were constructed outboard of the new
buildings to offer them protection. According to
the IRC, during the time when the IRC was
negotiating a lease with the Dock Board, the
Dock Board advised the IRC that vessels had
had allisions with wharves within the Port of
New Orleans, but no allisions had occurred at
the Lower Poydras Street wharf. The IRC
representatives were shown photographs of the
allisions at other wharves, but these photographs
depicted only minimal damage. The IRC
apparently did no further risk assessment, and
neither the initial construction of the mall nor
the initial construction of the riverside portion
of the Hilton Hotel resulted in any new structure
extending farther into the Mississippi River.
Rather, these structures were built entirely on
top of existing wharves.
In contrast, the 1987 Audubon Institute-
sponsored risk assessment similarly determined
that there had been few allisions at the Bienville
Street wharf and that because it is high up in the
bend, it faced low risk of being struck by an
outbound vessel. Nonetheless, recognizing low
incidence, but a potential for high consequences,
the Audubon Institute placed the Aquarium of
the Americas behind the levee with a 100-foot
buffer zone to protect the shoreside structure.
No similar safety feature was considered or
constructed for the Hilton Hotel or the
Riverwalk Marketplace.
The IRC obtained construction permits for
the riverside expansion of the hotel from the city
of New Orleans, the Corps of Engineers, and the
New Orleans Levee Board. In addition, the
construction plans were approved by the Dock
Board. According to the Dock Board, it may
make recommendations to the IRC or other
stakeholders in the area to widen the wharf, to
allow silt to accumulate, or to further increase
the robustness of construction in the area
immediately outbound of their structures;
however, it has no authority to compel such
action. Currently, the damaged portions of the
Riverwalk Marketplace mall, the parking deck,
and the Hilton Hotel are being rebuilt in the
same location. No physical barriers have been
included in the rebuilding of these facilities. As
with the initial construction, all permits were
granted, and all plans were approved.
Given the hazardous operating environment
in the Port of New Orleans and the number of
instances of loss of propulsion and steering, any
number of which could have resulted in similar
accidents or far more serious ones, the Safety
Board does not understand the property owners’
reluctance to provide adequate barriers to
protect their assets in the port area. Although the
River Front Alert Network is a commendable
effort to alert the harbor police and security
officers in the event of a need to evacuate the
area, such efforts are unlikely to result in a
complete evacuation under even slightly
different circumstances. For example, the
Bright
Field
rammed the Hilton Hotel during daylight
hours when, fortunately, few guests were
occupying rooms and no cleaning personnel
were in the immediate area. Had this accident
occurred during the evening, at night, or in the
morning hours, most of the rooms would
probably have been occupied. It is unlikely that
even the River Front Alert Network would have

71
been able to awaken the sleeping guests, alert
them to the danger, and evacuate them in time to
prevent serious injury or possible death.
The Safety Board is concerned that, despite
the historical record of marine incidents and
accidents in that section of the Mississippi
River, the Dock Board permitted the placement
of a commercial facility within about 20 feet of
an unprotected wharf. More than 13,500 people
a day visit the Riverwalk Marketplace. Those
visitors have a reasonable expectation that the
Port of New Orleans will assert its responsibility
to protect their safety by exercising the power to
disapprove a building plan that does not
adequately account for a known risk. The Safety
Board concludes that the IRC and the Dock
Board did not conduct adequate risk assessment
nor perform adequate safety management
oversight to protect their properties and the
people that use them from an allision such as
that involving the
Bright Field
.
While the construction of a shopping mall
and a hotel in such a high-risk area was ill-
advised, the Safety Board recognizes that
economy and practicality argue against
attempting to correct the error by relocating
those facilities. Nonetheless, the
Bright Field
accident highlights the risk to shoreside
structures within the Port of New Orleans and
the need to consider that risk in the approval
process for future construction there. The Safety
Board believes that the Dock Board, as part of
the permit-approval process for new commercial
and residential development along the wharves
within its jurisdiction, should require that any
new construction of occupied space be sited
behind a buffer zone sufficient to protect
persons and property by safely absorbing the
impact should a vessel strike a wharf.
After this accident, the Dock Board, in
effect, identified a buffer zone for the Riverwalk
Marketplace. The Dock Board “encouraged” the
IRC to widen the Upper Poydras Street wharf by
50 feet. The company had already widened the
wharf by that amount in one area to
accommodate a gaming vessel, and the Dock
Board suggested that the remainder of the wharf
be extended as well. The Safety Board concurs
in this suggestion and believes that the IRC
should enhance the safety of the patrons and
employees of the Riverwalk complex by
immediately undertaking to widen, by a
minimum of 50 feet, that length of the Poydras
Street wharf that has not previously been
extended. Such an extension prior to this
accident would have added a “crush zone” that
would probably have prevented the structural
damage and threat to persons that resulted from
the
Bright Field
accident.
Several passenger vessels, including
gaming, tour, and cruise vessels, were allowed
to dock along the left descending bank, the side
of the river at highest risk. Had the
Bright Field
lost power some time later and the same
accident scenario evolved, the ship would likely
have rammed the gambling vessel, resulting in
substantial loss of life. The cruise vessels, which
had even less warning time, would quite likely
also have sustained serious passenger injuries or
loss of life.
While silting around the vessels’ docking
areas may offer some protection from ramming
by deep-draft vessels at average river stages, the
silt layer did not reduce water depth sufficiently
to retard a runaway ship when the river was
high, as it was on the day of the
Bright Field
accident, nor did it protect the moored vessels
from ramming by shallow-draft vessels such as
tows and barges. The Safety Board is not aware
of any engineering evaluations conducted to
assess the effectiveness of the silting efforts.
The property owners and other stakeholders
within the Port of New Orleans clearly had the
responsibility to establish and maintain a
reasonable level of safety in the port area. The
Safety Board concludes that the Coast Guard,
the Dock Board, and the property owners did
not adequately address the risks posed to
moored vessels along the Erato, Julia, Poydras,
and Canal Street wharves; as a result, under
certain conditions, those vessels were vulnerable
to ramming by other marine traffic. The Safety
Board believes that the Coast Guard and the
Dock Board should reassess the risk of locating
passenger vessels along the left descending bank
of the Mississippi River and determine whether
to remove the vessels to a less vulnerable
location or put in place procedural, operational,
or physical barriers that will protect them from
ramming by riverborne traffic.

72
Additionally, no tugboats were used either
as escorts or as a “barrier” to prevent a runaway
ship from ramming the shore or colliding with
another marine asset. And no environmental
controls, such as the Corps of Engineers’
opening of the Bonnet Carré Spillway, were put
in place to reduce river flow or current.
On the river itself, the
Bright Field
was
operating at full speed in high-river and high-
current conditions. Apparently, neither the pilot
nor crew considered procedures that might be
employed to maximize the time available to
respond to an emergency. For example, the main
engines were being operated in bridge control,
and although this may have created a time
penalty in responding to an emergency, the pilot
and bridge crew did not discuss engine control
location prior to commencing the trip
downriver. In his testimony, the pilot claimed
that it was necessary to operate the
Bright Field
at maximum speed to attain reasonable
maneuverability of the vessel in the operating
environment of high water, rapid current, and a
heavily laden ship designed to be maneuverable
at lower speeds.
Several days after the accident, Safety
Board investigators boarded a fully loaded
vessel of similar size, displacement, and power
to the
Bright Field
that was operating
downbound in similar high water conditions.
During this transit, the pilot did not use full
speed to maneuver the ship. Each ship handles
differently, but the operation of the
Bright Field
at full speed left no margin for error. For
example, the main engine tripped off line
because of a temporary loss of lubricating oil
pressure. The oil pressure and engine operation
were restored within about 2 minutes, which is a
reasonable amount of time. However, operating
at full speed in high-river conditions, the ship
had no room to maneuver out of the emergency.
The Safety Board concludes that operating a
vessel at full speed in the restricted waters of the
Mississippi River may not allow sufficient time
or distance to recover from an emergency. The
Safety Board believes that the Coast Guard
should take the lead in working with the pilot
associations serving the Port of New Orleans to
evaluate the impact of operating vessels at full
speed in the Mississippi River and incorporate
that information in its risk-management and
risk-reduction strategies for the port area.
High-river conditions are repeatedly cited as
cause for concern. For example, various port
risk assessments cite local experts, in interviews
and in response to questionnaires, clearly
expressing that high river stage is an important
factor in river casualties. This opinion is
strongly supported by available data. Eleven
years of casualty data from the Port of New
Orleans and the Coast Guard clearly show a
seasonal trend to river casualties. The high
water months of February, March, April, and
May experience two to three times the casualties
that occur during the low-water months of July
through October.
In addition, the studies point out that the
Coast Guard acknowledges the fast Mississippi
River current and low seasonal water
temperatures as creating a very hostile
environment. No matter how many Coast Guard,
State, local, and other resources respond to a
casualty involving a large number of persons in
the water, it would be difficult to rescue
everyone. The Coast Guard 1994 search and
rescue exercise lead to the conclusion that,
under adverse conditions, the Coast Guard could
expect to rescue and save only a small
percentage of the people in the water. This
finding should be unacceptable to the Coast
Guard and the Port of New Orleans, and the two
agencies should consider alternative means to
deal with this emergency. For example, prior to
the
Bright Field
accident, the Bonnet Carré
Spillway had only been opened seven times to
alleviate high water conditions, apparently
because of the cumbersome and lengthy tasks
necessary to do so. Nonetheless, the risks
associated with high water and rapid current
were considered “unusual” enough that in
March 1997, the spillway was opened for the
eighth time. The Port of New Orleans, the Coast
Guard, and the Corps of Engineers might
consider more aggressive use of the Bonnet
Carré Spillway to alleviate these high water
conditions and to deal with the safety issues
created by them. Further, if the major
impediment to opening the spillway is the time
and effort it takes to do so, it may be appropriate
for the Corps of Engineers to consider ways to
make the spillway more usable and to employ it
for risk mitigation as well as for flood control.
No practical physical barrier aboard ship
exists that will safely stop a runaway vessel. In

73
such an emergency, a safe outcome depends on
the successful interaction of several physical
and operational factors. For example, if main
engine power is lost, adequate steering can
usually be maintained until the ship slows
enough for the anchors to be dropped. If a vessel
loses its steering, engine power can be used to
either slow the vessel (astern power) or, if it is a
twin-screw vessel, to maneuver the ship.
Anchors are perceived as providing some
level of protection by serving as “brakes” that
will stop or at least slow a ship. But anchors are
neither designed nor adequate for stopping a
heavily loaded ship traveling at high speed. Had
the
Bright Field’
s anchors been released, the
anchor chain would quite likely have payed out
at a speed that could not be controlled by the
windlass brake, and the chain would simply
have continued to run out until it parted from
the ship. In this accident, the dropping of the
anchor and paying out of chain could not have
been expected to significantly slow, let alone
stop, the ship.
Since this accident, the Coast Guard has
placed renewed emphasis on having anchors at
the ready (backed out of the hawsepipe,
disengaged from the windlass, and being held by
the brake), with a two-person forecastle watch.
While having the anchors manned and at the
ready may prove beneficial in certain
circumstances, it is unlikely to achieve anything
meaningful aboard a heavy vessel operating at
relatively high speeds in the Mississippi River.
Further, “increased emphasis” on having the
anchors at the ready may even provide a false
sense of security without effectively addressing
the dangers inherent in operating heavy vessels
at high speed in proximity to shoreside
businesses and passenger vessels.
The notable characteristic of all previous
risk assessment studies commissioned by the
Coast Guard or the Dock Board was their
limited scope. Most were conducted in light of
specific proposals, such as the addition of
gaming vessels to the port. Investigators
determined that no comprehensive study has
been done that considers all types of risks to all
port properties and people. The Safety Board
concludes that the stakeholders within the Port
of New Orleans, including Federal, State, and
local agencies; private commercial entities;
shipowners; and pilot associations have not
determined the overall level of risk associated
with the full range of activities within the port
area and have not provided adequate protection
for persons and property in that area.
The Coast Guard has overall responsibility
for maintaining public safety in the Port of New
Orleans area. Under the
Ports and Waterways
Safety Act of 1972
, the Congress charged the
Coast Guard with monitoring and managing risk
in all U.S. ports and taking actions to maintain
risk at an acceptable level. In carrying out this
role, the Coast Guard must assess and manage
the risk that is inherent in all commercial
activities within U.S. ports. In fact, in its
1996
Performance Report
, the Coast Guard’s Office
of Marine Safety and Environmental Protection
asserts that managing risk is its primary mission.
The Safety Board concurs with this assessment
and notes that the Coast Guard has the authority,
the responsibility, and the experience to direct a
comprehensive assessment of risk in the Port of
New Orleans.
The Safety Board believes that the Coast
Guard, with the cooperation of all stakeholders
within the Port of New Orleans, should conduct
a comprehensive risk assessment that considers
all activities, marine and shoreside, within the
port area. In addition to those risk factors
discussed earlier, this assessment should
consider the risks to people and property,
including shoreside businesses and passenger
vessels, that are associated with relatively high-
speed navigation of the river, high river stage
and rapid river current, railroad and highway
bridges spanning the waterway,
46
and the
carriage of cargoes such as bulk oil or other
hazardous materials or chemicals that can cause
pollution, fire, or explosion.
The Safety Board notes that many of the
risk factors associated with river commerce
within the port area have already been identified
in previous risk assessment studies and, further,
that these factors may be amenable to known
risk-reduction or risk-mitigation initiatives.
46
For more information, see Highway-Marine
Accident Report--
U.S. Towboat
Chris
Collision
with the
Judge William Seeber Bridge, New Orleans, Louisiana,
May 28, 1993
(NTSB/HAR-94/03).

74
Such initiatives might include reducing vessel
speed, opening the Bonnet Carré Spillway on a
more regular basis, using tugboats either as
escorts or as a “barrier” to protect marine assets,
adequately assessing the protection afforded by
silting-in of vulnerable areas, and moving the
passenger vessels to a safer location. The Safety
Board believes that the Coast Guard should, in
cooperation with the appropriate stakeholders,
including Federal, State, and local agencies;
private commercial entities; shipowners; and
pilot associations, implement risk-management
and risk-mitigation initiatives that will ensure
the safety of people and property within the Port
of New Orleans. The Safety Board further
believes that the Corps of Engineers, the State
of Louisiana, the Dock Board, the IRC
(including the New Orleans Hilton Riverside
Hotel), New Orleans Paddlewheels, Inc., the
New Orleans Baton Rouge Steamship Pilots
Association, the Crescent River Port Pilots
Association, and Associated Federal Pilots and
Docking Masters of Louisiana, Inc., should
participate with other stakeholders in instituting
risk management and mitigation initiatives that
will ensure the safety of people and property
within the Port of New Orleans.

75
Findings
1.
The following factors were not causal or
contributory to the accident involving the
Bright Field
: weather, fatigue, malfunc-
tioning of either the vessel’s steering gear or
equipment on the bridge, alcohol or other
drugs, crew health, crew qualifications, or
crew experience.
2.
The
Bright Field
showed evidence of
recurring engineering problems that affected
vessel main engine reliability, and had all
engineering systems been kept in good
repair and regularly tested, the vessel may
not have unexpectedly lost power during its
voyage down the Mississippi River.
3.
The
Bright Field
owners’ oversight of
testing and maintenance of the vessel’s
engineering systems was inadequate and led
to unreliable performance of the engineering
plant and contributed to the shutdown of the
main propulsion engine on the day of the
accident.
4.
Insufficient information was available to
determine whether any actions taken by the
pilot and crew of the
Bright Field
would
have been effective in preventing the
allision or mitigating its effects.
5.
At several points prior to and during the
Bright Field
emergency, the pilot, master,
and crew of the vessel did not exchange
information that under other circumstances
could have prevented or at least mitigated
the effects of the accident.
6.
Use of bridge resource management
precepts on board the
Bright Field
would
have enhanced the exchange of information
and the coordination of actions among the
pilot, master, and crew during the accident
sequence.
7.
The response to the
Bright Field
accident by
local emergency response agencies was
timely and appropriate.
8.
Evacuation of the
Queen of New Orleans
was hampered, and passenger risk increased,
by the fact that only one gangway was made
available for passenger egress during the
emergency.
9.
Nonoperating crewmembers of the
Queen of
New Orleans
and the
Creole Queen
had not
received training covering the full range of
emergency scenarios and were unprepared
to properly carry out their responsibilities in
this accident.
10.
The lack of effective recurring safety brief-
ings for occupants of the
Queen of New
Orleans
regarding emergency and evacua-
tion procedures may have contributed to the
confusion and panic reported among pas-
sengers and crew during the vessel
evacuation.
11.
The instruction placards and signage aboard
the
Queen of New Orleans
were ineffective
in disseminating emergency instructions and
vessel information to passengers.
12.
The International RiverCenter and the
Board of Commissioners of the Port of New
Orleans did not conduct adequate risk
assessment nor perform adequate safety
management oversight to protect their
properties and the people that use them from
an allision such as that involving the
Bright
Field
.
13.
The U.S. Coast Guard, the Board of
Commissioners of the Port of New Orleans,
and the property owners did not adequately
address the risks posed to moored vessels
along the Erato, Julia, Poydras, and Canal
Street wharves; as a result, under certain
CONCLUSIONS

76
conditions, those vessels were vulnerable to
ramming by other marine traffic.
14.
Operating a vessel at full speed in the
restricted waters of the Mississippi River
may not allow sufficient time or distance to
recover from an emergency.
15.
The stakeholders within the Port of New
Orleans, including Federal, State, and local
agencies; private commercial entities;
shipowners, and pilot associations have not
determined the overall level of risk
associated with the full range of activities
within the port area and have not provided
adequate protection for persons and
property in that area.
Probable Cause
The National Transportation Safety Board
determines that the probable cause of this
accident was the failure of Clearsky Shipping
Company to adequately manage and oversee the
maintenance of the engineering plant aboard the
Bright Field
, with the result that the vessel
temporarily lost power while navigating a high-
risk area of the Mississippi River. Contributing
to the amount of property damage and the
number and types of injuries sustained during
the accident was the failure of the U.S. Coast
Guard, the Board of Commissioners of the Port
of New Orleans, and International RiverCenter
to adequately assess, manage, or mitigate the
risks associated with locating unprotected
commercial enterprises in areas vulnerable to
vessel strikes.

77
As a result of its investigation of this
accident, and in addition to the safety
recommendations issued previously to the U.S.
Coast Guard, to the Board of Commissioners of
the Port of New Orleans, and to New Orleans
Paddlewheels, Inc., the National Transportation
Safety Board makes the following safety
recommendations:
--to the U.S. Coast Guard:
In cooperation with the Board of
Commissioners of the Port of New
Orleans, reassess the risk of locating
passenger vessels along the left
descending bank of the Mississippi
River and determine whether to remove
the vessels to a less vulnerable location
or put in place procedural, operational,
or physical barriers that will protect
these vessels from ramming by
riverborne traffic. (M-98-1)
Conduct, with the cooperation of all
stakeholders, a comprehensive risk
assessment that considers all activities,
marine and shoreside, within the Port of
New Orleans. (M-98-2)
Take the lead in working with the pilot
associations serving the Port of New
Orleans to evaluate the impact of
operating vessels at full speed in the
Mississippi River and incorporate that
information in your risk-management
and risk-reduction strategies for the port
area. (M-98-3)
In cooperation with the appropriate
stakeholders, including Federal, State,
and local agencies; private commercial
entities; shipowners; and pilot associa-
tions, implement risk-management and
risk-mitigation initiatives that will en-
sure the safety of people and property
within the Port of New Orleans.
(M-98-4)
--to the U.S. Army Corps of Engineers:
Participate with the U.S. Coast Guard
and other stakeholders in a comprehen-
sive risk assessment that considers all
activities, marine and shoreside, within
the Port of New Orleans. (M-98-5)
In cooperation with the appropriate
stakeholders, including Federal, State,
and local agencies; private commercial
entities; shipowners; and pilot associa-
tions, implement risk-management and
risk-mitigation initiatives that will en-
sure the safety of people and property
within the Port of New Orleans.
(M-98-6)
--to the State of Louisiana:
Participate with the U.S. Coast Guard
and other stakeholders in a comprehen-
sive risk assessment that considers all
activities, marine and shoreside, within
the Port of New Orleans. (M-98-7)
In cooperation with the appropriate
stakeholders, including Federal, State,
and local agencies; private commercial
entities; shipowners; and pilot associa-
tions, implement risk-management and
risk-mitigation initiatives that will en-
sure the safety of people and property
within the Port of New Orleans.
(M-98-8)
--to the Board of Commissioners of the Port
of New Orleans:
As part of the permit-approval process
for new commercial and residential
development along the wharves within
your jurisdiction, require that any new
construction of occupied space be sited
behind a buffer zone sufficient to
protect persons and property by safely
absorbing the impact should a vessel
strike the wharf. (M-98-9)
RECOMMENDATIONS

78
In cooperation with the U.S. Coast
Guard, reassess the risk of locating
passenger vessels along the left
descending bank of the Mississippi
River and determine whether to remove
the vessels to a less vulnerable location
or put in place procedural, operational,
or physical barriers that will protect
these vessels from ramming by
riverborne traffic. (M-98-10)
Participate with the U.S. Coast Guard
and other stakeholders in a comprehen-
sive risk assessment that considers all
activities, marine and shoreside, within
the Port of New Orleans. (M-98-11)
In cooperation with the appropriate
stakeholders, including Federal, State,
and local agencies; private commercial
entities; shipowners; and pilot associa-
tions, implement risk-management and
risk-mitigation initiatives that will en-
sure the safety of people and property
within the Port of New Orleans.
(M-98-12)
--to International RiverCenter:
As previously suggested by the Board of
Commissioners of the Port of New
Orleans, immediately enhance the safety
of the patrons and employees of the
Riverwalk complex by widening, by a
minimum of 50 feet, that length of the
Poydras Street wharf that has not
previously been extended. (M-98-13)
Participate with the U.S. Coast Guard
and other stakeholders in a comprehen-
sive risk assessment that considers all
activities, marine and shoreside, within
the Port of New Orleans. (M-98-14)
In cooperation with the appropriate
stakeholders, including Federal, State,
and local agencies; private commercial
entities; shipowners; and pilot associa-
tions, implement risk-management and
risk-mitigation initiatives that will en-
sure the safety of people and property
within the Port of New Orleans.
(M-98-15)
--to Clearsky Shipping Company:
Perform a baseline engineering assess-
ment of the
Bright Field’
s engineering
plant and correct all conditions not in
conformance with manufacturer’s speci-
fications. (M-98-16)
Institute an engineering testing, mainte-
nance, repair, and company oversight
program for the
Bright Field
that will
ensure safe and reliable operation of the
vessel’s engineering plant. (M-98-17)
Provide your bridge and engineroom
watchstanding officers and crewmem-
bers with initial and recurrent bridge
resource management training that in-
cludes communication and coordination
between pilots and members of the
bridge and engineroom watches and that
addresses their use of bridge and en-
gineroom systems. (M-98-18)
--to New Orleans Paddlewheels, Inc.:
In accordance with the guidance
published by the Passenger Vessel
Association, require that nonoperating
crewmembers on all your vessels
participate in formal emergency training
and drills in the proper handling of
emergencies that have the potential to
affect the persons in their charge.
Maintain written records to verify
nonoperating crew proficiency levels
and skill retention. (M-98-19)
Review the existing methods of
providing safety information to
boarding passengers and make the
necessary improvements to ensure that
all vessel occupants receive recurring
safety briefings, regardless of whether
the vessel is scheduled to leave the
dock. (M-98-20)
On all your vessels, post emergency
instructions that are printed on fire- and
heat-resistant material and that are
clearly visible to all passengers both
under normal conditions and during
emergencies when lighting and visibility
may be diminished. (M-98-21)

79
Participate with the U.S. Coast Guard
and other stakeholders in a comprehen-
sive risk assessment that considers all
activities, marine and shoreside, within
the Port of New Orleans. (M-98-22)
In cooperation with the appropriate
stakeholders, including Federal, State,
and local agencies; private commercial
entities; shipowners; and pilot associa-
tions, implement risk-management and
risk-mitigation initiatives that will en-
sure the safety of people and property
within the Port of New Orleans.
(M-98-23)
--to the New Orleans Baton Rouge
Steamship Pilots Association:
Encourage your members to participate
in initial and recurrent bridge resource
management training that teaches the
principles of resource management and
that emphasizes team coordination
between the pilot and crew. (M-98-24)
Participate with the U.S. Coast Guard
and other stakeholders in a comprehen-
sive risk assessment that considers all
activities, marine and shoreside, within
the Port of New Orleans. (M-98-25)
In cooperation with the appropriate
stakeholders, including Federal, State,
and local agencies; private commercial
entities; shipowners; and pilot associa-
tions, implement risk-management and
risk-mitigation initiatives that will en-
sure the safety of people and property
within the Port of New Orleans.
(M-98-26)
--to the Crescent River Port Pilots
Association:
Participate with the U.S. Coast Guard
and other stakeholders in a comprehen-
sive risk assessment that considers all
activities, marine and shoreside, within
the Port of New Orleans. (M-98-27)
In cooperation with the appropriate
stakeholders, including Federal, State,
and local agencies; private commercial
entities; shipowners; and pilot associa-
tions, implement risk-management and
risk-mitigation initiatives that will en-
sure the safety of people and property
within the Port of New Orleans.
(M-98-28)
--to Associated Federal Pilots and Docking
Masters of Louisiana, Inc.:
Participate with the U.S. Coast Guard
and other stakeholders in a comprehen-
sive risk assessment that considers all
activities, marine and shoreside, within
the Port of New Orleans. (M-98-29)
In cooperation with the appropriate
stakeholders, including Federal, State,
and local agencies; private commercial
entities; shipowners; and pilot associa-
tions, implement risk-management and
risk-mitigation initiatives that will en-
sure the safety of people and property
within the Port of New Orleans.
(M-98-30)

80
BY THE NATIONAL TRANSPORTATION SAFETY BOARD
JAMES E. HALL
Chairman
ROBERT T. FRANCIS II
Vice Chairman
JOHN A. HAMMERSCHMIDT
Member
JOHN J. GOGLIA
Member
GEORGE W. BLACK, JR.
Member
January 13, 1998

81
APPENDIX A
Investigation
The Safety Board learned of the accident involving the Bright Field about 1700 on
December 14, 1996. A five-person investigation team consisting of an investigator-in-
charge, an engineering specialist, an operations specialist, a human performance
specialist, and a survival factors specialist arrived on scene on December 15, 1996,
accompanied by representatives from the Safety Board’s Offices of General Counsel and
Public Affairs. Member Hammerschmidt was the Board Member on scene.
This accident was investigated jointly by the Safety Board and the U.S. Coast Guard
under the authority of section 304(a)(1)(E) of the Independent Safety Board Act of 1974 and
in accordance with 49 CFR 850, “Coast Guard-NTSB Marine Casualty Investigations.” The
Coast Guard invited the Government of Liberia to participate in the investigation, in
accordance with the IMO resolution A637, “Co-Operation in Maritime Casualty
Investigations.” The Government of Liberia accepted the invitation and a representative
participated fully in all aspects of the investigation.
Hearing / Deposition
The Safety Board did not conduct a public hearing in connection with this accident.
However the Safety Board was a participant in the U.S. Coast Guard Marine Board of
Investigation public hearings held in New Orleans, Louisiana, on December 17-21, 1996;
January 6-11 and 29-30, 1997; and March 19-20, 1997.

this page intentionally left blank

83
APPENDIX B
Chronology of
Bright Field
Engineering Problems
October 1995
25th Owner notes concern about continuing cracking problems on Sulzer RTA62 main engines
and attributes problem to design, material, manufacturer, operation and handling.
Provides specific instructions to masters and chief engineers about operation and
maintenance parameters.
January 1996
1st Chief engineer reports to owner about serious engineering problems on the Bright Field
including cracked main engine cylinder liners, and loss of power while transiting the
Panama Canal due to low main engine lubrication oil system pressure because of an
excessive pressure drop across the second filter.
February 1996
2nd Master telexes owner that he has to run at reduced rpms because of main engine
overheating problems and frequent “auto slowdowns”.
March 1996
Master telexes owner that engineering equipment malfunctions frequently due to the age
and condition.
April 1996
Bright Field dry docked in Nan Tung, China.
May 1996
20th Master telexes owner about severe damage to the main engine’s No. 2 cylinder and
piston. No spare parts available.

Appendix B—Cont.
84
June 1996
2nd Second engineer’s maintenance log reports repairs to the main engine’s No. 2 and 3
cylinder liners and pistons.
July 1996
5th 0900, arrived Long Beach, California.
23rd Anchored, Japan.
26th Renewed #2 piston, cylinder liner and rings to main engine.
August 1996
3rd Trouble with a pneumatic control valve 14B in automated propulsion pneumatic logic
control.
4th Removed #5 piston and cylinder liner to main engine, replaced cylinder liner.
5th Removed #4 cylinder liner and piston rings to main engine, replaced piston rings with
“used” rings.
6th 1500, departed for Indonesia.
16th 0440, arrived Pulau Laut, Indonesia.
18th 1245, departed Pulau Laut, Indonesia for Hong Kong.
26th Arrived Hong Kong. Owner’s representative boards vessel.
27th Repaired main engine pneumatic control valve 38A
28th 0005, departed Hong Kong
September 1996
2nd Arrived Banjarmasin, Borneo, Indonesia to load cargo of steaming coal.
3rd Renewed #1 cylinder liner and piston to main engine (liner cracked, piston head burnt and
dented).
5th Master informs owner must purchase fresh water, evaporator can only make 10 metric
tons, vessel consumes 15 metric tons daily.
6th Owner telexes Bright Field that main engine lubrication oil analysis shows low flash
point and high viscosity with possible fuel oil leakage into sump.
9th Ordered replacement parts for main engine fuel injection pump, cracked valve
12th Departed Banjarmasin, Indonesia, enroute Davant, Mississippi River (e.t.a. Oct 26th)
17th 0400, #4 piston rings seized and broken, running at reduced speed (65 rpms). Master
hopes to make Singapore for repairs. Chief engineer recommends lifting out #4 piston for
repairs.

Appendix B—Cont.
85
18th 0500, drifting while repairing rings to #4 piston, changed piston crown to #4 broken
piston crown bolts and no more spares. Also found water leakage in #4 cylinder by piston
crown damage. Discovered ring damage to #1, 2, 4, 5 pistons, found blocked holds where
cylinder oil is injected. #5 cylinder not working correctly, found cylinder liner cracks. Not
enough spare parts for piston ring and cylinder liner repairs, Master telexes owner,
“Serious trouble! Except for #1, all cylinder liners leaking gas. Not sure of safety”.
18th 0448, stopped main engine for repairs. Renewed #4 piston rings and piston crown.
Welded cracked in cylinder liner.
19th Rough seas main engine still under repair. Notes high level of impurity in main engine
and blockage of filters.
20th Master reports vessel in area of typhoon. Main engine damage is serious with no spare
parts available. Welded cracks in #5 cylinder liner. Replaced #4 cylinder liner with old
used liner (old #1). Engineering crew exhausted.
21st Dirty air cooler. Can not dismantle to clean because of sea conditions.
22nd 1600, completed temporary main engine repairs. #4 cylinder liner still leaking, running at
reduced rpms enroute Spore, Singapore for repairs main engine, air cooler e.t.a. 30 Sept.
25th High main engine scavenging temp due to malfunctioning sea water cooler and main
engine air cooler.
26th Repairs to both main high pressure air compressors.
28th Evaporator out of commission due to faulty pump.
29th Main engine slowdown.30th , 0700 arrived Spore, Singapore.
October 1996
1st Chief electrician tests some temp/pressure sensors.
2nd Telephone conversation between second engineer and owner concerning the quality of the
main engine’s lubrication oil. In telex to owner, master reports that the chief engineer has
increased main engine cylinder oil flow rate.
3rd Owner’s representative boards vessel and reports concern about poor operating condition
of Bright Field’s main engine and lack of confidence in chief engineer. Master telexes
repairs completed, enroute Devant, LA, via Suez Canal, e.t.a. 15 Nov
4th Urgent request for spare parts at Suez for high pressure air compressor, boiler fuel oil
burning pump, evaporator.
7th Revised e.t.a. Devant, LA, Nov 21th.
9th Mmaster requested permission to reduced main engine speed to 63 rpms due to high
exhaust gas temps and ‘overloads’. Reports continued cylinder cracking problems if
speed isn’t reduced.
10th Main engine temp problems due to air/electrical valve in speed control system. Chief
engineer overhauls 14A, 4B, and 7D pneumatic control valves.1st , renewed #1 piston
rings. Renewed #4 cylinder liner.

Appendix B—Cont.
86
11 Main engine fuel timing cannot be adjusted.
17th Response to owner message, can’t increase speed more.
21st 1400, arrived Suez Canal.
21st No. 2 & 3 cylinder leaking past piston rings and stuffing boxes. #2 piston found to have
dented head, planned to lift out #2 and #3 pistons to inspect/change damaged rings before
departure from Suez.
23rd Renewed #2 and #3 piston rings.
24th Main engine repairs completed. Ring damage attributed to poor quality of rings. main
engine cylinder oil consumption is 1.32 g/hp-h. Departed Port Said, e.t.a. Devant, LA is
Nov 16th.
28th Second engineer looking for tools to set main engine fuel oil injecting timing.
30th Main engine calibration tools found on board surveyed in response to owner request.
November 1996
4th Reduced rpm to 61 due to high exhaust gas temperatures (508C vs. alarm at 515C).
Request repair of CRT monitors and main engine fuel injection pump timing.
5th 2200, slow down caused by the high crank case oil mist alarm. Heavy smoke emitted
from main engine, repair work underway.
6th 1800, stopped main engine, found hole in #5 piston head cracked and leaking exhaust
gases through stuffing box into crank case, contaminating lube oil. Found #5 main engine
piston head burn through. Replaced with old used piston head. Engineering crew renews
main engine sump lubricating oil due to concern about low flash point of oil. Only
replaced 8.4 cubic meters of oil (all that was in storage). Owner informed main engine
sump was cleaned.
7th 2300 underway again running at reduced speed (61 rpms) due to high exhaust
temperatures.
8th Request for spare parts: 2 piston heads, piston rings, main engine fuel injection valve.
Request for 14 tons of main engine lubrication oil (no spare), 10 tons for storage and 4
tons to be added to the main engine sump. New e.t.a is Nov 20th.
12th Chief engineer notes that vessel does not have proper tools to set main engine fuel oil
pump timing correctly. Consulting instruction books. 1200 hours stopped to try to adjust
fuel pump timing based on instructions from owner. 1800 work completed underway
again.
13th New e.t.a. Nov 21st
14th Requesting 14,000 liters of main engine lube oil on arrival Davant. Auxiliary boiler FO
boost pump ooc (requested spare parts on August 27th ), no spare parts. Must use diesel
oil instead of bunker fuel oil every time main engine and G/Es are started and stopped.
14th Master requests main engine expert meet vessel to solve problems, no one on board
knows how to fix problems. Attempted to increase rpms from 61. At 63 turbocharger
inlet temp rose to 510 (alarm at 515C). Reduced speed to 61 rpms.

Appendix B—Cont.
87
15th Master notes last d/d 04-28-96 and last special survey 17-09-95.
20th Second engineer still looking for missing tool to set main engine fuel oil injector timing.
21st 0610 at sea buoy, set manned engine room. Chief engineer relieved of duty and replaced.
1630 along side Davant coal dock to off load coal.
21st Sulzer technical representative checks main engine. Identifies several sources of possible
lube oil contamination. Notes many serious problems with the main engine.
22nd Master reports results of Sulzer survey to owner.
24th Tested main engine emergency shut downs.
25th 0849 coal discharge completed, anchored Mississippi River to clean cargo holds.
25th Overhauled #2 main engine cylinder, new piston head.
26th Bunkering fuel oil and diesel oil.
27th Vessel fails cargo hold inspection. Engineering crew rebuilds main engine injector pumps
and set timing with help of Sulzer technical representative. Vessel receives approximately
8,000 liters of main engine lubrication oil.
28th Overhauled #5 main engine cylinder, replaced piston rings, found three small cracks in
liner.
30th Repaired defective main engine emergency stop valve.
December 1996
1st Master requests engineering spare parts. Notes status of repair work; #2 and #5 cylinders
cracked and piston rings worn (poor quality), cleaned stuffing boxes and scavenging air
boxes, air/water separator for air cooler and exhaust manifold, M/E fuel oil pump timing
with assistance of Sulzer, main engine emergency stop system repaired 3 control air
valves.
2nd Crew attempted unauthorized repair to Terasaki monitors.
5th Vessel passed hold inspection. Repaired main engine control air supply pressure reducers
(A-124HA,124HB).
7th Tested main engine with sea trial data and found continued high turbocharger inlet temps.
Recommended repairs to turbocharger and /or air cooler.
9th Chief engineer sends notice to owner confirming seriousness of engineering problems
observed by Sulzer technician. At 1200, along side Cargil (Reserve) grain loading facility
to load cargo.
11th Found turbocharger rotor rings worn. 1317 completed loading corn.
12th Renewed #5 cylinder piston rings. Chief engineer sends off main engine lube oil sample.
12th Anchored Mississippi River for repairs to turbocharger and air cooler by local
engineering repair service.
13th ETD December 14, 0800. Next port of call is Cristobal, Panama with an ETA of
December 19th at 1600.
14th 0700, engineering repairs completed, 0945, vessel underway from Reserve, sailed from

Appendix B—Cont.
88
anchorage at 1112, draft forward 11.96m, draft aft 12.06m., ETA Kashima, Japan on
January 18, 1997.
14th 1055 and 1110, main engine will not start in W/H control.
14th 1158 and 1235, main engine experiences overheating alarms/problems due to jacket water
cooling problems.
14th 1406, loss of main engine lube oil pressure. Failure of standby lube oil pump to start. Low
pressure alarm and main engine trip.

89
APPENDIX C
Voyage Data Recorders (VDRs)
The Safety Board has long considered that marine VDRs (also known as voyage event
recorders, or VERs), when used as management oversight tools, can provide valuable
information, not only on engineering plant performance, but on crew performance and training
needs. Use of a VDR to monitor crew performance can provide management with a means of
measuring training effectiveness and identifying needed changes in training or procedures. When
used as accident reconstruction tools, VDRs help investigators determine how an accident
occurred so that they can develop measures to help prevent similar accidents.
The Safety Board has promoted the use of VDRs of various types since the 1970s and is on
record in support of the value of these systems as management tools as well as accident
investigation tools. Safety Board staff has been extensively involved in aviation and surface
vehicle data recorder readout, data analysis, rulemaking, and technical standards development for
VDRs. The Safety Board has been working closely with the Coast Guard for more than 1 year in
an effort to develop International Maritime Organization (IMO) carriage requirements and
technical standards for VDRs.
The IMO’s Navigation Subcommittee has requested that the International
Electrotechnical Commission (IEC) develop an international technical testing standard for VDRs.
The standard will be based on the IMO recommendations. The IEC working group (TC-80/WG-
11) commenced work in March 1997 and expects to publish a standard in 1999. Representatives
from the Safety Board are working with the IEC group to develop the standard.
The IMO is expected to require the installation of VDRs on roll-on roll-off (RORO)
passenger ferries as early as 1998, followed by a requirement for VDRs on all vessels of more
than 1,600 gross tons within the next 4 to 5 years. While the Safety Board would prefer more
timely deployment of VDRs, it is encouraged that this significant issue is finally receiving
international attention and action.
