
2020 ALABAMA STATE HEALTH ASSESSMENT
1
2020
Alabama
State Health
Assessment

A
L
A
B
A
M
A
D
E
P
A
R
T
M
E
N
T
O
F
P
U
B
L
I
C
H
E
A
L
T
H
1875
EST.
Accredited Health Department
March 9, 2022
As State Health Ocer of Alabama, I am pleased to present the 2020 Alabama State Health
Assessment (SHA).
is assessment assists the Alabama Department of Public Health (ADPH) with
identifying strengths and areas of improvements for state distributed resources.
e 2020 SHA summary provides updates of 14 health indicators in Alabama, changes in
the state’s health since 2015, and information on resources available to address these concerns. e
14health indicators were identied through surveying government and local agencies, communi-
ty organizations and groups, healthcare providers and support professionals, and residents across
Alabama. e SHA also includes data on new, emerging health areas requested by partners.
e pandemic has been a challenging experience, but the heroic eorts remind us that
building and maintaining healthy communities requires a collaborative approach. ADPH will
continue to be a partner in developing solutions to many community issues. ADPH hopes that the
information in this SHA increases your awareness of the health issues in our state, your knowledge
of resources and programs that are available, and a drive to become involved in initiatives to create
the “Healthy People. Healthy Communities. Healthy Alabama” we envision.
e SHA is also an essential part to ADPH maintaining accreditation, and ADPH welcomes
your comments and feedback. For more information about ADPH and our services, please visit our
website at www.alabamapublichealth.gov.
Sincerely,
Scott Harris, M.D., M.P.H.
State Health Ocer

2020 ALABAMA STATE HEALTH ASSESSMENT
4
Table of Contents
Section I: Overview
Collaborative Development of the State Health Assessment.................................................................................................................... 6
Identifying the Leading Health Indicators ........................................................................................................................................................... 6
Advancements Made Since 2015 ........................................................................................................................................................................... 7
Alabama’s Economic and Demographic Data ..................................................................................................................................................8
Section II: Indicators
Health Indicator 1: Mental Health and Substance Abuse .............................................................................................................................13
1. Suicide Mortality ..........................................................................................................................................................................................13
2. Depression Diagnosis in Medicaid Recipients ................................................................................................................................ 14
3. Adults with Depression ............................................................................................................................................................................15
4. Depression Among Medicare Recipients ...........................................................................................................................................15
5. Schizophrenia Among Medicare Recipients .................................................................................................................................... 16
6. Mental Health Professional Shortage Areas ..................................................................................................................................... 16
7. Substance Abuse Diagnosis in Medicaid Recipients .....................................................................................................................17
8. Drug-related Overdose ............................................................................................................................................................................ 18
9. Drug Poisoning Mortality .......................................................................................................................................................................... 19
Health Indicator 2: Access to Care ........................................................................................................................................................................21
1. Percent of Alabamians with No Healthcare Coverage .................................................................................................................. 21
2. Rural Healthcare Facilities ......................................................................................................................................................................22
3. Households Without a Vehicle ............................................................................................................................................................. 22
4. Primary Care Health Professionals Shortage Areas ...................................................................................................................... 23
Health Indicator 3: Pregnancy Outcomes ........................................................................................................................................................25
1. Inadequate Prenatal Care .......................................................................................................................................................................25
2. Obstetrical Services in Alabama 1980-2019 ...................................................................................................................................26
3. Infant Mortality ...........................................................................................................................................................................................27
4. Low Birth Weight .........................................................................................................................................................................................27
5. Teen Pregnancy ...........................................................................................................................................................................................28
6. A Closer Look into Nutrition and Physical Activity .........................................................................................................................28
Health Indicator 4: Nutrition and Physical Activity .........................................................................................................................................31
1. Adults Classified as Obese ......................................................................................................................................................................31
2. Adults Consuming Vegetables Less Than Once Per Day ............................................................................................................ 32
3. Adults Consuming Fruits Less Than Once Per Day ......................................................................................................................32
4. Adults Who Participate in Physical Activities ..................................................................................................................................33
5. A Closer Look into Nutrition and Physical Activity .........................................................................................................................34
Health Indicator 5: Social Determinants of Health ....................................................................................................................................... 37
1. The Alabama Black Belt ...........................................................................................................................................................................37
2. Income Disparities .....................................................................................................................................................................................38
3. Education and Poverty ............................................................................................................................................................................38
4. Unemployment Rate .................................................................................................................................................................................39
5. Food Insecurity ...........................................................................................................................................................................................39
6. Housing Assistance ..................................................................................................................................................................................40
7. Family and Social Support .......................................................................................................................................................................41
8. Social Vulnerability Index .........................................................................................................................................................................41
Health Indicator 6: Sexually Transmitted Infections ....................................................................................................................................43
1. Syphilis Incidence ......................................................................................................................................................................................43
2. Gonorrhea Incidence ............................................................................................................................................................................... 44
3. Chlamydia Incidence .............................................................................................................................................................................. 44
4. Human Immunodeficiency Virus Incidence ....................................................................................................................................45
5. A Closer Look into Sexually Transmitted Infections .................................................................................................................... 46
Health Indicator 7: Geriatrics ................................................................................................................................................................................ 48
1. Adult Abuse Cases .................................................................................................................................................................................... 48
2. Alzheimer’s Disease Among Medicare Recipients ....................................................................................................................... 49
Health Indicator 8: Cardiovascular Diseases ....................................................................................................................................................51
1. Adults Ever Told They Have High Blood Pressure ...........................................................................................................................51
2. Hypertension Diagnosis in Medicaid Recipients ............................................................................................................................ 52

2020 ALABAMA STATE HEALTH ASSESSMENT
5
3. Hypertension Among Medicare Recipients ....................................................................................................................................53
4. Hyperlipidemia Among Medicare Recipients .................................................................................................................................. 53
5. Stroke Among Medicare Recipients ....................................................................................................................................................54
6. Blue Cross and Blue Shield Members with Cardiovascular Disease-related Claims .......................................................54
7. Heart Disease and Stroke Mortality.....................................................................................................................................................55
Health Indicator 9: Child Abuse/Neglect ........................................................................................................................................................... 57
1. Child Abuse Calls ........................................................................................................................................................................................57
2. Maltreatment Types of Child Victims ................................................................................................................................................. 58
Health Indicator 10: Environmental Health ...................................................................................................................................................... 59
1. Droughts and Hot Weather Hazards ...................................................................................................................................................59
2. Public Water Systems ...............................................................................................................................................................................60
3. Water Quality Lead Testing at Schools ...............................................................................................................................................60
Health Indicator 11: Violence ..................................................................................................................................................................................63
1. Violent Crimes .............................................................................................................................................................................................63
2. Violent Deaths .............................................................................................................................................................................................63
3. Firearm-related Deaths ...........................................................................................................................................................................64
Health Indicator 12: Cancer ....................................................................................................................................................................................66
1. Overall Cancer Mortality ..........................................................................................................................................................................66
2. Colorectal Cancer Incidence ................................................................................................................................................................. 67
3. Breast Cancer Incidence ........................................................................................................................................................................68
4. Lung and Bronchus Cancer Incidence ...............................................................................................................................................68
5. Prostate Cancer Incidence ..................................................................................................................................................................... 69
6. Cervical Cancer Incidence ...................................................................................................................................................................... 69
Health Indicator 13: Diabetes .................................................................................................................................................................................. 71
1. Adults Ever Told They Have Diabetes ..................................................................................................................................................71
2. Diabetes Among Medicare Recipients ............................................................................................................................................... 72
3. Diabetes Diagnosis in Medicaid Recipients ..................................................................................................................................... 72
4. Blue Cross and Blue Shield Members with Diabetes-related Claims ..................................................................................... 73
5. Diabetes Related Mortality ..................................................................................................................................................................... 74
Health Indicator 14: Tobacco Usage and Vaping ............................................................................................................................................ 75
1. Current Adult Cigarette Smokers ......................................................................................................................................................... 75
2. Adult Nicotine Product Use ....................................................................................................................................................................76
3. Current High School Student Smokers .............................................................................................................................................. 76
4. High School Students Vaping ................................................................................................................................................................. 77
Section III: Appendix
Detailed Alabama Economic and Demographic Data ................................................................................................................................80
Health Indicator 1: Mental Health and Substance Abuse Indicators by County ................................................................................ 82
Health Indicator 2: Access to Care Indicators by County ...........................................................................................................................84
Health Indicator 3: Pregnancy Outcomes Indicators by County ............................................................................................................. 86
Health Indicator 4: Nutrition and Physical Activity Indicators by County ............................................................................................88
Health Indicator 5: Social Determinants of Health Indicators by County ............................................................................................90
Health Indicator 6: Sexually Transmitted Infections Indicators by County .........................................................................................92
Health Indicator 7: Geriatrics Indicators by County .....................................................................................................................................94
Health Indicator 8: Cardiovascular Diseases Indicators by County ....................................................................................................... 95
Health Indicator 9: Child Abuse/Neglect Indicators by County ............................................................................................................... 97
Health Indicator 10: Environmental Health Indicators by County ..........................................................................................................98
Health Indicator 11: Violence Indicators by County ....................................................................................................................................... 99
Health Indicator 12: Cancer Indicators by County ........................................................................................................................................101
Health Indicator 13: Diabetes Indicators by County ...................................................................................................................................103
Health Indicator 14: Tobacco Usage and Vaping Indicators by County ...............................................................................................105
Alabama Department of Public Health Districts .......................................................................................................................................... 106
Alabama Community Health Issues Survey .................................................................................................................................................. 107
Acronym List ..............................................................................................................................................................................................................109
Data and Technical Notes ......................................................................................................................................................................................110
Acknowledgements ................................................................................................................................................................................................... 111

2020 ALABAMA STATE HEALTH ASSESSMENT
6
Collaborative Development of the
State Health Assessment
The Alabama (AL) Department of Public Health (ADPH)
seeks to promote, protect, and improve the health of all
individuals in AL. With the guidance of community partners,
ADPH sta developed a State Health Assessment (SHA).
This statewide report helps ADPH better understand local
communities’ concerns/needs and develop plans with
partners to address health outcomes.
The following section depicts how the ADPH SHA
workgroup collaborated with a team of University of AL
in Tuscaloosa members, complied survey results from
community partners, completed a literature review, and
reviewed the 2015 Community Health Assessment (CHA)
data to create the 2020 SHA.
Step 1: Sought the public’s input through the 2019
Community Health Issues Survey (CHIS)
Once the workgroup had been formed, the first in-person
meeting highlighted that new health concerns could have
emerged in the 5 years since the last SHA, and it would
be necessary to query a sample of community members
regarding new health topics. After determining the Health
Issue Focused Approach was the best model, the SHA
workgroup reviewed the previous survey to improve
upon delivery and clarity. The workgroup contracted
with the University of AL in Tuscaloosa to develop the
2019 survey, asking individuals to choose and rank their
top ten health concerns. This survey was distributed by
paper and electronically with partners and the public for
anyone ages 19 years or older. Leading health concern
results were disseminated to ADPH sta at the state and
public health district level.
Step 2: Gathered surveillance data on the leading
concerns in the community
Through the community feedback, partners also
suggested new or additional data sources to include
in the 2020 SHA to make it more comprehensive. The
workgroup identified multiple sources for each of the
top health indicators to create a broader picture of
community health. The 2020 SHA includes an in-depth
report from a variety of sources such as county-level
census data, behavioral health surveys, health registries,
billing and claims data, the AL State Department of
Education (ALSDE), and local non-profit initiatives.
During the data gathering process, additional data was
collected on specific populations that experience greater
health disparities. Partners also requested local and rural
community resources be incorporated into SHA. The
resources were recommended and compiled by ADPH
program sta.
Step 3: Explained specific health-related concerns
throughout the SHA
The front page of each health indicator includes a
summary of top health concerns identified through
Steps 1 and2. The summary page also highlights areas
where populations are disproportionately aected. The
SHA workgroup identified new data sources and topics
to establish a baseline and to monitor progress on each
major concern. Community resources were expanded
through the local partners and are listed at the end of
each health indicator section.
Identifying the Leading Health
Indicators
Between May and October 2019, CHIS was distributed
in online and paper formats to community members,
organizations, and partners. It received a total of 5,585
responses (1,836partially completed and 3,749fully
completed). This survey was available in English and
Spanish. Most respondents were between the ages of
20 and 64 years old. Healthcare-related professionals
were the primary respondents of the CHIS survey
(38.6percent), followed by educators (9.5percent),
and other government employees (9.3percent).
Approximately 29.7percent of respondents identified
themselves as a minority race. The paper English-version
survey can be found in the Appendix.
Respondents were asked to rank the top ten important
health issues from a list of 59 general health topics with
space included for other concerns to be indicated. The
total was aggregated to identify the 14 leading health
indicators listed below. The team identified two new
indicators since the 2014 survey, “Social Determinants
of Health” and “Environmental Health.” In this document,
each listed indicator will have an introduction that briefly
describes the health concern and recent data to highlight
the current health status. The indicators are:
1. Mental Health and Substance Abuse
2. Access to Care
3. Pregnancy Outcomes
4. Nutrition and Physical Activity
5. Social Determinants of Health (new)
6. Sexually Transmitted Infections
7. Geriatrics
8. Cardiovascular Diseases
9. Child Abuse/Neglect
10. Environmental Health (new)
11. Violence
12. Cancer
13. Diabetes
14. Tobacco Usage and Vaping

2020 ALABAMA STATE HEALTH ASSESSMENT
7
How the Data Was Chosen
To increase utilization and implementation of SHA,
ADPH is creating more opportunities for the community
to view and interact with the population health data.
The purpose of publicly available data is to provide
community partners the opportunity to make data-
driven decisions within their community via policy or
environmental changes.
The final statewide SHA includes detailed data and
information on each health indicator and associated
measures, a comparative ranking of counties for each
concern and indicator (where available), and existing
resources that may be available to assist in intervention. To
keep the document concise, there are only a few measures
for each health indicator. The SHA workgroup chose to
provide the data at the state and county level to represent
as many Alabamians as possible in the identified measure.
Advancements Made Since 2015
The public health system is a collaborative environment,
often relying on the public, private, and community
partners. Every 5 years, ADPH describes the health of
all 67 counties within the jurisdiction. Since the 2015
CHA, the state has continued to make progress in
various areas with a focus on health disparities, such
as incorporating disproportionately aected groups in
routine data collection and community focus groups.
While the information presented is not comprehensive of
all the work done at ADPH since the last SHA, it highlights
ongoing eorts to improve data gathering and inform
local community needs:
· ADPH hired a full-time SHA Coordinator to
continually update the health indicator data,
conduct assessments throughout the state,
and provide timely data to internal and external
partners upon request.
· The department switched from primarily using
paper surveys and contracted with the University
of AL in Tuscaloosa to collect and manage the
online survey responses. By increasing the
online platform, the survey could reach more
populations and health providers.
· In this document, new health indicators
(“Environmental Health” and “Social Determinants
of Health”) were added to explore how the
environment aects an individual’s health. Within
the other 12 indicators, new data points provide
more details about Alabamian health outcomes.
· Partners involved in the development of the SHA
also brought local community issues to the table.
“Health Indicators 3: Poor Pregnancy Outcomes”
(page 47), “Health Indicator 4: Nutrition and
Physical Activity” (page 57), and “Health Indicator
6: Sexually Transmitted Infections” (STI [page
80]) contain sections that further investigate
health disparities and how the built environment
impacts the opportunity to participate in
preventative health behaviors.

2020 ALABAMA STATE HEALTH ASSESSMENT
8
Alabama Economic and
Demographic Data
SHA includes a brief overview of state-level health data
and comparison data from the 2004-2020 United States
(U.S.) Census Bureau and the 2015 CHA.
Alabama has a Growing Elderly Population
· The percent of individuals over 55 years old is
steadily increasing.
· In 2013, the population for 65 years old or more
was 14.9 percent. In 2019, the population for 65
years old or more increased to 17.4 percent.
1
· Nursing home usage and medical expenditures
are expected to continue to rise in the
upcoming decades.
Figure 1 – This graph demonstrates the AL age
distribution by assessment years 2013 and 2019.
Source: U.S. Census Bureau.
0-17
18-24
25-34
35-44
45-54
55-64
65 or more
■2013 ■2019
23.0%
22.1%
10.0%
9.3%
12.8%
13.0%
12.6%
12.4%
13.7%
12.4%
12.9%
13.4%
14.9%
17.4%
Alabamians Mostly Live in Urban Centers
AL’s population was estimated to have increased
2.6percent since the 2010 U.S. Census, particularly in the
areas surrounding six major cities: Auburn, Birmingham,
Huntsville, Montgomery, Mobile, and Tuscaloosa. In 2019,
57.0percent of AL residents live in urban areas.
2
The population shifting to more urban areas can aect
dierent environmental aspects that influence the
health of a community. Examples of the impacts of
this shift include: a small/aordable housing market,
gentrification,
and providers concerned about reaching
rural populations more eectively (e.g., telehealth).
3
Figure 2 – This map represents the population distribution
throughout AL in 2019. Source: U.S.Census Bureau.
Lauderdale
Colbert
Franklin
Marion
Winston
Walker
Limestone
Lawrence
Morgan
Cullman
Madison
Jackson
92,729
98,915
372,909
51,626
55,241
31,362
32,924
119,679
96,774
71,513
26,196
102,268
57,826
57,826
23,629
29,709
13,805
16,302
63,521
89,512
113,605
14,910
22,722
13,235
79,978
217,702
209,355
19,930
12,427
8,111
14,651
8,923
22,394
44,428
10,663
40,367
33,254
164,542
18,068
57,961
10,101
24,686
33,114
13,772
19,448
20,733
12,067
36,633
37,049
52,342
26,271
49,172
17,205
105,882
23,622
16,326
413,210
223,234
81,209
55,869
37,196
18,863
10,373
9,726
226,486
12,589
658,573
Marshall
DeKalb
Cherokee
Etowah
Blount
St. Clair
Calhoun
Cleburne
Clay
Talladega
Randolph
Chambers
Tallapoosa
Coosa
Jeerson
Lamar
Fayette
Tuscaloosa
Bibb
Hale
Sumter
Perry
Dallas
Marengo
Choctaw
Washington
Clarke
Monroe
Conecuh
Butler
Crenshaw
Pike
Barbour
Henry
Dale
Coee
Geneva
2019 AL Population
660,0000
Houston
Covington
Escambia
Baldwin
Mobile
Wilcox
Lowndes
Montgomery
Autauga
Chilton
Elmore
Macon
Bullock
Russell
Lee
Greene
Pickens
Shelby
Almost One-Third of the Alabama Population
Identifies as a Minority Race
Almost one-third (33.2 percent) of the AL population
identifies as a minority race. The fastest growing
minority group is the Hispanic population, growing from
2.3 percent in 2005, to 4.5percent of the AL residents
in 2019.
1
African Americans (AA)/blacks made up 26.9
percent of the AL residents in 2019.
Although the primary language in AL is English, 5.5
percent of residents spoke a non-English language at
home in 2019. Spanish was the most prevalent non-
English languages spoken at home (3.6 percent).
4

2020 ALABAMA STATE HEALTH ASSESSMENT
9
The below demographics do not include temporary
residents, such as students, seasonal employees, and
farm workers.
Table 1 – This table demonstrates the racial and
ethnicity identification of AL residents in 2019. Data
does not round to 100 percent due to estimation
techniques. Source: U.S. Census Bureau.
Racial Identification Count/Percent (%)
AA/black 1,319,551 (26.9)
American Indian/Alaska Native 23,265 (0.5)
Asian 66,129 (1.3)
Native Hawaiian and other
Pacific Islander
1,892 (0.04)
White 3,326,375 (67.8)
Some other race alone 74,451 (1.5)
Two or more races 91,522 (1.9)
Ethnicity Identification Count/Percent (%)
Hispanic 219,296 (4.5)
Non-Hispanic 4,683,889 (95.5)
Over One-Fourth of the Alabama Population are
College Graduates
Educational attainment has been correlated with
better health outcomes. According to the U.S.Census,
87.0percent of Alabamians age 25or older have
graduated from high school or attained post-secondary
education in 2019.
1
This is below the national average in
2019, which was 88.6percent:
· AL is nationally ranked 43rd in education by the
K-12 Achievement Index for 2018. AL had an
overall graduation rate of 90 percent for the class
of 2020.
5
· The largest public-school enrollment size
was elementary children (Grades1-5) with
282,251students. AL had 739,716 students
enrolled during the 2018-2019 school year.
There were 46,766teachers employed in public
schools, or one teacher for every 16students.
5
Figure 3 – This graph demonstrates the educational
attainment of AL residents aged 25 years or older by
assessment years 2013 and 2019. Data does not round
to 100 percent due to estimation techniques. Source:
U.S. Census Bureau.
Less than 12th
Grade, No
Diploma or GED
High School
or GED
Post High
School
College
Graduate
■2013 ■2019
87.0% in 2019
12.9%
15.5%
30.9%
31.0%
29.8%
30.0%
26.3%
23.5%
At the End of 2019, Most of the Eligible Labor Force
was Employed
Employment is an important social indicator
to economic stability. At the end of 2019, the
unemployment rate was 4.9 percent of the active labor
force at that time.
6
93.2%
95.1%
6.8%
4.9%
Figure 4 – This graph demonstrates the employment
rate of AL residents by assessment years 2014 and 2019.
Source: U.S. Census Bureau.
Employed
Unemployed
■2014 ■2019
Nearly 1 out of 5 Alabamians Live Below the Federal
Poverty Line
Poverty and low-income status are associated with a
variety of adverse health outcomes, including shorter
life expectancy, higher likelihood for inadequate health
insurance, and overcrowded housing:
7
· Based on the 2019 Census data, the 100 percent
federal poverty line for a two-person household
was $16,910. For a three-person household, the
poverty line was set to $21,330. The poverty line
limit was $25,750 for a four-person household.
8
· In the 2013, 18.7percent of Alabamians lived
below the federal poverty level.

2020 ALABAMA STATE HEALTH ASSESSMENT
10
· The percentage improved in 2019 to 15.5 percent of
Alabamians living below the federal poverty level.
1
18.7%
15.5%
81.3%
84.5%
Figure 5 – This graph demonstrates federal poverty level
of AL residents by assessment years 2013 and 2019.
Source: U.S. Census Bureau.
Below
Above
■2013 ■2019
Ambulatory Diculty is the Most Common Disability
Filed in Alabama
Living with a disability or special healthcare need can
significantly aect a person’s health. In the table below,
types of disabilities among adults in AL are categorized
by experienced diculties. Individuals may be counted
in more than one group:
· In 2019, 15.9 percent of the population was living with
a disability, which was the same for the 2015 CHA.
9
· According to the Centers for Disease Control and
Prevention (CDC), disability-associated healthcare
expenditures in AL amounted to roughly $9,522 per
person living with a disability in 2015.
10
· Additionally, this population tends to be more
physically inactive, smoke, and have high blood
pressure. In AL, adults with disabilities are more
likely to be obese (45.6 percent) compared to
adults without disabilities (30.9 percent).
11
Table 2 – This table demonstrates types of disabilities
among AL residents in 2019. Source: U.S. Census Bureau.
Disability %
Independent Living Diculty 7.4%
Self-care Diculty 3.3%
Ambulatory Diculty 9.3%
Cognitive Diculty 6.3%
Vision Diculty 3.1%
Hearing Diculty 4.4%
Heart Disease is the Leading Cause of Death in Alabama
In 2018, CDC estimated the average life expectancy in AL
was 75.1 years compared to the national average of 78.7
years.
12
AL had the third worst overall life expectancy in
the U.S., only behind WestVirginia and Mississippi. For
males, the average life expectancy was 72.1 years, and for
females, the average life expectancy was 78.0 years.
12,13
According to CDC, 7 of the 10 leading causes of death are
non-communicable diseases, which can be preventable
with lifestyle changes.
12
Mortality rates are used as
indicators for understanding population-level disease
burden and individual management of chronic diseases.
The leading cause of death in AL was heart disease.
The mortality rate of heart disease has increased
from 256.5deaths per 100,000persons in 2014 to
274.2 deaths per 100,000 persons in 2019.
14
For more
information about cardiovascular diseases (CVDs), see
Health Indicator 8: Cardiovascular Diseases.
Cancer mortality contributes to over 10,000 deaths per
year in AL.
12
AL improved its cancer rate dropping from
212.1 deaths per 100,000 persons in 2014, to 209.3 deaths
per 100,000 persons in 2019.
14
For more information
about cancer, see Health Indicator 12: Cancer.
Figure 6 – This graph demonstrates the crude leading
causes of death among AL residents in 2014 and 2019.
Chronic Lower Respiratory Disease (CLRD) is ranked
third. Source: ADPH Center for Health Statistics.
Heart
Disease
Cancer
CLRD
Stroke
All
Accidents
Alzheimer’s
Disease
Diabetes
Septicemia
Influenza/
Pneumonia
Kidney
Disease
■2014 ■2019 Per 100,000 residents
256.5
274.2
212.1
209.3
62.8
72.0
54.6
64.0
49.9
56.2
38.8
54.2
26.3
24.9
21.3
21.1
21.0
20.8
20.8
20.5

2020 ALABAMA STATE HEALTH ASSESSMENT
11
Written Sources
1. U.S. Census Bureau, American Community
Survey, 1 Year Estimates: Quick Facts Table
V2019, 2019.
2. U.S. Census Bureau, American Community
Survey, 1 Year Estimates: Quick Facts Table
County Level V2019, 2019.
3. U.S. Department of Housing and Urban
Development (USHUD), Displacement of Lower-
Income Families in Urban Areas Report, 2018.
4. U.S. Census Bureau, American Community
Survey, 1 Year Estimates: Language Spoken at
Home Table S1601, 2019.
5. ALSDE, Plan 2020: AL Public High School
Graduation Rates, 2020.
6. U.S. Census Bureau, American Community
Survey, 1 Year Estimates: Selected Economic
Characteristics Table DP03, 2019.
7. Healthy People 2030, Economic Stability, 2020.
8. U.S. Department of Health and Human Services
(USDHHS), 2019 Poverty Guidelines, 2019.
9. U.S. Census Bureau, American Community
Survey, 1 Year Estimates: Disability
Characteristics Table S1810, 2019.
10. CDC, Disability and Health Overview, 2020.
11. CDC, Behavioral Risk Factors Surveillance
System, 2018.
12. CDC Wide-ranging Online Data for Epidemiologic
Research (WONDER), Crude Leading Causes of
Death, 2021.
13. National Vital Statistics Report, Life Expectancy,
2021.
14. ADPH, Center for Health Statistics Mortality Files,
2021.

2020 ALABAMA STATE HEALTH ASSESSMENT
12
Indicators
In this section of SHA, each of the 14 leading
health indicators for AL are presented in
the order they are ranked. Each indicator
has an introduction that briefly describes
the health concerns, disproportionately
aected populations, and why it is important
to the community. Then, the following pages
of data measures address the current health
status of Alabamians in more detail.
At the end of each section, a list of local and
statewide representatives is provided under
resources, along with the data sources.
This includes hospitals, federally qualified
health centers (FQHC), rural health clinics,
education systems, healthcare providers,
government programs, veteran’s aairs
medical centers, and the Young Men’s
Christian Association (YMCA).

2020 ALABAMA STATE HEALTH ASSESSMENT
13
1. Mental Health and Substance Abuse
Ranked AL’s First Health Indicator
The concern for mental health and substance abuse moved
to number one from its previous second highest rank in the
2015 survey. According to the World Health Organization
(WHO), mental health is the “state of well-being in which an
individual realizes his or her own abilities, can cope with the
normal stresses of life, can work productively, and is able to
make a contribution to his or her community.” Mental health
aects an individual’s mood, emotional, psychological, and
social well-being. Family history, biological factors, and life
experiences influence mental health. The most common
mental health illnesses are anxiety, depression, and post-
traumatic stress disorders.
1
According to the Substance Abuse and Mental Health
Services Administration (SAMHSA), 41percent of AL
adults sought medical treatment for a mental health
issue between 2017-2019. Early signs of declining mental
health can be an individual withdrawing from normal social
support, displaying negative emotions, completing daily
tasks, and abusing substances.
2
Substance misuse and
abuse refer to the harmful use of alcohol and illicit drugs,
including prescription drugs.
3
There can be physical, social,
and psychological harm in addition to criminal penalties
for possession of the substance. Often, practitioners
see mental health and substance abuse co-occurring.
Treatment solutions could include individual and group
psychotherapies. Accountability and social support are an
instrumental part of the recovery process. Discrimination,
poverty, and segregation towards individuals with mental
illness are all barriers to seeking treatment.
3
Raising
awareness helps reduce stigma towards mental illness.
Vulnerable Populations
Groups at a higher risk of having a persisting mental illness
are veterans, individuals who have experienced a traumatic
event early in life, and individuals in abusive relationships
or families. In the past 20 years, mental illness rates have
been rising. While more services are available, rural and
minority populations are still underrepresented due to
access to care and social stigma.
3
Geographic Variation
Health outcomes can vary over regions based on the
populations and the opportunities to self-manage care.
For mental health concerns, the Northeastern Public
Health District had the highest suicide rate in 2019. This
area also had the highest substance abuse diagnosis
prevalence in Medicaid recipients in 2018.
Topics Addressed for This Indicator are:
·
Suicide mortality.
· Depression diagnosis among Medicaid recipients.
·
Alabama adults with depression.
· Depression among Medicare recipients.
· Schizophrenia among Medicare recipients.
· Mental health professional shortage areas.
·
Substance abuse diagnosis in Medicaid recipients.
·
Drug-related overdose.
· Drug poisoning mortality.
Highlights
Data by county can be found in the Appendix. Data
for mental health conditions and substance abuse
prevalence are not as complete or comprehensive
as other health indicators. The Centers for Medicare
and Medicaid Services only have limited claims data,
which do not cover the total population. Data are also
retrieved from ADPH Center for Health Statistics, ADPH
Oce of Primary Care and Rural Health, ADPH Oce of
Emergency Medical Services (EMS), the Behavioral Risk
Factor Surveillance System (BRFSS), and the National
Center for Health Statistics:
· In 2019, suicide was the twelfth leading cause of
death in AL.
·
In 2018, 38.8 percent of the adult Medicaid
population-initiated rehabilitation treatment
within 14 days of being diagnosed with an alcohol
or drug dependency.
·
The suicide mortality rate is almost more than
four times greater for males compared to
females (26.6deaths compared to6.9deaths
per 100,000persons).
Risk Factors:
·
Family history.
· Lack of a support system and isolation.
· New, unexpected stressors.
· Chronic illness.
· Dicult life transitions.
· Neglect and abusive relationships.
· Post-traumatic stress disorder.
· Excessive alcohol or previous drug use.
Suicide Mortality
Suicide is one of the leading mental health concerns,
ranking as the tenth leading cause of death in the U.S. and
twelfth for AL.
4
Suicide is death caused by self-injury with
the intent to die:
5
· The Northeastern Public Health District (Blount,
Calhoun, Cherokee, Clay, Cleburne, DeKalb,
Etowah, Shelby, St.Clair, Talladega, and Randolph
counties) had the highest rate of suicide
mortality in AL.

2020 ALABAMA STATE HEALTH ASSESSMENT
14
· The suicide mortality rate is nearly more than four
times greater for males than females (26.6deaths
compared to6.9deaths per 100,000persons).
· The highest suicide mortality rate for 2019 is among
the 35-44 years old age group, with a significant
increase since the 2015 CHA (26.5deaths compared
to 18.7deaths per 100,000persons, respectively).
· Among white individuals, the suicide mortality
rate is 21.8 deaths per 100,000persons in 2019,
compared to 17.3deaths in the 2015 CHA.
Table 1.1 – Suicide Mortality Rate, 2019
Count
Rate per
100,000
AL 804 16.4
U.S. 47,511 14.5
Public Health Districts
Northern 184 16.9
Northeastern 158 19.5
West Central 66 15.2
Jeerson 102 15.5
East Central 101 14.3
Southeastern 58 15.3
Southwestern 71 17.2
Mobile 64 15.5
Geographic Variation
Rural 368 17.5
Urban 436 15.6
Sex
Female 174 6.9
Male 630 26.6
Race/Ethnicity
White 697 21.8
AA/black 82 6.3
Household Income
Not Applicable (N/A) - -
Age (in years)
Under 18 25 2.3
18-24 79 17.7
25-34 129 19.9
35-44 157 26.5
45-54 137 22.2
55-64 119 18.1
65+ 158 18.6
Education
Less than high school 164 -
High school or GED 349 -
Some college 168 -
College graduate or higher 116 -
Unknown 7 -
Depression Diagnosis in Medicaid
Recipients
Depression is defined as a persistent depressed mood
or loss of interest in activities for more than 2 weeks,
causing significant impairment in daily life.
3
The Medicaid
population also includes children:
· In 2018, 3.8 percent of AL Medicaid recipients
had a diagnosis of depression, a decrease from
5.4 percent in the 2015 CHA.
· In 2018, AL Medicaid recipients who identified as white
individuals had more diagnoses than AL Medicaid
recipients who identified as AA/black individuals.
· Mobile had the highest percentage of depression
in the state.
Demographic information was not available for previous
years. For the district level, only confirmed county
diagnoses were included in the calculation.
Table 1.2 – Depression Diagnosis
Among Medicaid Recipients, 2018
Count %
AL 40,977
3.3
U.S. - -
Public Health Districts
Northern 7,535
3.1
Northeastern 6,614 3.4
West Central 3,908 3.2
Jeerson 4,086 2.5
East Central 4,878 2.6
Southeastern 4,415 3.8
Southwestern 4,082 4.3
Mobile 5,423 4.6
Geographic Variation
N/A - -
Sex
Female 28,192 -
Male 12,785 -
Race/Ethnicity
AA/black 13,006 -
Non-Hispanic Asian or Pacific Islander 95 -
White 22,516 -
American Indian/Alaska Native 122 -
Hispanic 625 -
Unknown/Not provided 3,613 -
Household Income
N/A - -
Age (in years)
Under 21 13,278 -
21 and over 27,699 -
Education
N/A - -

2020 ALABAMA STATE HEALTH ASSESSMENT
15
Adults with Depression
Depression is defined as a persistent depressed mood
or loss of interest in activities for more than 2 weeks,
causing significant impairment in daily life.
3
According to BRFSS:
· West Central (25.9 percent) and the Southeastern
(26.7 percent) public health districts had the
highest prevalence of depression in 2019.
· Females continued to have a higher prevalence
of depression with 28.5percent compared
to 19.3 percent in males. In the 2015 CHA, the
prevalence of depression was 26.3 percent in
females and 17.1 percent in males.
· White adults had a prevalence of depression of
26.6 percent compared to AA/black adults with
a prevalence of 17.0percent. These rates were
similar in the 2015 CHA.
· The prevalence is similar throughout age
distributions, but sharply declines over age
65years old with an 18.0percent prevalence.
Table 1.3 – Percentage of Adults
Who Ever Had Depression, 2019
%
95% Confidence
Interval (CI)
AL 24.1 (22.7-25.4)
U.S. - -
Public Health Districts
Northern 25.8 (22.3-29.3)
Northeastern 24.8 (21.5-28.2)
West Central 25.9 (22.0-29.8)
Jeerson 21.1 (17.8-24.5)
East Central 24.4 (20.2-28.6)
Southeastern 26.7 (22.5-30.9)
Southwestern 19.9 (16.5-23.4)
Mobile 21.9 (18.4-25.4)
Geographic Variation
N/A - -
Sex
Female 28.5 (26.5-30.4)
Male 19.3 (17.3-21.2)
Race/Ethnicity
White 26.6 (24.9-28.3)
AA/black 17.0 (14.8-19.3)
Household Income
Less than 15,000 43.5 (38.6-48.4)
$15,000-24,999 30.2 (26.3-34.2)
$25,000-34,999 23.8 (18.5-29.1)
$35,000-49,999 23.7 (19.8-27.6)
$50,000+ 18.5 (16.5-20.6)
Age (in years)
18-24 24.3 (18.7-29.9)
25-34 26.8 (22.8-30.7)
35-44 25.9 (22.4-29.4)
45-54 26.9 (23.7-30.2)
55-64 25.0 (22.3-27.8)
65+ 18.0 (16.1-19.8)
Education
Less than high school 32.8 (28.0-37.6)
High school or GED 24.1 (21.6-26.5)
Some college 25.7 (23.2-28.2)
College graduate or higher 16.4 (14.5-18.2)
Depression Among Medicare Recipients
Depression can be more prevalent for older adults and
persons living with a disability as they experience loss,
Figure 1.1 – This map represents the distribution of
depression prevalence by county. Medicare provides
insurance to persons over the age of 65 years old and
some disabilities. Source: Centers for Medicare and
Medicaid Services.
Lauderdale
Colbert
Franklin
Marion
Winston
Walker
Limestone
Lawrence
Morgan
Cullman
Madison
Jackson
19.3
19.0
18.1
18.1
22.2
22.6
20.9
20.6
20.3
19.7
21.4
24.3
20.8
20.8
19.1
18.6
16.3
20.7
24.0
22.4
19.8
14.8
16.3
18.7
18.6
20.4
20.4
16.0
12.3
14.9
16.6
14.3
22.0
20.6
14.1
15.0
14.8
15.8
10.9
18.2
8.9
16.6
15.9
14.9
14.2
9.9
13.1
15.1
19.0
20.5
20.8
21.2
18.9
21.7
12.7
12.3
15.7
16.2
15.6
16.5
14.0
14.0
11.1
13.0
13.5
14.7
19.4
Marshall
DeKalb
Cherokee
Etowah
Blount
St. Clair
Calhoun
Cleburne
Clay
Talladega
Randolph
Chambers
Tallapoosa
Coosa
Jeerson
Lamar
Fayette
Tuscaloosa
Bibb
Hale
Sumter
Perry
Dallas
Marengo
Choctaw
Washington
Clarke
Monroe
Conecuh
Butler
Crenshaw
Pike
Barbour
Henry
Dale
Coee
Geneva
Prevalence (%)
Houston
Covington
Escambia
Baldwin
Mobile
Wilcox
Lowndes
Montgomery
Autauga
Chilton
Elmore
Macon
Bullock
Russell
Lee
Greene
Pickens
Shelby
25.00

2020 ALABAMA STATE HEALTH ASSESSMENT
16
grief, and physical pain. Identifying depression symptoms
early can help reduce suicides and other health problems.
3
For Medicare recipients:
· The prevalence of depression was 18.4 percent
in 2018, aecting 102,710members. In the 2015
CHA, the prevalence was 13.3percent.
· The Northern District had the highest prevalence
among AL districts.
· Etowah County (a county within the
Northeastern District) had the highest county
prevalence in 2018 (24.3percent). In the
2015CHA, the highest counties were Cullman
and Tuscaloosa (Northern and West Central
Districts, respectively).
Additional demographic information is not available at
this time.
Schizophrenia Among Medicare
Recipients
Schizophrenia is a mental health disorder that includes
hallucinations, delusions, disorganized speech, grossly
disorganized or catatonic behavior, and mood stability
symptoms.
3
People diagnosed with schizophrenia hear,
see, or believe things that are not real. Approximately half
of the individuals with schizophrenia have a co-occurring
mental or behavioral health disorder:
6
· In 2018, there was a state prevalence of
3.1percent with schizophrenia, aecting over
17,000 Medicare fee-for-service recipients. The
prevalence of schizophrenia was 3.5percent in
the 2015 CHA.
· Perry and Dallas counties had the highest
percentage of schizophrenia (5.7percent and
5.6percent, respectively).
Additional demographic information is not available at
this time.
Figure 1.2 – This map represents the distribution
of schizophrenia prevalence by county. Medicare
provides insurance to persons over the age of 65 years
old and some disabilities. Source: Centers for Medicare
and Medicaid Services.
Lauderdale
Colbert
Franklin
Marion
Winston
Walker
Limestone
Lawrence
Morgan
Cullman
Madison
Jackson
2.6
2.1
2.1
2.5
2.5
2.9
2.4
2.9
3.1
3.7
2.6
4.3
2.3
2.3
2.2
2.3
2.6
4.0
3.7
2.4
2.7
2.1
3.3
3.1
2.8
2.6
4.5
3.1
3.9
4.1
3.7
5.7
3.8
2.7
2.6
2.3
3.6
2.8
4.2
3.3
4.6
4.3
4.8
4.0
3.7
3.6
3.5
2.4
4.5
2.8
3.2
3.2
2.9
3.4
3.1
2.0
3.9
1.9
2.8
2.5
5.6
4.7
4.0
4.6
3.0
3.0
4.1
Marshall
DeKalb
Cherokee
Etowah
Blount
St. Clair
Calhoun
Cleburne
Clay
Talladega
Randolph
Chambers
Tallapoosa
Coosa
Jeerson
Lamar
Fayette
Tuscaloosa
Bibb
Hale
Sumter
Perry
Dallas
Marengo
Choctaw
Washington
Clarke
Monroe
Conecuh
Butler
Crenshaw
Pike
Barbour
Henry
Dale
Coee
Geneva
Prevalence (%)
Houston
Covington
Escambia
Baldwin
Mobile
Wilcox
Lowndes
Montgomery
Autauga
Chilton
Elmore
Macon
Bullock
Russell
Lee
Greene
Pickens
Shelby
25.00
Mental Health Professional
Shortage Areas
A good system of mental health resources can assist all
populations in managing their mental health outcomes,
which can include: insurance coverage, reduction of
barriers associated with social stigma, and awareness
of resources.
3
One critical resource is access to local
mental health providers.
The map in Figure 1.3 depicts:
· Mental health professional areas that have a
provider shortage either by geographic or low-
income designation.

2020 ALABAMA STATE HEALTH ASSESSMENT
17
· Mental health professionals included in this data
are medical doctors practicing general
medicine and child psychiatry.
· Health Professional Shortage Areas (HPSA)
scores range from 1-25, with 25 being the most
significant disparity.
In 2018, Madison County was the only county with
sucient mental health professionals to provide services
to its residents. However, services were more adequately
covered in the Northern Public Health District than the
rest of the state.
Figure 1.3 – This map represents the HPSA score,
ranging from 1 to 25, for each county. Source: ADPH
Oce of Primary Care and Rural Health.
Lauderdale
Colbert
Franklin
Marion
Winston
Walker
Limestone
Lawrence
Morgan
Cullman
Madison
Jackson
11
12
15
11
11
12
12
15
17
17
17
18
16
19
19
19
19
19
18
10
10
18
18
18
11
18
18
18
18
18
20
18
11
18
17
17
17
17
17
17
17
17
18
18
18
18
18
18
18
17
17
17
17
18
19
19
5
16
16
20
18
20
16
16
18
18
Marshall
DeKalb
Cherokee
Etowah
Blount
St. Clair
Calhoun
Cleburne
Clay
Talladega
Randolph
Chambers
Tallapoosa
Coosa
Jeerson
Lamar
Fayette
Tuscaloosa
Bibb
Hale
Sumter
Perry
Dallas
Marengo
Choctaw
Washington
Clarke
Monroe
Conecuh
Butler
Crenshaw
Pike
Barbour
Henry
Dale
Coee
Geneva
HPSA Designation Type
Houston
Covington
Escambia
Baldwin
Mobile
Wilcox
Lowndes
Montgomery
Autauga
Chilton
Elmore
Macon
Bullock
Russell
Lee
Greene
Pickens
Shelby
Numerals indicate HPSA Scores (Range: 1-25)
Geographic Low-Income Non-Designated
Substance Abuse Diagnosis in
Medicaid Recipients
Substance abuse is defined as taking a controlled
substance in a harmful dose. This could include
consumption of alcohol, prescription pain medication,
and other illicit drugs.
Following up with long care support and rehabilitation
services is important for recovery in this population. In
2018, 38.8percent of the adult Medicaid population-
initiated treatment within 14days of being diagnosed:
7
· In 2018, there were 18,037Medicaid fee-for-
service recipients diagnosed with substance
abuse in AL.
7
·
The Northeastern Public Health District had the
highest prevalence of substance abuse diagnosis
with 1.73 percent of all Medicaid recipients.
·
Females were diagnosed more when compared
to males.
This information was calculated dierently in the 2015
CHA and cannot be used to assess an accurate historical
trend. For the district level, only confirmed county
diagnoses were included in the calculation.
Table 1.4 – AL Substance Abuse Diagnosis
in Medicaid Recipients, 2018
Count %
AL 18,037 1.5
U.S. - -
Public Health Districts
Northern 4,018 1.67
Northeastern 3,359 1.73
West Central 2,017 1.67
Jeerson 2,366 1.46
East Central 1,553 0.87
Southeastern 1,496 1.29
Southwestern 1,423 1.26
Mobile 1,565 1.32
Geographic Variation
N/A - -
Sex
Female 10,876 -
Male 7,161 -

2020 ALABAMA STATE HEALTH ASSESSMENT
18
Race/Ethnicity
White 10,912 -
American Indian/Alaska Native 54 -
Asian 361 -
AA/black 4,419 -
Hispanic 162 -
Other/Not provided 2,471 -
Household Income
N/A - -
Age (in years)
N/A - -
Education
N/A - -
Drug-related Overdose
According to CDC, AL’s opioid dispensing rate was
the highest prescribing rate in the country with 85.8
medications for every 100 persons in 2019.
8
This rate
was significantly higher than the average U.S. rate of 46.7
prescriptions per 100 persons.
8
The maps show the rates of all drug and opioid overdose
emergency response (911 runs) by county in 2018.
· The average rate of drug-related overdose
911 runs was 37.8 per 10,000 persons, and the
average rate of opioid-related overdose runs was
5.5 per 10,000 persons.
· The rate of 911 runs for overdoses were highest in
Jeerson County and the surrounding area.
Naloxone is a medication designed to reverse opioid overdose
rapidly. One dose of naloxone counts as one administration:
· In 2018, 6,287 doses of naloxone were administered
and reported to the Oce of EMS, a 34.7 percent
increase from 2017 (4,666 doses administered).
9
· The administration was highest in males
2544years old with over 1,500 naloxone
administrations. The number of administrations
may be higher than the number of persons who
may receive more than one injection.
This data does not account for outcomes after
administration. Naloxone administration may be
aected by availability. ADPH plans to utilize Syndromic
Surveillance System data by identifying overdoses
through emergency room visits.
Figure 1.4 – The number of drug-related overdose 911 runs
by county. The map is further broken down into opioid-
related runs by county. White counties show areas where
data was not collected. Source: ADPH Oce of EMS.
Lauderdale
Colbert
Franklin
Marion
Winston
Walker
Limestone
Lawrence
Morgan
Cullman
Madison
Jackson
Marshall
DeKalb
Cherokee
Etowah
Blount
St. Clair
Calhoun
Cleburne
Clay
Talladega
Randolph
Chambers
Tallapoosa
Coosa
Jeerson
Lamar
Fayette
Tuscaloosa
Bibb
Hale
Sumter
Perry
Dallas
Marengo
Choctaw
Washington
Clarke
Monroe
Conecuh
Butler
Crenshaw
Pike
Barbour
Henry
Dale
Coee
Geneva
Houston
Covington
Escambia
Baldwin
Mobile
Wilcox
Lowndes
Montgomery
Autauga
Chilton
Elmore
Macon
Bullock
Russell
Lee
Greene
Pickens
Shelby
Average 37.8 per 10,000 population
2018 Rates of All Drug-Related Overdose
911 Runs by County of Residence
100.00.0
Lauderdale
Colbert
Franklin
Marion
Winston
Walker
Limestone
Lawrence
Morgan
Cullman
Madison
Jackson
Marshall
DeKalb
Cherokee
Etowah
Blount
St. Clair
Calhoun
Cleburne
Clay
Talladega
Randolph
Chambers
Tallapoosa
Coosa
Jeerson
Lamar
Fayette
Tuscaloosa
Bibb
Hale
Sumter
Perry
Dallas
Marengo
Choctaw
Washington
Clarke
Monroe
Conecuh
Butler
Crenshaw
Pike
Barbour
Henry
Dale
Coee
Geneva
Houston
Covington
Escambia
Baldwin
Mobile
Wilcox
Lowndes
Montgomery
Autauga
Chilton
Elmore
Macon
Bullock
Russell
Lee
Greene
Pickens
Shelby
Average 5.5 per 10,000 population
2018 Rates of Opioid-Related Overdose
911 Runs by County of Residence
40.00.0

2020 ALABAMA STATE HEALTH ASSESSMENT
19
Drug Poisoning Mortality
According to CDC, in 2019, there were 827drug
poisoning deaths in AL with a rate of 16.9per 100,000
persons compared to the national rate of 23.1 per
100,000persons. Compared to 2013, there were 648drug
poisoning deaths with a crude rate of 13.4deaths per
100,000persons.
10
This includes both intentional and
unintentional poisonings noted on death certificates.
In Figure 1.5, the map is modeling age-adjusted drug poisoning
deaths from the National Center for Health Statistics:
· In 2019, The highest drug poisoning death rates
by county were Russell County with 38.0deaths,
Dekalb County with 32.2deaths, Jeerson
County with 31.0deaths, and St. Clair County with
25.7 deaths per 100,000persons.
· In 2013, Walker County previously had the highest
death rate with 43.9deaths per 100,000 persons.
These rates are an underestimation of the total amount.
If poisoning is not suspected, a drug test may not be run.
ADPH plans to use Poison Control Center data to better
understand the prevalence and distribution in AL.
Data Sources
Table 1.1 – Suicide Mortality, 2019. ADPH, Center for Health
Statistics Mortality Files, 2019. Data requested March 2021.
Table 1.2 – Depression Diagnosis Among Medicaid
Recipients, 2018. AL Medicaid Agency, 2019. Data
requested July 2020.
Table 1.3 – Percentage of Adults Who Ever Had
Depression, 2019. CDC, BRFSS, 2019. Data requested
March 2021.
Figure 1.1 – Depression Among Medicare Recipients,
2018. Centers for Medicare and Medicaid Services, 2019.
Data requested January 2021.
Figure 1.2 – Schizophrenia Among Medicare
Recipients, 2018. Centers for Medicare and Medicaid
Services, 2019. Data requested January 2021.
Table 1.4 – AL Substance Abuse Treatment
Admissions in Medicaid Recipients, 2018-2019. AL
Medicaid Agency, 2019. Data requested July 2020.
Figure 1.4 – Rates of Drug Overdose-Related 911 Runs
by County of Residence, 2018. ADPH, Oce of EMS,
2018. Data requested January 2021.
Figure 1.5 – Drug Poisoning Mortality, 2018. National Center
for Health Statistics, 2018. Data requested March 2021.
Written Sources
1. WHO, Mental Well-Being, 2020.
2. SAMHSA, Behavioral Health Barometer Region 4,
Volume 6. Adult Mental Health and Service Use, 2020.
3. CDC, Mental Health, 2020.
4. CDC National Center for Health Statistics, Age
Adjusted Leading Causes of Death, 2019.
5. CDC, Suicide Prevention, 2020.
6. National Institute of Mental Health, Schizophrenia, 2020.
7. National Alliance on Mental Illness, Substance Abuse
Disorders, 2020.
8. CDC, U.S. State Opioid Dispensing Rates, 2019.
9. ADPH, Oce of Emergency Medical Services, 2018.
10. CDC National Center for Health Statistics, Drug
Poisoning Mortality, 2018.
Figure 1.5 – This map represents the mortality rate due
to drug poisonings in AL. Source: National Center for
Health Statistics.
Lauderdale
Colbert
Franklin
Marion
Winston
Walker
Limestone
Lawrence
Morgan
Cullman
Madison
Jackson
16.2
13.7
13.3
16.6
12.7
18.7
16.7
19.3
18.2
22.2
21.1
24.2
21.7
21.6
20.3
17.4
18.7
20.2
26.6
27.1
17.2
24.2
19.5
17.0
17.6
18.6
16.1
19.5
17.5
16.4
18.2
16.6
23.0
19.7
16.1
14.0
13.9
9.5
11.1
14.5
12.0
14.6
14.4
13.1
16.7
16.2
21.3
26.8
15.3
11.5
18.2
12.6
16.3
16.0
16.5
19.1
15.8
16.6
10.6
13.2
11.1
16.0
14.5
12.8
9.1
18.9
27.2
Marshall
DeKalb
Cherokee
Etowah
Blount
St. Clair
Calhoun
Cleburne
Clay
Talladega
Randolph
Chambers
Tallapoosa
Coosa
Jeerson
Lamar
Fayette
Tuscaloosa
Bibb
Hale
Sumter
Perry
Dallas
Marengo
Choctaw
Washington
Clarke
Monroe
Conecuh
Butler
Crenshaw
Pike
Barbour
Henry
Dale
Coee
Geneva
Rate per 100,000
Houston
Covington
Escambia
Baldwin
Mobile
Wilcox
Lowndes
Montgomery
Autauga
Chilton
Elmore
Macon
Bullock
Russell
Lee
Greene
Pickens
Shelby
30.00

2020 ALABAMA STATE HEALTH ASSESSMENT
20
Community Resources
AL Department of Mental Health
Location: Montgomery County, AL
Type: State Government Organization
AL Department of Rehabilitation Services
Location: Montgomery County, AL
Type: State Government Organization
Alabama Suicide Prevention & Resources Coalition
Location: Jeerson County, AL
Type: Non-profit Organization
Brewer-Porch Children’s Center
Location: Tuscaloosa County, AL
Type: Research Institution
CDC
Location: Atlanta, GA
Type: Federal Government Organization
Consumer Product Safety Commission
Location: Atlanta, GA
Type: Federal Government Organization
Health Resources and Services Administration (HRSA)
Location: Washington, DC Metro
Type: Federal Government Organization
Hill Crest Behavioral Health Services
Location: Jeerson County, AL
Type: Behavioral Health Facility
Laurel Oaks Behavioral Health Center
Location: Houston County, AL
Type: Behavioral Health Facility
National Institute on Alcohol Abuse and Alcoholism
Location: Bethesda, MD
Type: Federal Government Organization
National Institute on Drug Abuse
Location: Washington, DC Metro
Type: Federal Government Organization
National Suicide Prevention Lifeline
1-(800) 273-8255
Location: Washington, DC Metro
Type: Federal Government Partnership
Sequel Courtland
Location: Lawrence County, AL
Type: Youth Behavioral Health Facility
Sequel Tuskegee
Location: Macon County, AL
Type: Youth Behavioral Health Facility

2020 ALABAMA STATE HEALTH ASSESSMENT
21
2. Access to Care
Ranked AL’s Second Health Indicator
Alabamians identified access to care as the second
highest ranked health indicator in the community health
system. Healthy People 2030 describes access to care
as “the timely use of personal health services to achieve
the best possible health outcomes.”
1
Addressing access
to healthcare services improves prevention of disease
and reduces disability due to disease by allowing early
detection and treatment of health conditions.
Quality access to care solutions can increase a
community’s quality of life, reduce preventable deaths,
and increase the population’s life expectancy. A well-
developed care system can give an individual access to
insurance cost coverage, geographic availability, and a
personal relationship with the provider.
2
This allows the
community to gain entry into the healthcare system,
access a healthcare location where needed services are
provided, and find a healthcare provider with whom the
individual can communicate and trust long-term.
Vulnerable Populations
Anyone can be categorized as having limited access to
care; however, having two or more limited access factors
can decrease your overall health. Rural and underinsured
individuals could be at a higher risk for not having proper
access to care. Additionally, individuals who have
unstable income, such as small business owners and
individuals in the service industry, could be at risk of
losing health insurance coverage.
3
Geographic Variation
Rural AL is the primary geographic location at risk for this
outcome, and rurality is addressed under various health
measures throughout SHA.
Topics Addressed for This Indicator are:
· Percent of Alabamians with no healthcare coverage.
· Rural healthcare facilities.
· Households without a vehicle.
· Primary care HPSAs.
Highlights
Data are retrieved from the Rural Health Information Hub, the
ADPH Oce of Primary Care and Rural Health, and BRFSS:
· In 2019, a higher percentage of AL’s population
was uninsured than the U.S. (17.5percent
compared to 13.6 percent).
· Alabamians between 18-24 years old have the
highest percentage of the uninsured population
at 24.3 percent.
Risk Factors:
· Income level.
· Job stability/unemployment.
· Health insurance coverage.
· Geography/rural residents.
· Perceived discrimination from providers.
· Access to reliable information.
Percent of Alabamians with no
Healthcare Coverage
While healthcare coverage does not directly correlate to
access to care, it poses a barrier to receiving early and
preventive care:
3
· AL had a higher percentage of the uninsured
population than the U.S. (17.5percent compared
to 13.6 percent) in 2019.
· The Southeastern Public Health District had the
highest percentage of the uninsured population.
· Males have a higher uninsured prevalence
compared to females (18.9 percent and 16.3
percent, respectively).
· AA/black adults have higher uninsured prevalence
healthcare coverage than white adults
(18.7percent and 15.1 percent, respectively).
· Alabamians between 18-24 years old have the
highest percentage of the uninsured population at
24.3 percent. After 65years old, most individuals
are covered by Medicare or private insurance.
* In Table 2.1, rural and urban calculations were supplied
by the U.S. Census Bureau.
Table 2.1 – Percentage of Alabamians Ages 18-64
Years Old with no Healthcare Coverage, 2019
% 95% CI
AL 17.5 (15.9-19.1)
U.S. 13.6 -
Public Health Districts
Northern 20.8 (16.3-25.2)
Northeastern 16.5 (12.7-20.2)
West Central 14.3 (10.4-18.1)
Jeerson 17.0 (13.1-20.8)
East Central 16.9 (12.3-21.5)
Southeastern 22.6 (17.2-28.0)
Southwestern 11.3 (8.1-14.5)
Mobile 18.0 (14.0-22.1)

2020 ALABAMA STATE HEALTH ASSESSMENT
22
Geographic Variation *
Rural 12.8 -
Urban 11.3 -
Sex
Male 18.9 (16.4-21.3)
Female 16.3 (14.2-18.4)
Race/Ethnicity
White 15.1 (13.3-16.8)
AA/black 18.7 (15.6-21.8)
Household Income
Less than $15,000 29.1 (23.1-35.1)
$15,000-24,999 31.3 (26.1-36.4)
25,000-$34,999 19.3 (13.6-25.0)
$35,000-$49,999 13.8 (9.9-17.6)
$50,000+ 6.7 (5.1-8.4)
Age (in years)
18-24 24.3 (18.4-30.2)
25-34 19.9 (16.2-23.6)
35-44 20.7 (17.2-24.3)
45-54 13.7 (11.2-16.3)
55-64 10.8 (8.6-13.1)
Education
N/A - -
Rural Healthcare Facilities
Rural and urban are defined at the county level since most
data is not available at sub-county levels. The model used
considers the three following widely accepted indicators that
tend to describe accepted concepts of rural and urban areas:
1. Public education employment as a percentage of total
non-agricultural employment.
2. Agricultural sales per square mile of land surface.
3. Population per square mile of land surface:
· AL’s geography is considered 96 percent rural.
· Figure 2.1 shows AL’s rural healthcare facilities as of
October 2020. The graph includes critical access
hospitals, rural health clinics, and FQHC sites.
· In 2019, AL had 5 critical access hospitals, 117rural
health clinics, 105 FQHC sites, and 48short-term
hospitals located outside urbanized areas.
· Some rural hospitals have faced financial
challenges for staying open, such as low
reimbursement rates, reduced patient volumes,
and uncompensated care.
4
· The disparity of access to care can be seen in
Medicaid enrollment data. The annual statewide
Medicaid eligibility for both adults and children is
24.7 percent. In rural populations, the Medicaid
eligibility is 48.1percent.
Figure 2.1 – This map represents rural healthcare
facilities in AL. Green circles are rural health clinics, blue
circles are critical access hospitals, and red circles are
FQHC sites outside of urban areas. The yellow patches
are urban areas determined by the U.S. Census Bureau.
Source: Rural Health Information Hub, 2019.
Critical Access Hospital
Rural Health Clinic
Federally Qualified Health Center Site Outside of Urbanized Area
U.S. Census Bureau Urbanized Area
Households without a Vehicle
AL has very few public transportation options outside
of urban centers. In 13 counties, there are no public
transportation options as of March2021:
5
· Overall, 5.8 percent of rural households did not
have access to a car compared to the 4.4percent
of urban households between 2015-2019.
7
· The Southwestern Public Health District had
the highest concentration of households
without a vehicle.

2020 ALABAMA STATE HEALTH ASSESSMENT
23
· Greene County had the highest percent of
households without a vehicle (18.0percent)
between 2015-2019. This area is covered by the
West Alabama Public Transportation system.
7,8
· The second highest area was Wilcox County, with
an estimated 15.6 percent of households did not
have a vehicle between years 2015-2019. In this
area, there is a rural transportation program that
oers services for dialysis patients, individuals
who need handicap transportation, and low-
income work employees.
7,8
·Statewide, travel time to work was increasing for
residents. In the previous CHA, 15.9 percent of
commuters took more than 35minutes to arrive
to work. In 2019, 21.5 percent of commuters took
over 35minutes to get to work.
7
Figure 2.2 – The percentage of households without
vehicles is represented by county. Yellow counties
indicate a higher proportion of households without
vehicles. Source: U.S. Census Bureau.
Lauderdale
Colbert
Franklin
Marion
Winston
Walker
Limestone
Lawrence
Morgan
Cullman
Madison
Jackson
6.3
3.0
4.7
4.3
5.5
4.9
5.9
5.0
4.6
5.2
4.5
6.1
4.1
3.8
5.3
5.9
6.9
7.5
5.4
3.2
6.0
5.0
6.5
4.8
7.8
2.8
6.0
10.3
10.9
18.0
10.0
13.0
6.2
5.0
4.0
7.9
7.3
4.4
12.3
10.3
10.7
10.2
7.0
6.8
7.5
10.8
6.8
5.1
5.4
5.9
6.1
4.9
6.3
6.2
8.1
4.3
7.1
3.3
4.5
4.4
14.0
10.5
15.6
12.5
8.1
9.2
7.7
Marshall
DeKalb
Cherokee
Etowah
Blount
St. Clair
Calhoun
Cleburne
Clay
Talladega
Randolph
Chambers
Tallapoosa
Coosa
Jeerson
Lamar
Fayette
Tuscaloosa
Bibb
Hale
Sumter
Perry
Dallas
Marengo
Choctaw
Washington
Clarke
Monroe
Conecuh
Butler
Crenshaw
Pike
Barbour
Henry
Dale
Coee
Geneva
Percent of Households
Houston
Covington
Escambia
Baldwin
Mobile
Wilcox
Lowndes
Montgomery
Autauga
Chilton
Elmore
Macon
Bullock
Russell
Lee
Greene
Pickens
Shelby
20.00
Primary Care Health Professional
Shortage Areas
HPSAs represent a geographical service area with
shortages of providers compared to the whole
population. The HPSA score is calculated by using a
federally determined algorithm. The higher scores
indicate a demand for additional services.
Primary care health professionals include medical and
osteopathic doctors practicing family medicine, general
medicine, general pediatrics, general internal medicine, or
general obstetrics and gynecological (OB-GYN) services.
In 2015, the Oce of Telehealth began an initiative to
set up additional capacity for telemedicine services. By
2018, the Oce of Telehealth partnered with providers to
successfully oer telemedicine to rural communities by
increasing services in all county health departments.
Figure 2.3 – This map represents the HPSA score,
ranging from 1 to 25, for each county. Source: ADPH
Oce of Primary Care and Rural Health.
Lauderdale
Colbert
Franklin
Marion
Winston
Walker
Limestone
Lawrence
Morgan
Cullman
Madison
Jackson
14
15
9
14
10
15
11
10
14
15
15
15
13
15
15
15
15
16
9
13
18
17
12
13
15
13
18
23
20
19
16
16
14
14
16
18
20
21
20
11
18
18
18
15
11
16
17
15
11
18
14
13
5
16
15
17
18
22
16
20
Marshall
DeKalb
Cherokee
Etowah
Blount
St. Clair
Calhoun
Cleburne
Clay
Talladega
Randolph
Chambers
Coosa
Lamar
Fayette
Tuscaloosa
Bibb
Hale
Sumter
Perry
Dallas
Marengo
Choctaw
Washington
Clarke
Monroe
Conecuh
Butler
Crenshaw
Pike
Barbour
Henry
Dale
Coee
Geneva
HPSA Designation Type
Houston
Covington
Escambia
Baldwin
Mobile
Wilcox
Lowndes
Montgomery
Chilton
Macon
Bullock
Russell
Lee
Greene
Pickens
Shelby
Numerals indicate HPSA Scores (Range: 1-25)
Geographic Low-Income Non-Designated
17
Tallapoosa
Elmore
16
12
Autauga
15
Jeerson
20
18
Tallapoosa
21
15
18
16

2020 ALABAMA STATE HEALTH ASSESSMENT
24
Data Sources
Table 2.1 – Percentage of Alabamians Ages 18-64
Years Old with no Healthcare Coverage, 2019. U.S.
Census Bureau, American Community Survey, 1 Year
Estimates: Quick Facts Table V2019, 2019 and CDC,
BRFSS, 2019. Data requested March 2021.
Figure 2.1 – Selected Rural Healthcare Facilities in AL.
USDHHS, Rural Health Information Hub., HPSA Survey
2011-2014. Data requested July 2020.
Figure 2.2 – Percentage of Households without a
Vehicle, 2015-2019. U.S. Census Bureau, American
Community Survey, 5 Year Estimates Table DP04, 2019.
Data requested March 2021.
Figure 2.3 – Primary Care HPSA, January 2019. ADPH,
Oce of Primary Care and Rural Health, HPSA Survey
2011-2014. Data requested July 2020.
Written Sources
1. Healthy People 2030, Access to Healthcare, 2020.
2. CDC, Access to Care, 2021.
3. Rural Health Information Hub, Healthcare Access in
Rural Communities.
4. Rural Health Information Hub, Rural Hospitals, 2020.
5. AL Transit, Directory of Transportation Providers, 2021.
6. Rural Health Information Hub, Transportation to
Support Rural Healthcare, 2020.
7. U.S. Census Bureau, American Community Survey, 1
Year Estimates, 2019.
8. ALDOT, Rural Transportation Program, 2021.
Community Resources
AL Department of Economic and Community Aairs
Location: Montgomery County, AL
Type: State Government Organization
ALSDE
Location: Montgomery County, AL
Type: State Government Organization
AL Department of Labor (ALDOL)
Location: Montgomery County, AL
Type: State Government Organization
AL Partnership for Telehealth
Location: Montgomery County, AL
Type: Nonprofit Organization
AL Hospital Association
Location: Montgomery County, AL
Type: Advocacy Organization
AL Medicaid Agency’s Non-Emergency
Transportation Program
Location: Montgomery County, AL
Type: For-profit Organization
AL Oce of Primary Care and Rural Health
Location: Montgomery County, AL
Type: State Government Organization
AL Primary Healthcare Association
Location: Montgomery County, AL
Type: Advocacy Organization
AL Rural Health Association
Location: Montgomery County, AL
Type: Private Education Society
Connecting AL
Location: Montgomery County, AL
Type: Private Non-profit
State Health Planning and Development Agency
Location: Montgomery County, AL
Type: State Government Organization
Kid One Transport
Location: Montgomery County, AL
Type: Non-profit Organization

2020 ALABAMA STATE HEALTH ASSESSMENT
25
3. Pregnancy Outcomes
Ranked AL’s Third Health Indicator
Pregnancy outcomes remained in the top three primary
health indicators for AL. Biological and social factors
aecting the length of the pregnancy or the infant’s
survival may impact pregnancy outcomes.
The complications and possible loss of a baby is
physically and mentally dicult, and a long recovery for
both parents.
1
AL ranks 47th for infant mortality rate in
2019.
2
About 1 in 100pregnancies result in stillbirth, which
is the death of a baby before or during delivery.
1
Strategies to improve pregnancy outcomes include
breastfeeding and family planning. Breastfeeding is
the best source of nutrition for most infants and can
reduce the risk of health conditions for both infants
and mothers.
2
Breastfeeding also helps strengthen the
infant’s immune and digestive system during the first
year of their life.
Family planning can help reduce unexpected
pregnancies, particularly in teen mothers. Contraception
can increase safe sexual practices and protect
individuals from sexually transmitted infections
(STIs).
2
Reversible birth control methods can include
intrauterine contraception, hormonal methods, and
barrier methods. Permanent methods of birth control
include female and male sterilization, such as tubal
ligation and vasectomy.
Vulnerable Populations
Many social and biological factors also aect the time
the mother begins prenatal care and the number of visits
she receives. For AL, AA/black women have double the
infant mortality rate than white women, highlighting racial
and ethnic disparities present for expecting mothers to
overcome.
2
Improving generational health outcomes start
with family planning, lowering maternal stress, implementing
good nutritional choices, detecting and preventing diabetes.
Geographic Variation
The areas with the highest rates of teen pregnancy
are in Wilcox and Greene counties. The areas with
the highest rates of infant mortality are in Coosa and
Greene counties. As demonstrated in this chapter, poor
pregnancy outcomes mainly occur where there is a lack
of public obstetrical services in the state.
Topics Addressed for This Indicator are:
· Inadequate prenatal care.
· Obstetrical services in AL, 1980-2019.
· Infant mortality.
· Low birth weight.
· Teen pregnancy.
Highlights
Data are collected by hospitals and transmitted
electronically to ADPH Center for Health Statistics. Data
are also retrieved from ADPH Oce of Primary Care and
Rural Health:
· The infant mortality rate was 7.7deaths per
1,000 births for 2019. In the 2015 CHA, the infant
mortality rate was 8.5deaths per 1,000 births.
· The disparity of infant mortality in minority
females is two times higher when compared to
white females.
· Over 1 out of every 10 births in AL were babies
born with low birth weights.
Risk Factors:
· Socioeconomic disadvantage.
· Failure of natural labor progression.
· Chronic health conditions.
· Inadequate prenatal care.
· Smoking, alcohol, and illicit drug use.
· Untreated STIs.
· Transportation to prenatal care.
· Stress or physical abuse during pregnancy.
Inadequate Prenatal Care
Inadequate prenatal care is defined as seeking medical
or prenatal services after the fourth month of pregnancy
or prenatal care that included fewer than half of the
recommended visits:
1
· In 2019, 1 in 4 pregnancies in AL had inadequate
prenatal care (25.8percent). In the 2015 CHA,
the percentage was similar; 24.8percent had
inadequate prenatal care.
· Urban areas have higher rates of inadequate
prenatal care (27.2percent) than rural areas
(23.8percent).
· Mothers who were not married during their
pregnancy were more likely to not receive
adequate prenatal care (34.4percent) than
mothers who were married (18.8percent).
· Young mothers under 20 years old have the highest
inadequate prenatal care rate (35.6 percent) than
any other age group.

2020 ALABAMA STATE HEALTH ASSESSMENT
26
Table 3.1 – Inadequate Prenatal Care, 2019
Count %
AL 15,115 25.8
U.S. - -
Public Health Districts
Northern 3,309 26.4
Northeastern 2,276 25.4
West Central 1,802 34.1
Jeerson 2,584 30.5
East Central 1,972 22.4
Southeastern 921 20.1
Southwestern 1,066 23.1
Mobile 1,185 22.1
Geographic Variation
Rural 5,761 23.8
Urban 9,354 27.2
Sex
N/A - -
Race/Ethnicity
White 8,851 23.3
AA/black 5,715 30.6
Other 549 -
Marital Status
Not married 9,019 34.4
Married 6,088 18.8
Mother’s Age (in years)
Under 20 1,424 35.6
20-24 4,499 29.5
25-29 4,660 25.0
30-34 3,007 21.8
35+ 1,525 22.1
Mother’s Education
N/A - -
Obstetrical Servicers in Alabama
1980-2019
Many primary care physicians are expanding their
rural obstetrical care due to the drastic reduction of
available OB-GYN services in rural areas.
3
In 2019, 16rural
counties oered hospital-based obstetrical services
in AL, compared to the 45 rural counties with hospitals
providing obstetrical services in 1980.
Prenatal care availability may have been impacted by
access to obstetrical services:
· According to the ADPH Center for Health
Statistics Natality records, in 2019, there were
1,478 births in AL that received no prenatal care.
· In 2019, over 25 percent of all births in AL involved
females who had less than adequate prenatal
care during their pregnancy.
4
· This percentage was the highest in rural Greene and
Hale counties, 59.3 and 42.5percent, respectively.
Figure 3.1 – A picture of the loss of rural obstetrical
services in rural AL in the past 40 years. Source: ADPH
Oce of Primary Care and Rural Health.
Lauderdale
Colbert
Franklin
Marion
Winston
Walker
Limestone
Lawrence
Morgan
Cullman
Madison
Jackson
Marshall
DeKalb
Cherokee
Etowah
Blount
St. Clair
Calhoun
Cleburne
Clay
Talladega
Randolph
Chambers
Tallapoosa
Coosa
Jeerson
Lamar
Fayette
Tuscaloosa
Bibb
Hale
Sumter
Perry
Dallas
Marengo
Choctaw
Washington
Clarke
Monroe
Conecuh
Butler
Crenshaw
Pike
Barbour
Henry
Dale
Coee
Geneva
Houston
Covington
Escambia
Baldwin
Mobile
Wilcox
Lowndes
Montgomery
Autauga
Chilton
Elmore
Macon
Bullock
Russell
Lee
Greene
Pickens
Shelby
Lauderdale
Colbert
Franklin
Marion
Winston
Walker
Limestone
Lawrence
Morgan
Cullman
Madison
Jackson
Marshall
DeKalb
Cherokee
Etowah
Blount
St. Clair
Calhoun
Cleburne
Clay
Talladega
Randolph
Chambers
Tallapoosa
Coosa
Jeerson
Lamar
Fayette
Tuscaloosa
Bibb
Hale
Sumter
Perry
Dallas
Marengo
Choctaw
Washington
Clarke
Monroe
Conecuh
Butler
Crenshaw
Pike
Barbour
Henry
Dale
Coee
Geneva
Houston
Covington
Escambia
Baldwin
Mobile
Wilcox
Lowndes
Montgomery
Autauga
Chilton
Elmore
Macon
Bullock
Russell
Lee
Greene
Pickens
Shelby
Obstetrical Service in Alabama - 1980
■■Counties with Hospitals Providing Obstetrics
Obstetrical Service in Alabama - May 2019
■■Counties with Hospitals Providing Obstetrics

2020 ALABAMA STATE HEALTH ASSESSMENT
27
Infant Mortality
Infant mortality is the number of children who died
before their first birthday divided by the number of live
births during the year.
1
In AL, the leading cause of infant
deaths includes low birthweight and gestation under
37weeks, congenital malformations, Sudden Infant Death
Syndrome (SIDS), and bacteria sepsis of newborns:
2
· The infant mortality rate was 7.7deaths per 1,000
births for 2019. In the 2015 CHA, the infant mortality
rate was 8.5deaths per 1,000 births.
· The West Central Public Health District had the
highest infant mortality rate of 10.8deaths per
1,000 births.
· Coosa County had the highest infant mortality
rate with 26.3deaths per 1,000 births followed by
Greene County (23.3deaths), and Marengo County
(21.8deaths).
· AA/black mothers have twice the infant mortality
rate than white mothers.
*In Table 3.2, this rate is unstable due to low sample.
Table 3.2 – Infant Mortality, 2019
Count
Rate per
1,000 births
AL 449 7.7
U.S. 20,921 5.6
Public Health Districts
Northern 79 6.3
Northeastern 55 6.1
West Central 57 10.8
Jeerson 85 10.0
East Central 72 8.2
Southeastern 36 7.9
Southwestern 28 6.1
Mobile 37 6.9
Geographic Variation
N/A - -
Sex
N/A - -
Race/Ethnicity
White 191 5.6
AA/black 222 11.9
Hispanic 35 7.2
Household Income
N/A - -
Mother’s Age (in years)
15-17 9 9.3*
18-19 25 8.3
20-29 262 7.7
30-39 141 7.2
40+ 11 9.9
Mother’s Education
Less than high school 75 9.1
High school or GED 180 9.5
Some college 128 7.3
College graduate or higher 62 4.5
Low Birth Weight
Low birth weight is defined as live-born infants with birth
weight less than 5.5pounds (2,500 g), and it was the third
leading cause of infant morbidity and mortality in 2019:
2,5
· In AL, 1 out of every 10births were babies born
with low birth weights.
· East Central District had the highest percentage of
low birth weight infants in the state (12.5percent).
· AA/black mothers’ low birth weight prevalence
(16.3 percent) was higher than white mother’s
(7.8percent).
Table 3.3 – Low Birth Weight, 2019
Count %
AL 6,153 10.5
U.S. 311,245 8.3
Public Health Districts
Northern 1,163 9.3
Northeastern 788 8.8
West Central 601 11.4
Jeerson 928 10.9
East Central 1,095 12.5
Southeastern 474 10.4
Southwestern 458 9.9
Mobile 646 12.0
Geographic Variation
Rural 2,409 9.9
Urban 3,744 10.9
Sex
N/A - -
Race/Ethnicity
White 2,957 7.8
AA/black 3,042 16.3
Other 154 -
Mother’s Marital Status
Not married 3,768 14.4
Married 2,382 7.4
Mother’s Age (in years)
10-19 444 11.1
20-24 1,635 10.7

2020 ALABAMA STATE HEALTH ASSESSMENT
28
25-29 1,837 9.8
30-34 1,415 10.3
35+ 822 11.9
Mother’s Education
Less than high school 941 11.5
High school or GED 2,281 12.1
Some college 1,878 10.7
College graduate or higher 1,041 7.5
Teen Pregnancy
Teen pregnancy can be influenced by socio-economic
factors and the availability of social support programs. The
U.S. data includes females aged15-19 years old. For AL,
teenage pregnancy includes females aged 10-19years old.
6
· The Southeastern Public Health District had the
highest teen pregnancy rate with 15.8pregnancies
per 1,000females aged 10-19 years old.
· In 2019, Wilcox County had the highest teen
pregnancy rate with 32.1pregnancies per
1,000females aged 10-19 years old, followed by
Greene County at 25.8pregnancies.
· St.Clair County had the lowest teen pregnancy
rate, with 4.8pregnancies per 1,000females aged
10-19years old.
Table 3.4 – Teen Pregnancy, 2019
Count
Rate per 1,000
females aged
10-19 years old
AL 4,002 13.0
U.S. 171,674 16.7
Public Health Districts
Northern 865 12.9
Northeastern 595 11.7
West Central 416 14.8
Jeerson 449 10.9
East Central 583 12.9
Southeastern 369 15.8
Southwestern 352 14.0
Mobile 373 14.3
Geographic Variation
Rural 1,839 14.3
Urban 2,163 12.1
Sex
N/A - -
Race/Ethnicity
White 1,867 -
AA/black 1,615 -
Hispanic 484 -
Household Income
N/A - -
Mother’s Marital Status
Not married 3,583 -
Married 419 -
Mother’s Age (in years)
Under 19 4,002 13.0
Mother’s Education
Less than high school 1,763 -
High school or GED 1,816 -
Some college 417 -
College graduate or higher - -
A Closer Look into Pregnancy
Outcomes
AL rates of poor pregnancy outcomes are higher than
the national average, specifically for mothers who are
young, reside in rural areas, and identify with a minority
racial or ethnic group. The ADPH Bureau of Family Health
Services and community partner, the University of AL
at Birmingham, conducted the Title V Maternal and
Child Health (MCH) Block Grant Needs Assessment.
This process was used to identify where AL experiences
worse pregnancy outcomes and determine the best
approaches to promote health equity.
7
Maternal and Child Health Assessment
The workgroup met in early 2020 to align evidence-
based strategies with the identified needs from the MCH
population. A total of 1,247and community members
from across the state participated in surveys, focus
groups, and key informant interviews. The survey was
disseminated in online and paper versions for three
populations: family, providers, and adolescents. The
family survey comprised the largest representative group
(874 respondents) and respondents mostly identified as
female. The provider survey respondents were primary
healthcare providers representing specialties under
family medicine, OB-GYN, pediatrics, and adolescent
medicine. The adolescent survey had 86 respondents
between the ages of 12 and 26years old.
Additional qualitative information was collected
through interviews and focus groups. The key informant
interviews included 22 individuals who had expert
knowledge in one or more MCH populations (i.e.,
reproductive, maternal, neonatal, child, or adolescent
health) for AL. They were asked in their interview
to address strengths, barriers, and gaps/areas of

2020 ALABAMA STATE HEALTH ASSESSMENT
29
need for local, state, public, and private groups. The
stakeholder focus group had 147participants and
included underrepresented populations, such as women
with disabilities; people who identified as lesbian,
gay, bisexual, transgender, and queer (LGBTQ+); and
Spanish-speaking families.
The health issues addressed in the survey were perinatal/
infant, child, adolescent, children/youth with special
healthcare needs, and women/maternal domains.
In this section, the perinatal/infant health concerns
are discussed with eight broad themes identified
below. Several of these themes are further explored
with supporting quantitative statistics and qualitative
stakeholder feedback. Hale County was the only county
not represented by a survey respondent in these results.
The eight identified perinatal/infant health themes were:
· Pregnancy and parenthood for teens, young
families, and new parents.
· Safe sleep education.
· Breastfeeding.
· Infant mortality.
· Mental health.
· Reproductive and prenatal/perinatal care.
· Smoking, substance, and alcohol use.
· Health/dental care access, cost, and insurance.
Safe Sleep Education
According to the National Vital Statistics System, the
sleep-related sudden unexpected infant deaths rate
for AL was 175.8 per 100,000 live births between 2015 –
2019.
8
This statistic is higher than the national average of
90.1 deaths per 100,000 in 2019. The American Academy
of Pediatrics recommends infants should be placed to
sleep on their backs until 12 months of age during a Safe
to Sleep campaign that started in 1994.
9
According to the
Pregnancy Risk Assessment Monitoring System (PRAMS),
the U.S. average of infants placed on their backs was
79.6percent in 2019. In AL, the percentage of infants
placed on their backs has increased from 71.3percent in
2015 to 79.6 percent in 2019.
10
In response to determining care gaps, stakeholders
identified that some parents and caregivers struggled
to access essential supplies, such as cribs aligned
with safe sleep guidelines. Key informants noted a
need to recognize and appropriately address cultural
issues around co-sleeping. Survey respondents further
explained that having a baby in bed makes nighttime
feedings easier (66percent), having a baby sleep in bed
with family is preferable (52percent), and a baby will be
safe in bed with family (50 percent).
Breastfeeding
Breastfeeding is a natural source of nutrition and provides
a healthy start for infants. AL breastfeeding percentage is
lower than the national average, but it has been trending
better with 77.8percent of mothers able to breastfeed
in 2019, according PRAMS.
10
Additionally, community
members reported a perceived lack of support from
service providers and older family members to encourage
breastfeeding; they reported that mothers were
prompted to use baby formula more from these groups.
Lactation support was reported to be widely available for
most women after delivery, but long-term support was
unavailable in the community, especially for women who
did not qualify for WIC or other support services.
Infant Mortality
In AL, the infant mortality rate was 7.1 deaths per 1,000
live births in 2019, improving from the 2015CHA rate of
8.5 deaths per 1,000 live births.
4
Despite the statewide
decrease, AA/black mothers have twice the infant
mortality rate of White mothers (11.9 deaths compared
to 5.6 deaths per 1,000live births). Hispanic mothers
also have a high infant mortality rate (7.2 deaths per
1,000live births).
4
Furthermore, stakeholders felt that
limited access to consistent, high-quality care during the
full spectrum of birth (primary, prenatal, postnatal, and
mental health) might have contributed to the high infant
mortality rate in AL. Service providers and key informants
connected infant mortality to broader social and health
issues such as co-sleeping, poverty, systemic racism,
smoking, substance abuse, lack of access to family
planning services, and the mother’s overall health.
Reproductive and Prenatal/Perinatal Care
As discussed earlier in this section, obstetric services have
significantly decreased in rural areas. In the survey group,
23 percent of respondents reported they or someone in
their house did not have health insurance. Stakeholders
identified socioeconomic status, education, neighborhood
crime and safety, literacy, and housing as barriers to health
maintenance. Specific populations expressed unique
experiences when interacting with reproductive health
providers and care facilities. Women with disabilities
expressed concerns about the lack of accessibility and
accommodations during health appointments. This
population also identified the lack of education tailored
toward parenting with a disability. Spanish-speaking
populations identified that health education materials
in Spanish were either unavailable or poorly translated.
LGBTQ+ stakeholders reported that LGBTQ+ centered
care was dicult to find, noting that they were either
refused care, received poor care, misgendered by oce
sta, or had the added burden of educating their service
provider about their health considerations.

2020 ALABAMA STATE HEALTH ASSESSMENT
30
Data Sources
Table 3.1 – Inadequate Prenatal Care, 2019. ADPH,
Center for Health Statistics Birth and Death Files, 2019.
Data requested March 2021.
Figure 3.1 – A Picture of the Loss of Rural Obstetrical
Services in AL, 1980 to 2019. ADPH, Oce of Primary
Care and Rural Health, 2020. Data requested March 2021.
Table 3.2 – Infant Mortality, 2019. ADPH, Center
for Health Statistics Birth and Death Files, 2019. Data
requested March 2021.
Table 3.3 – Low Birth Weight, 2019. ADPH, Center
for Health Statistics Birth and Death Files, 2019. Data
requested March 2021.
Table 3.4 – Teen Pregnancy, 2019.
ADPH, Center
for Health Statistics Birth and Death Files, 2019. Data
requested March 2021.
Written Sources
1. CDC, Maternal and Infant Health, 2020.
2. ADPH, AL Perinatal Program, 2020.
3. Center for Medicare and Medicaid Services,
Improving Access to Maternal Healthcare in Rural
Communities, 2018.
4. ADPH, Center for Health Statistics, 2020.
5. WHO, Definitions for Newborns with Low Birth
Weight, 2006.
6. CDC, Social Determinants and Eliminating Disparities
in Teen Pregnancy, 2019.
7. ADPH MCH Services Block Grant, Comprehensive
Needs Assessment, 2020.
8. National Vital Statistic System, SIDS Statistics, 2019.
9. Academy of Pediatrics, Back to Sleep Campaign, 2021.
10. PRAMS, Prevalence of Selected MCH Indicators for
AL, 2019.
Community Resources
AL Abstinence Education Program
Location: Dallas County, AL
Type: Federally Funded Program
American Humane Association
Location: Washington, DC
Type: Federal Government Organization
AL Healthy Teen
Location: Montgomery County, AL
Type: State Governmental Program
AL Prison Birth Project
Location: Lee County, AL
Type: Non-profit Organization
AL Women’s Wellness Center
Location: Madison County, AL
Type: Health Center
Black Mamas Matter Alliance
Location: Atlanta, GA
Type: Advocacy Organization
CDC
Location: Atlanta, GA
Type: Federal Government Organization
Cheaha Women’s Health and Wellness
Location: Calhoun County, AL
Type: Health Center
Her Choice
Location: Jeerson County, AL
Type: Health Center
USDHHS
Oce of Adolescent Health
Location: Washington, DC
Type: Federal Government Organization
Kids Count
Location: Statewide
Type: Research Institution
The National Campaign to Prevent Teen and
Unplanned Pregnancy
Location: Nationwide
Type: Public Health Campaign

2020 ALABAMA STATE HEALTH ASSESSMENT
31
4. Nutrition and Physical Activity
Ranked AL’s Fourth Health Indicator
AL identified nutrition and physical activity (NPA) as the
fourth highest current health indicator. Most Americans
are sedentary and may engage in limited physical
activities. The American Heart Association
®
(AHA)
recommends about 30 minutes per day of moderate
physical activity, while the average American is either in a
sitting or lying position for about 18 hours a day.
1
NPA is combined in this report since they influence one
another. Insucient physical activity and poor nutrition
can result in weight gain and chronic health conditions.
2
The Body Mass Index (BMI) is one way to calculate body
fat by using weight divided by height, although other
calculations are more accurate. A BMI between 25.0-
29.9kg/m
2
is categorized as overweight, 30.0-34.9kg/
m
2
is categorized as obese, and over 35kg/m
2
is labeled
morbidly obese.
3
In 2019, over one-third of Alabamians
were considered at least obese.
2
Obesity is a risk factor
for hypertension, diabetes, heart disease, sleep apnea,
mental illness, and osteoarthritis.
Vulnerable Populations
AL is a very rural state, and many residents live in food
deserts, i.e., places with limited access to fresh fruits and
vegetables. The U.S. Department of Agriculture, (USDA)
defines food insecurity as a “lack of access to enough
food for an active, healthy life for all household members
and limited availability of nutritionally adequate foods.”
4
In AL, 16.1 percent overall and 20.8 percent of children
struggled with food insecurity in 2019.
5
Geographic Variation
AL has a state park system and green walkways in many
urban centers. ADPH partnered with the AL Department
of Transportation (ALDOT) to increase the number of
walkable communities, which includes more sidewalks and
slower speed limits to increase neighborhood mobility.
Topics Addressed for This Indicator are:
· Adults classified as obese.
· Adults consuming fruits less than once per day.
· Adults consuming vegetables less than once per day.
· Adults who participate in physical activity.
Highlights
The data presented for this information comes from BRFSS,
which includes self-reported measures. Data are also retrieved
from U.S. Census Bureau, AL Department of Conservation and
Natural Resources, and community partners:
· Over one-third (36.1 percent) of AL adults are obese.
· Regular exercise and physical activity reduce the
risk for many chronic diseases.
Risk Factors:
· Neighborhood safety.
· Physical pain.
· Education.
· Food access.
· Ages 45-65 years old.
· Overconsumption of beverages high in sugar content.
· Medications that contribute to weight gain.
Adults Classified as Obese
Obesity is defined as a BMI of more than 30kg/m
2
. This
medical condition can have associated adverse eects
on the body, such as CVD, stroke, diabetes, cancer, and
respiratory complications:
· In 2019, over one-third (36.1percent) of AL
adults were obese. The prevalence of obesity has
gradually increased over the past 20 years. The
national prevalence of obesity is 32.1percent. AL
had the seventh highest adult obesity prevalence
in the U.S. for 2019.
7
· According to BFRSS, 41.7 percent of Alabamians
with an annual household income less than
$15,000 were obese.
· AA/black individuals have a significantly higher
prevalence of obesity than white individuals.
Table 4.1 – Percentage of Adults
Classified as Obese, 2019
% 95% CI
AL 36.1 (34.6-37.7)
U.S. Median 32.1 -
Public Health Districts
Northern 34.7 (30.8-38.6)
Northeastern 34.4 (30.7-38.1)
West Central 41.1 (36.7-45.5)
Jeerson 35.1 (31.1-39.2)
East Central 34.7 (30.2-39.2)
Southeastern 38.8 (34.2-43.5)
Southwestern 38.2 (33.9-42.5)
Mobile 37.3 (33.0-41.6)
Geographic Variation
N/A - -
Sex
Male 36.0 (33.7-38.4)
Female 36.2 (34.2-38.3)

2020 ALABAMA STATE HEALTH ASSESSMENT
32
Race
White 32.5 (30.8-34.3)
AA/black 46.7 (43.4-49.9)
Household Income
Less than $15,000 41.7 (36.4-46.9)
$15,000-24,999 40.6 (36.5-44.7)
$25,000-34,999 38.9 (33.5-44.4)
$35,000-49,999 35.8 (31.3-40.2)
$50,000+ 33.2 (30.8-35.6)
Age (in years)
18-24 24.6 (19.0-30.2)
25-34 36.4 (32.0-40.8)
35-44 40.3 (36.2-44.4)
45-54 41.5 (37.8-45.2)
55-64 41.2 (38.0-44.4)
65+ 31.3 (29.0-33.6)
Education
Less than high school 43.4 (38.1-48.6)
High school or GED 34.4 (31.7-37.1)
Some college 37.3 (34.6-40.1)
College graduate or higher 32.0 (29.5-34.5)
Adults Consuming Vegetables Less
Than Once Per Day
Nutrition is an essential tool to keeping a healthy lifestyle.
Vegetable intake is an indicator of an overall healthy diet
and may reduce the risk of many chronic diseases:
· Among those least likely to consume at least
one serving of vegetables are lower educational
attainment and a low household income.
· Nutrition was assessed through self-reported
data on daily fruit and vegetable consumption.
Over 1 in every 5 AL adults (22.3percent)
consume vegetables less than once per day.
· College graduates are significantly more likely
to have consumed one or more servings of
vegetables, compared to Alabamians whose
highest level of education is high school graduate
or less.
· AL males and females had similar percentages of
consuming one or more servings of vegetables.
Table 4.2 – Percentage of Adults Consuming
Vegetables Less Than Once Per Day, 2019
% 95% CI
AL 22.3 (20.9-23.7)
U.S. Median 20.3 -
Public Health Districts
Northern 19.2 (15.8-22.5)
Northeastern 22.2 (18.8-25.7)
West Central 20.6 (16.9-24.4)
Jeerson 25.8 (22.0-30.0)
East Central 24.1 (19.5-28.7)
Southeastern 23.7 (19.3-28.1)
Southwestern 21.7 (18.1-25.3)
Mobile 23.4 (19.5-27.3)
Geographic Variation
N/A - -
Sex
Male 23.0 (20.8-25.1)
Female 21.7 (19.9-23.6)
Race
White 19.3 (17.7-20.9)
AA/black 31.4 (28.2-34.6)
Household Income
Less than 15,000 35.8 (30.5-41.2)
$15,000-24,999 26.4 (22.6-30.1)
$25,000-34,999 20.9 (15.7-26.1)
$35,000-49,999 22.5 (18.3-26.7)
$50,000+ 14.9 (13.0-16.8)
Age (in years)
18-24 27.1 (20.7-33.4)
25-34 20.1 (16.3-24.0)
35-44 18.6 (15.3-21.8)
45-54 20.8 (17.7-23.9)
55-64 23.5 (20.5-26.4)
65+ 24.2 (22.0-26.4)
Education
Less than high school 34.2 (28.9-39.4)
High school or GED 25.4 (22.8-27.9)
Some college 20.0 (17.5-22.5)
College graduate or higher 14.6 (12.7-16.4)
Adults Consuming Fruits Less Than
Once Per Day
Nutrition is an essential tool to keeping a healthy lifestyle.
Fruit intake is an indicator of an overall healthy diet and
may reduce the risk of many chronic diseases:
· According to BRFSS, nearly 1 in 2AL adults (46.1
percent) do not consume at least one fruit serving
each day, including 100percent fruit juices.
· College graduates are significantly more likely
to have consumed one or more servings of fruit,
compared to Alabamians whose highest level of
education is high school graduate or less.

2020 ALABAMA STATE HEALTH ASSESSMENT
33
· White populations have a similar consumption of
fruit servings compared to AA/black populations
(47.7 percent compared to 44.9 percent).
Table 4.3 – Percentage of Adults Consuming Fruit
Less Than Once Per Day, 2019
% 95% CI
AL 46.1 (44.5-47.8)
U.S. Median 39.3 -
Public Health Districts
Northern 45.3 (41.1-49.5)
Northeastern 45.7 (41.7-49.7)
West Central 47.8 (43.2-52.4)
Jeerson 43.8 (39.5-48.0)
East Central 45.6 (40.7-50.6)
Southeastern 51.4 (46.5-56.3)
Southwestern 46.2 (41.7-50.8)
Mobile 47.1 (42.5-51.6)
Geographic Variation
N/A - -
Sex
Male 47.7 (45.2-50.2)
Female 44.7 (42.6-46.9)
Race
White 47.4 (45.4-49.3)
AA/black 44.9 (41.6-48.2)
Household Income
Less than 15,000 50.1 (44.9-55.4)
$15,000-24,999 47.3 (42.8-51.7)
$25,000-34,999 47.1 (41.1-53.0)
$35,000-49,999 42.5 (37.7-47.2)
$50,000+ 44.3 (41.7-46.9)
Age (in years)
18-24 45.4 (38.6-52.3)
25-34 48.2 (43.4-53.0)
35-44 44.2 (40.0-48.4)
45-54 48.2 (44.4-51.9)
55-64 48.8 (45.5-52.1)
65+ 42.9 (40.4-45.4)
Education
Less than high school 49.0 (43.6-54.5)
High school or GED 48.4 (45.4-51.5)
Some college 47.3 (44.3-50.3)
College graduate or higher 39.5 (36.9-42.1)
Adults Who Participate in Physical
Activities
Regular exercise and other physical activities reduce
the risk for many chronic diseases. An individual may
experience barriers to physical activity due to their
environment and access to safe neighborhoods:
· Current physical activity guidelines recommend
adults participate in at least 150minutes of
moderate aerobic activity each week and
participate in muscle-strengthening exercises two
or more days per week.
· Conversely, 31.5 percent of AL adults did not meet
the recommended physical activity guidelines to
stay healthy and prevent chronic disease.
· Males are more likely to meet recommended
physical activity levels than females.
· Physical activity decreases with age. In young adults
18-24years old, 3 out of 4report meeting physical
activity standards. In adults over 65 years old, 3 out
of 5report meeting physical activity standards.
Table 4.4 – Percentage of Adults Who Reported
Doing Any Physical Activity in the Past Month, 2019
% 95% CI
AL 68.5
(67.0-70.0)
U.S. Median 73.7 -
Public Health Districts
Northern 69.7 (66.1-73.4)
Northeastern 70.3 (66.9-73.7)
West Central
66.1 (61.9-70.3)
Jeerson 69.9 (66.2-73.7)
East Central 67.8 (63.3-72.3)
Southeastern 63.3 (58.7-67.8)
Southwestern 66.9 (63.0-70.8)
Mobile 69.7 (65.8-73.6)
Geographic Variation
N/A - -
Sex
Male 71.7 (69.5-73.9)
Female 65.7 (63.7-67.6)
Race
White 69.0 (67.3-70.7)
AA/black 64.7 (61.7-67.7)
Household Income
Less than $15,000 57.3 (52.3-62.3)
$15,000-24,999 60.4 (56.3-64.5)
$25,000-34,999 63.2 (57.5-68.9)
$35,000-49,999 69.4 (65.2-73.5)
$50,000-74,999 79.0 (77.0-81.0)
Age(in years)
18-24 77.6 (72.3-82.9)
25-34 72.4 (68.1-76.6)
35-44 70.4 (66.6-74.2)
45-54 69.1 (65.7-72.5)

2020 ALABAMA STATE HEALTH ASSESSMENT
34
55-64 63.1 (59.8-66.3)
65+ 63.4 (61.1-65.8)
Education
Less than high school 57.1 (51.9-62.2)
High school or GED 63.2 (60.4-65.9)
Some college 70.5 (68.0-73.1)
College graduate or higher 80.4 (78.4-82.4)
A Closer Look into Nutrition and
Physical Activity
Each year, chronic diseases account for 70percent of
all deaths in the U.S. Obesity, physical inactivity, and
poor nutrition are modifiable behaviors that contribute
to chronic diseases, specifically heart disease, stroke,
diabetes, and cancer.
7
Vulnerable populations may have
diculties achieving recommended levels of physical
activity and accessing nutritionally dense foods. For
example, rural populations may have a longer commute
to grocery stores, parks, and recreation centers; thus, any
additional barriers in their physical and built environment
can lead to dierent levels of health risks, needs, and
outcomes compared to urban populations. In this section,
parks and quality food access were further explored for
their association to health outcomes of Alabamians.
Walk Score and Access to State Parks
Walking is a low-cost, low-impact physical activity to
maintain and improve health.
7
The AHA recommends
that adults get at least 30minutes of moderate-intensity
aerobic exercise 5 or more days a week, with strength
training activities at least 2days per week.
8
Only 68.5
percent of Alabamians met the reported physical activity
guidelines in 2019.
9
A walk score is based on the walking distance (under one
mile) to amenities such as stores, restaurants, and parks.
A good walk score is above 70 and indicates low car
dependence, multiple forms of available transportation,
and that most errands can be accomplished on foot.
10
The average walk score in AL’s higher population areas
was22 in 2019, indicating higher car dependence.
Homewood, AL, had the highest walk score, followed
by Birmingham and Tuscaloosa (41, 35,and 33,
respectively).
10
Rural areas did not receive a score, which
highlights pedestrian walkability concerns and the lack of
alternative forms of transportation. The score also does
not account for diverse populations such as children,
seniors, or people living with disabilities.
Parks may be a way for individuals in non-urban areas to
increase their physical activity in public spaces. Access
to parks, trails, greenways, and recreational centers
provides opportunities to support a more active lifestyle
and improve neighborhood safety.
11
AL state parks are
managed by the AL Department of Conservation and
Natural Resources. AL has 21 state parks that cover
approximately 48,000acres.
12
A park is more likely to be used if it is nearby and easy
to access.
11
Individuals deprived of green areas may be
deprived of physical activity. Most state parks are directly
outside urban centers where greenways, local parks, and
walkways also exist. Figure 4.1overlays the prevalence of
obesity with the 21 state park locations. The areas with
higher obesity rates are more rural and have fewer areas
of walk space. The West Central District has the highest
obesity rate in the state (41.1 percent in 2019).
Food Insecurity and Health Outcomes
A healthy, well-rounded diet includes 2 cups of fruit and
2.5 cups of vegetables every day.
13
Only 46.1percent of
Alabamians eat the recommended servings of fruit per
Figure 4.1 – This map examines the prevalence of
obesity and locations of the 21 state parks in AL. Source:
CDC Places, which combines information from BRFSS
and American Community Survey 2013-2017 datasets.
Lauderdale
Colbert
Franklin
Marion
Winston
Walker
Limestone
Lawrence
Morgan
Cullman
Madison
Jackson
34.4
33.4
33.1
36.9
38.0
36.0
36.0
37.4
38.9
36.4
39.1
37.0
34.0
33.4
36.1
35.0
36.3
34.8
36.6
38.0
40.9
37.1
36.1
35.9
38.7
32.7
34.0
41.9
40.4
45.6
45.6
44.1
38.7
40.4
41.0
35.0
39.1
32.1
46.0
38.3
45.8
40.7
37.6
36.6
41.2
42.1
43.2
37.7
37.6
36.0
43.0
43.4
36.0
34.9
40.5
34.9
36.9
29.7
35.4
35.8
42.2
44.6
45.3
45.8
36.6
42.9
34.5
Marshall
DeKalb
Cherokee
Etowah
Blount
St. Clair
Calhoun
Cleburne
Clay
Talladega
Randolph
Chambers
Tallapoosa
Coosa
Jeerson
Lamar
Fayette
Tuscaloosa
Bibb
Hale
Sumter
Perry
Dallas
Marengo
Choctaw
Washington
Clarke
Monroe
Conecuh
Butler
Crenshaw
Pike
Barbour
Henry
Dale
Coee
Geneva
Obesity
Houston
Covington
Escambia
Baldwin
Mobile
Wilcox
Lowndes
Montgomery
Autauga
Chilton
Elmore
Macon
Bullock
Russell
Lee
Greene
Pickens
Shelby
50.025.0

2020 ALABAMA STATE HEALTH ASSESSMENT
35
day, and 22.3 percent eat the recommended vegetables
per day. The availability and aordability of healthy foods
allows people to make healthier food choices.
14
The
ADPH NPA Division uses ongoing surveillance to develop
eective dietary interventions and to understand
the barriers Alabamians face to eating healthy foods
regularly. Food-related environmental factors influence
available food choices and diet quality, such as:
· Ongoing supply of healthy foods and food insecurity.
14
· Access to transportation to food diverse areas.
14
· Proximity to healthy food retailers.
14
· Food costs and grocery tax between food retail
providers.
14
· Convenience of purchasing and making healthy
meals.
14
USDA defines food insecurity as a periodic lack of
access to enough food for an active, healthy life for
all household members and limited availability of
nutritionally adequate foods.
15
AL’s food insecurity rate
was 16.1 percent in 2019, with an estimated 788,250
people who experienced food insecurity.
5
Additionally,
meal gaps refer to the population in between secure and
insecure. Every county had residents who did not qualify
for Federal Nutrition Assistance but still experienced
food insecurity. Nearly 1in 4children and 1 in 6 adults
experienced hunger regularly.
5
Another environmental factor is the convenience
of purchasing meals and access to food diverse
areas. Food deserts refer to a residential area with
no immediate access to quality foods that support a
healthy diet (greater than 1 mile for urban areas and
greater than 10 miles in rural areas).
16
Rural populations
may be experiencing insecurity due to living in a food
desert. In urban areas, residents often live close
to grocery stores compared to rural areas, where
multiple modes of transportation may be required to
access the closest grocery store.
16
Furthermore, 5.8
percent of rural households in AL do not have a car
compared to 4.4percent of urban households. Since
43.0percent of the population live in rural counties, lack
of transportation and the distance from grocery stores
negatively impacts food security for many Alabamians.
Five food banks serve and distribute food throughout
AL.
5
In 2019, the Community Food Bank of Central AL
completed a regional study to assess the general health,
living situation, nutrition knowledge, and experiences
with hunger and food pantries. The Central AL area
covers 12counties and feeds over 60,000 people at risk
of hunger per month. Eighty-two percent of the served
population reported running out of food and not having
enough money to buy more.
17
Financial constraints are the most reported reasons
for food insecurity. The average American household
spent $5,576.21 on food from home and restaurants
in 2019, which was 9.6 percent of their disposable
income.
18
Aordability and access vary by income level.
High-income areas are more likely to have access to
grocery stores and healthy food options. A high-income
household spent $13,987 on food, representing 8.0
percent of their income.
15,18
Low-income populations
spent an average of $4,400 on food, representing 36.0
percent of their disposable income.
18
In the Community
Food Bank study, 91percent of the served population
was unemployed, 62 percent were on disability support,
and 27percent were retired or unpaid caretakers. Over
80 percent of respondents made an income of less
than $20,000 per year. For those with limited financial
resources, respondents reported that fixed expenses
(e.g., housing and medication costs) are usually covered
first, leaving little for flexible expenses (e.g., food
budgets).
17
The served population had to make dicult
choices between food and other expenses.
The served population had to choose between:
· Food and medicine (73 percent).
17
· Food and utilities (62 percent).
17
· Food and transportation (54 percent).
17
· Food and rent/housing costs (42 percent).
17
· Food and educational expenses (17 percent).
17
Most of the served population bought the cheapest food
even if it was not the healthiest option (78percent).
Other strategies the population took to avoid hunger
included getting help from family or friends (58 percent),
buying food in dented or damaged packages to save
money (50percent), growing food in a garden (41
percent), and watered-down food or drinks to make them
last longer (28 percent). Unaddressed food insecurity
and poor diets lead to chronic illnesses such as heart
disease, diabetes, and obesity.
14
The served population
had a much higher prevalence of chronic diseases than
the national and state averages:
· The served population reported an 80.0 percent
high blood pressure prevalence compared to the
state average of 42.5 percent in 2019.
17,19
· The served population reported a 51.0 percent
high cholesterol prevalence compared to the
state average of 36.9 percent in 2019.
17,19
· The served population reported a 44.0 percent
diabetes prevalence compared to the state
average of 13.9 percent in 2019.
17,19

2020 ALABAMA STATE HEALTH ASSESSMENT
36
Data Sources
Table 4.1 – Percentage of Adults Classified as Obese,
2019. CDC, BRFSS, 2018-2019. Data requested March 2021.
Table 4.2 – Percentage of Adults Consuming
Vegetables Less Than Once Per Day, 2019. CDC,
BRFSS, 2018-2019. Data requested March 2021.
Table 4.3 – Percentage of Adults Consuming Fruit
Less Than Once Per Day, 2019. CDC, BRFSS, 2018-
2019. Data requested March 2021.
Table 4.4 – Percentage of Adults who Reported Doing
any Physical Activity in the Past Month, 2019. CDC,
BRFSS, 2018-2019. Data requested March 2021.
Written Sources
1. AHA, Recommendations for Physical Activity in
Adults, 2020.
2. CDC, Obesity, 2020.
3. CDC, Body Mass Index, 2020.
4. USDA, Food and Nutrition Service, 2019.
5. Feeding America, Food Insecurity in AL, 2019.
6. ADPH, Nutrition and Physical Activity, 2020.
7. America’s Health Rankings, AL Obesity, 2019.
8. CDC, Physical Activity Basics, 2021.
9. CDC BRFSS, Adults who Meet Physical Activity
Guidelines, 2019.
10. Walk Score, Walk Score Methodology, 2021.
11. CDC, Parks, Trails, and Health, 2014.
12. AL Department of Conservation and Natural
Resources, About AL State Parks, 2021.
13. USDA, Dietary Guidelines for Americans 2020-2025, 2020.
14. CDC, Healthy Food Environments: Improving Access
to Healthier Food, 2020.
15. USDA Economic Research Service, Food Access
Research Atlas, 2021.
16. USDA Economic Research Service, Food Deserts in
AL, 2020.
17. Community Food Bank of Central AL, Hunger in
Central AL, 2020.
18. USDA Economic Research Service, Consumer
Expenditure Survey, 2021.
19. CDC BRFSS, Chronic Disease Outcomes in AL, 2020.
Community Resources
AL Child Nutrition Program
Location: Statewide
Type: State Government Program
AL Cooperative Extension System
Location: Montgomery County, AL
Type: Nonprofit Organization
AL Oce of Minority Health
Location: Montgomery County, AL
Type: State Government Organization
AL Oce of Women’s Health
Location: Montgomery County, AL
Type: State Government Organization
AL State Parks Division
Location: Montgomery County, AL
Type: State Government Organization
Auburn Outdoor Adventures
Location: Lee County, AL
Type: Non-profit Organization
Community Supported Agriculture
Location: Etowah County, AL
Type: Non-profit Organization
Community Supported Agriculture
Location: Lauderdale County, AL
Type: Non-profit Organization
Farmers Market Authority
Location: Montgomery County, AL
Type: State Government Organization
Lakeshore Foundation
Location: Jeerson County, AL
Type: Non-profit Organization
National Center for Physical Activity and Disability
Location: Nationwide
Type: Federally Funded Program
National Physical Activity Plan
Location: Nationwide
Type: Federally Funded Program
Produce for Better Health Foundation
Location: Montgomery County, AL
Type: Nonprofit Organization
Scale Back AL
Location: Montgomery County, AL
Type: State Funded Program
Sweet Grown AL
Location: Montgomery County, AL
Type: Non-profit Organization
YMCA
Location: Nationwide
Type: Non-profit Organization

2020 ALABAMA STATE HEALTH ASSESSMENT
37
5. Social Determinants of Health
Ranked AL’s Fifth Health Indicator
Social determinants of health (SDOH) topics are a
collection of factors identified as the fifth highest
health indicator for AL. While SDOH are upstream
objectives influencing all health indicators in this SHA,
the community partners wanted to highlight and discuss
specific methods to create opportunities for AL residents.
According to Healthy People 2030, the five SDOH topics
are economic stability, education access and quality,
healthcare access and quality, neighborhood and built
environment, and social/community context.
1
SDOH diers from access to care for they are a more
permanent, societal structure that prevents adequate
health factors. They can aect a wide range of physical
health, mobility, and quality of life outcomes.
Vulnerable Populations
SDOH plays a significant role in AL’s citizens’ health,
well-being, and quality of life and contributes to health
disparities and inequities. Income disparities, education,
poverty, unemployment, food insecurity, housing, and
family social support services need to be addressed as a
system to build environments that contribute to wellness
and support opportunities for healthy choices.
1
Geographic Variation
While there are some lifestyle and behavioral choices,
each individual is located within a specific community
with local policies and government that impact how
they can access health opportunities. For example, AL is
primarily a rural state, which can create physical barriers
to care, and social stigmas can prevent individual’s
knowing or feeling comfortable accessing a service.
Topics Addressed for This Indicator are:
· AL Black Belt.
· Income disparities.
· Education and poverty.
· Unemployment rate.
· Food insecurity.
· Housing assistance.
· Family and social support.
· Social Vulnerability Index (SVI).
Highlights
Data is from collaborating state agencies such as the
ALDOL and ALSDE. Data are also retrieved from U.S.
Census Bureau, University of AL, and CDC Agency for
Toxic Substances and Disease Registry (ATSDR):
· According to USHUD, as of January 2019, it
was estimated 3,261 persons experienced
homelessness on any given day in AL.
· In 2019, 16.3 percent of AL households were
unable to provide adequate food for one or more
household members due to lack of resources
compared to the 12.3 percent in U.S.households.
2
Risk Factors:
· Rural areas.
· Low income housing.
· High school education attainment or below.
· Incarceration.
· Unemployment.
The Alabama Black Belt
SDOH can create disparities with care delivery and health
outcomes. One area in AL with a high SDOH burden is
called the Black Belt.
Once named for the color of its fertile soil and later for the
high percentage of AA/black residents, 11 states make up
the Black Belt throughout the southeast.
The AL Black Belt consists of 18counties: Barbour,
Bullock, Butler, Choctaw, Crenshaw, Dallas, Greene, Hale,
Lowndes, Macon, Marengo, Montgomery, Perry, Pickens,
Pike, Russell, Sumter, and Wilcox:
· In 2019, the AL Black Belt had a 40percent white
and 56percent AA/black population.
3
· In 2019, almost 1 in 4 residents lived below the
poverty rate (23.7percent).
3
· The per capita income in this region was $24,387.
3

2020 ALABAMA STATE HEALTH ASSESSMENT
38
Figure 5.1 – The AL Black Belt contains 18counties
(highlighted green on the map). Source: University of AL
in Tuscaloosa.
Lauderdale
Colbert
Franklin
Marion
Winston
Walker
Limestone
Lawrence
Morgan
Cullman
Madison
Jackson
Marshall
DeKalb
Cherokee
Etowah
Blount
St. Clair
Calhoun
Cleburne
Clay
Talladega
Randolph
Chambers
Tallapoosa
Coosa
Jeerson
Lamar
Fayette
Tuscaloosa
Bibb
Hale
Sumter
Perry
Dallas
Marengo
Choctaw
Washington
Clarke
Monroe
Conecuh
Butler
Crenshaw
Pike
Barbour
Henry
Dale
Coee
Geneva
Houston
Covington
Escambia
Baldwin
Mobile
Wilcox
Lowndes
Montgomery
Autauga
Chilton
Elmore
Macon
Bullock
Russell
Lee
Greene
Pickens
Shelby
Income Disparities
Income equality is how finances are distributed
throughout a population. About 15 percent of AL’s
population lives below the 200 percent poverty rate:
3
· In 2019, AL’s poorest counties were Dallas,
Perry, Greene, and Bullock, respectively. These
counties are located within the AL Black Belt.
· The average poverty rate is slightly higher for rural
areas at 18.4 percent compared to urban areas
at 16.1percent for 2019. Alabama households in
urban areas have per capita incomes that are
roughly $6,000 more per home.
3
· Madison and Shelby counties have the highest
per capita income.
Figure 5.2 – This map describes income variation
throughout AL. Source: U.S. Census Bureau.
Lauderdale
Colbert
Franklin
Marion
Winston
Walker
Limestone
Lawrence
Morgan
Cullman
Madison
Jackson
28,033
28,411
36,620
22,596
14,884
21,641
23,450
27,367
24,453
21,907
24,301
24,883
24,747
23,468
22,952
21,311
22,636
24,483
23,882
26,409
25,345
23,142
24,721
23,519
23,305
38,549
26,789
23,024
16,799
14,884
21,191
15,055
20,778
24,658
23,694
25,217
22,729
27,860
20,419
23,470
20,877
18,473
22,453
24,563
21,038
20,527
19,769
19,028
23,687
27,806
21,711
24,645
25,276
27,097
22,225
26,752
25,861
32,626
29,052
29,819
19,612
25,635
16,841
20,209
29,071
22,308
32,098
Marshall
DeKalb
Cherokee
Etowah
Blount
St. Clair
Calhoun
Cleburne
Clay
Talladega
Randolph
Chambers
Tallapoosa
Coosa
Jeerson
Lamar
Fayette
Tuscaloosa
Bibb
Hale
Sumter
Perry
Dallas
Marengo
Choctaw
Washington
Clarke
Monroe
Conecuh
Butler
Crenshaw
Pike
Barbour
Henry
Dale
Coee
Geneva
Per capita income
Houston
Covington
Escambia
Baldwin
Mobile
Wilcox
Lowndes
Montgomery
Autauga
Chilton
Elmore
Macon
Bullock
Russell
Lee
Greene
Pickens
Shelby
40,00014,000
Education and Poverty
Education is an indicator for chronic disease because it
helps understand employment options, income mobility,
and basic literacy.
4
For adults below the poverty status,
income was correlated with education level:
· Two out of every five people with less than a high
school education live below the federal poverty line.
· Approximately 17.6percent of individuals who
have an educational achievement of a high school
diploma or GED live below the poverty line.

2020 ALABAMA STATE HEALTH ASSESSMENT
39
Figure 5.3 – The distribution of poverty level by
education group. Source: ALSDE, 2018 and County
Health Rankings, 2019.
U.S. poverty
rate
Overall AL
poverty rate
Less than
9th grade
Less than
9th grade
Some
college
College
graduate
10.5%
15.5%
40.4%
17.6%
11.8%
4.5%
Unemployment Rate
Employment is another indicator for SDOH. Good
working conditions, employee benefits, and work
stability often contribute to wellness and support
opportunities for healthy choices.
5
The AL labor force is a way to determine perceived
economic stability:
· During the early Coronavirus Disease 2019
(COVID-19) pandemic, the unemployment rate
was 7.7percent (as of July 22, 2020).
6
· For 2019, the average unemployment rate was
3.0percent, with 67,883individuals out of work.
· In 2019, the unemployment rate in rural areas
was 4.6percent compared to urban areas with
4.3percent.
· Wilcox County had the highest unemployment
rate at 7.2percent in 2019.
·The Southwestern Public Health District had the
most counties with high unemployment rates.
Figure 5.4 – This map describes the percent of
unemployed throughout AL in 2019. Source: ALDOL.
Lauderdale
Colbert
Franklin
Marion
Winston
Walker
Limestone
Lawrence
Morgan
Cullman
Madison
Jackson
3.3
2.6
2.5
3.3
3.7
2.8
3.1
2.6
2.5
2.8
2.9
3.3
2.7
2.6
3.3
3.4
3.1
3.1
3.3
2.2
3.5
3.2
3.0
3.0
3.4
2.7
2.7
3.5
4.5
5.6
3.9
5.2
3.1
2.7
3.0
3.0
2.9
2.7
4.3
2.9
3.6
3.8
3.3
2.8
3.6
4.9
4.0
3.5
3.4
2.9
2.9
3.1
3.6
3.0
5.8
4.6
3.7
3.5
2.6
2.7
5.5
3.5
7.1
5.7
3.1
4.7
2.9
Marshall
DeKalb
Cherokee
Etowah
Blount
St. Clair
Calhoun
Cleburne
Clay
Talladega
Randolph
Chambers
Tallapoosa
Coosa
Jeerson
Lamar
Fayette
Tuscaloosa
Bibb
Hale
Sumter
Perry
Dallas
Marengo
Choctaw
Washington
Clarke
Monroe
Conecuh
Butler
Crenshaw
Pike
Barbour
Henry
Dale
Coee
Geneva
Unemployment
Houston
Covington
Escambia
Baldwin
Mobile
Wilcox
Lowndes
Montgomery
Autauga
Chilton
Elmore
Macon
Bullock
Russell
Lee
Greene
Pickens
Shelby
6.5%0.0%
Food Insecurity
Food insecurity is defined as “a household-level economic
and social condition of limited or uncertain access to
adequate food.”
7
Lacking constant access to food can lead
to binge eating, malnutrition, and mineral deficiencies.
In 2019, 16.3 percent of AL households were unable
to provide adequate food for one or more household
members due to lack of resources compared to the 12.3
percent in U.S. households.
2
This is a decrease from 2015
where it was 16.7percent in AL.
According to USDA, AL was the sixth largest food
insecure area in the U.S. in 2017-2019.
7
Food insecurity is
particularly high among:
· Low income households.
· Households with children, especially those with a
single parent.

2020 ALABAMA STATE HEALTH ASSESSMENT
40
· Single person dwelling homes.
· AA/black and Hispanic households.
Food insecurity was measured by Food Stamps or the
Supplemental Nutrition Assistance Program (SNAP)
utilization. In 2019, 14percent of households in AL
received Food Stamps/SNAP. The median income among
households that received food stamps was $18,515.
3
Figure 5.5 – This map describes the food insecurity
throughout AL by percentage of households SNAP
utilization. Source: U.S. Census Bureau.
Lauderdale
Colbert
Franklin
Marion
Winston
Walker
Limestone
Lawrence
Morgan
Cullman
Madison
Jackson
12.0
10.0
10.1
13.1
13.0
16.3
16.5
12.6
13.7
18.1
16.4
14.3
9.5
11.4
14.7
15.8
18.1
19.0
15.5
9.8
17.2
14.8
15.4
12.5
16.5
5.4
10.3
14.7
27.5
38.9
25.5
35.1
16.2
17.3
11.1
19.6
15.5
10.8
23.3
18.8
22.5
26.8
15.3
15.5
16.6
16.1
13.7
15.7
15.0
12.9
17.2
17.7
16.6
14.0
17.4
16.1
16.6
7.7
12.4
12.8
30.5
21.4
25.4
33.5
18.6
22.8
14.0
Marshall
DeKalb
Cherokee
Etowah
Blount
St. Clair
Calhoun
Cleburne
Clay
Talladega
Randolph
Chambers
Tallapoosa
Coosa
Jeerson
Lamar
Fayette
Tuscaloosa
Bibb
Hale
Sumter
Perry
Dallas
Marengo
Choctaw
Washington
Clarke
Monroe
Conecuh
Butler
Crenshaw
Pike
Barbour
Henry
Dale
Coee
Geneva
SNAP Utilization
Houston
Covington
Escambia
Baldwin
Mobile
Wilcox
Lowndes
Montgomery
Autauga
Chilton
Elmore
Macon
Bullock
Russell
Lee
Greene
Pickens
Shelby
40.0%0.0%
Housing Assistance
According to USHUD, as of January 2019, it was estimated
3,261persons experienced homelessness on any given
day in AL.
In Figure 5.6, the map shows a distribution of individuals
whose monthly mortgage is greater than 35.0 percent of
the household income.
· According to U.S. Census Bureau, 19.1percent
of AL households have over one-third of their
household income devoted to monthly mortgage
or rent payments in 2018.
· Perry County had the highest percentage with
an average 63.1percent of its population with
a mortgage higher than one-third their income
between 2015-2019.
8
· There was an average of 1,867,893households
between 2015-2019 with 31.2 percent of units
used for renting.
8
Federal Housing Assistance gives aid to seniors, children,
and people living with disabilities. The largest rental
assistance support is through housing choice vouchers
and public housing.
Figure 5.6 – This map describes the percentage
of homeowners with a high cost burden mortgage.
Source: U.S. Census Bureau.
Lauderdale
Colbert
Franklin
Marion
Winston
Walker
Limestone
Lawrence
Morgan
Cullman
Madison
Jackson
19.2
13.2
13.2
18.7
17.2
16.1
25.4
16.6
22.2
15.7
22.0
19.1
15.6
17.7
25.3
20.0
14.4
24.6
21.0
18.1
16.5
22.9
18.5
15.9
22.1
14.1
19.7
16.0
24.8
41.7
29.0
63.1
16.2
24.7
24.1
23.9
23.7
17.3
24.9
22.0
11.2
18.2
19.8
16.8
23.6
29.6
18.6
19.2
16.8
14.0
20.6
17.5
17.0
16.6
23.1
19.3
19.9
20.2
13.6
19.8
19.2
30.1
28.4
33.5
17.3
18.2
19.4
Marshall
DeKalb
Cherokee
Etowah
Blount
St. Clair
Calhoun
Cleburne
Clay
Talladega
Randolph
Chambers
Tallapoosa
Coosa
Jeerson
Lamar
Fayette
Tuscaloosa
Bibb
Hale
Sumter
Perry
Dallas
Marengo
Choctaw
Washington
Clarke
Monroe
Conecuh
Butler
Crenshaw
Pike
Barbour
Henry
Dale
Coee
Geneva
Percent
Houston
Covington
Escambia
Baldwin
Mobile
Wilcox
Lowndes
Montgomery
Autauga
Chilton
Elmore
Macon
Bullock
Russell
Lee
Greene
Pickens
Shelby
65.0%0.0%

2020 ALABAMA STATE HEALTH ASSESSMENT
41
Family and Social Support
Positive relationships at home, at work, and in the
community can help families find support and improve
their well-being. Social capital refers to the interpersonal
support and trust between other civic associations.
9
In Figure 5.7, the indicator for this section is the percentage
of single-parent household for children under 18 years old:
· Between 2015-2019, approximately 1 out of every
4 children (25.2 percent) lived in a single-parent
household in AL.
10
· Adults and children living in single-parent
households have a higher risk of stress and
adverse health outcomes.
9
Figure 5.7 – This map describes percentage of single-parent
households in each county. Source: U.S. Census Bureau.
Lauderdale
Colbert
Franklin
Marion
Winston
Walker
Limestone
Lawrence
Morgan
Cullman
Madison
Jackson
20.2
19.3
23.9
20.4
23.2
22.6
19.0
22.4
22.4
18.3
12.7
25.4
18.6
19.5
25.9
22.7
18.8
17.8
19.4
14.4
23.3
11.2
20.3
33.8
30.3
14.6
29.6
26.0
44.1
39.0
28.8
39.0
19.5
23.2
15.5
29.0
25.7
23.0
35.6
32.7
57.3
33.7
34.3
24.7
29.4
29.6
18.6
27.2
24.2
27.4
23.4
23.2
18.8
29.4
27.2
23.8
28.1
18.0
19.9
19.6
41.3
30.7
33.3
44.7
34.7
24.3
30.0
Marshall
DeKalb
Cherokee
Etowah
Blount
St. Clair
Calhoun
Cleburne
Clay
Talladega
Randolph
Chambers
Tallapoosa
Coosa
Jeerson
Lamar
Fayette
Tuscaloosa
Bibb
Hale
Sumter
Perry
Dallas
Marengo
Choctaw
Washington
Clarke
Monroe
Conecuh
Butler
Crenshaw
Pike
Barbour
Henry
Dale
Coee
Geneva
Percent
Houston
Covington
Escambia
Baldwin
Mobile
Wilcox
Lowndes
Montgomery
Autauga
Chilton
Elmore
Macon
Bullock
Russell
Lee
Greene
Pickens
Shelby
60.0%0.0%
Social Vulnerability Index
Geospatial determinants of health include
neighborhood infrastructures and how a person’s
community aects an individual. CDC created a risk
score based on multiple environments, including
natural, built, population connectivity, social/
behavioral, and health policy.
11
This can provide crucial
information for emergency preparedness and address
endemic SDOHs in a community.
The 15 social factors are calculated within a score that
combines the following factors: poverty, unemployment,
income, education status, lack of vehicle access, multi-
unit structures, mobile housing units, crowded housing,
group quarters, adults living with disabilities, children,
older population, single- parent households, minority
groups, and primary language other than English.
11
The scores are ranked from 0 to 1, where a score closer to
1 indicates an area of high vulnerability:
· The West Central Public Health District had a
higher average of SVIs for 2018.
Figure 5.8 – This map describes the proportion of
social vulnerability on a scale from 0 to 1. Source: CDC
ATSDR Community Engagement.
Lauderdale
Colbert
Franklin
Marion
Winston
Walker
Limestone
Lawrence
Morgan
Cullman
Madison
Jackson
0.08
0.17
0.06
0.26
0.05
0.68
0.09
0.38
0.41
0.65
0.14
0.29
0.12
0.20
0.56
0.48
0.36
0.44
0.62
0.03
0.64
0.35
0.47
0.23
0.71
0.00
0.30
0.86
0.89
1.00
0.95
0.98
0.24
0.55
0.27
0.73
0.39
0.33
0.85
0.82
0.88
0.97
0.79
0.42
0.77
0.61
0.74
0.76
0.53
0.15
0.67
0.50
0.21
0.32
0.80
0.58
0.52
0.02
0.18
0.11
0.92
0.59
0.94
0.91
0.70
0.83
0.45
Marshall
DeKalb
Cherokee
Etowah
Blount
St. Clair
Calhoun
Cleburne
Clay
Talladega
Randolph
Chambers
Tallapoosa
Coosa
Jeerson
Lamar
Fayette
Tuscaloosa
Bibb
Hale
Sumter
Perry
Dallas
Marengo
Choctaw
Washington
Clarke
Monroe
Conecuh
Butler
Crenshaw
Pike
Barbour
Henry
Dale
Coee
Geneva
SVI Index
Houston
Covington
Escambia
Baldwin
Mobile
Wilcox
Lowndes
Montgomery
Autauga
Chilton
Elmore
Macon
Bullock
Russell
Lee
Greene
Pickens
Shelby
1.0%0.0%

2020 ALABAMA STATE HEALTH ASSESSMENT
42
Data Sources
Figure 5.1 – AL Black Belt Counties. University of AL in
Tuscaloosa, 2019. Data requested March 2021.
Figure 5.2 – AL Per Capita Income, 2019. U.S. Census
Bureau, American Community Survey 1-Year Estimates,
Quick Facts Table County Level V2019, 2019. Data
requested December 2020.
Figure 5.3 – AL Below-Poverty Status by Education
Level, 2019. ALSDE, 2018 and County Health Rankings,
2019. Data requested July 2020.
Figure 5.4 – Unemployment Rate, 2019. ALDOL, 2019.
Data requested July 2020.
Figure 5.5 – Food Stamp/SNAP Utilization, 2015-
2019. U.S. Census Bureau, American Community Survey
5-Year Estimates Selected Social Characteristics Table
DP03, 2019. Data requested December 2020.
Figure 5.6 – Monthly Mortgage Greater than 35
Percent of Income, 2015-2019. U.S. Census Bureau,
American Community Survey, 5-Year Estimates Selected
Housing Characteristics DP04, 2019. Data requested
December 2020
Figure 5.7 – Children in Single Parent Households,
2019. U.S. Census Bureau, American Community Survey
5-Year Estimates Selected Social Characteristics Table
DP02, 2019. Data requested December 2020.
Figure 5.8 – SVI, 2018. CDC, ATSDR Community
Engagement. Data requested March 2021.
Written Sources
1. Healthy People 2030, SDOH, 2020.
2. AL Food Bank Association, Hunger in AL, 2019.
3. U.S. Census Data, American Community Survey, 1
Year Estimate Quick Tables V2019, 2019.
4. Healthy People 2030, Education, Access, and
Quality, 2020.
5. Healthy People 2030, Employment, 2020.
6. U.S. Department of Labor, Bureau of Labor Statistics,
2020.
7. U.S. Census Data, American Community Survey, KIDS
COUNT Data Center, 2020.
8. U.S. Census Data, American Community Survey, 5
Year Estimate Table DP02, 2019.
9. CDC, Adverse Childhood Experiences Risk and
Protective Factors, 2020.
10. U.S. Census Data, American Community Survey, 5
Year Estimate Table DP04, 2019.
11. CDC, SVI, 2020.
Community Resources
Action for Healthy Kids
Location: Montgomery County, AL
Type: Advocacy Program
Adult Vocational Rehabilitation
Location: Etowah County, AL
Type: Educational Facility
AL Community Foundation
Location: Montgomery County, AL
Type: Nonprofit Organization
AL Possible
Location: Statewide
Type: Non-profit Organization
Continuums of Care
Location: Statewide
Type: Federal Program
Dothan Rescue Mission
Location: Houston County, AL
Type: Homeless Shelter
East AL United Way
Location: Montgomery County, AL
Type: Nonprofit Organization
FQHC
Location: Statewide
Type: Medical Centers
Firehouse Ministries
Location: Jeerson County, AL
Type: Homeless Shelter
Habitat for Humanity
Location: Montgomery County, AL
Type: Nonprofit Organization
Healthy People 2030
Location: Nationwide
Type: Advocacy Program
USDHHS
Location: Washington, DC
Type: Federal Government

2020 ALABAMA STATE HEALTH ASSESSMENT
43
6. Sexually Transmitted Infections
Ranked AL’s Sixth Health Indicator
STIs are ranked sixth in priority for AL’s health indicators.
Reproductive health is the focal point for interventions
involving sexual safety, maternal health, and child health.
Many STIs have mandatory reporting requirements in
AL, which allows ADPH to investigate areas within the
state with high rates of chlamydia, gonorrhea, human
immunodeficiency virus (HIV), and syphilis. STIs are spread
through sexual contact and bodily fluids. Condom use and
communication with partners about possible exposures
are highly recommended to prevent the spread of STIs.
1
The number of new HIV infections continues to outweigh
the number of deaths among people diagnosed with HIV,
largely due to the success and widespread utilization of
highly active antiretroviral therapy in 1995. About 1.2 million
people are living with HIV in the U.S. In 2019, 15.2percent of
new HIV diagnoses were in the south. There were 635 newly
diagnosed HIV infections reported among AL residents in
2019. CDC estimated that 13 percent of persons infected
with HIV in the U.S. were unaware of their status.
2
Applying
this knowledge to the 2019state prevalence, estimates
suggest an additional 2,517 AL residents may be infected
with HIV and are unaware of their status.
It is important for anyone engaging in sexual activity
to get tested frequently to protect their own and their
partners’ health. Vaccinations for hepatitis B and human
papillomavirus (HPV) are good primary preventions.
Vulnerable Populations
Pregnant women can become infected with STIs and
should get a screening during their routine medical care.
A positive screening can pose a serious risk to their
pregnancy, and the baby may become infected while
pregnant. Syphilis during pregnancy is increasing across
the U.S., and can cause miscarriage, prematurity, low
birth weight, and severe anemia. CDC recommends
all expecting mothers to be tested for all STIs by the
first prenatal visit. If positive, health practitioners can
recommend a safe form of treatment for their patients.
Individuals who have multiple partners and people who
identify as LGBTQ+ have an increased risk of having an
STI, so CDC recommends getting screened once a year.
2
Geographic Variation
STIs can occur anywhere there is bodily fluid exchange.
Stigma and poor sexual education are the primary reasons
for high transmission post infection. Areas with high STI
rates are near urban centers and within populations
experiencing limited access to clinical treatments.
Topics Addressed for This Indicator are:
· Syphilis incidence.
· Gonorrhea incidence.
· Chlamydia incidence.
· HIV incidence.
Highlights
Data are retrieved from the ADPH Oce of Sexually
Transmitted Diseases (STDs) and the Oce of HIV
Prevention and Care:
· STI rates have been increasing every year,
especially in person ages 15-24 years old.
· AA/black individuals were nearly three times
more likely to be diagnosed with HIV than white
individuals.
Risk Factors:
· Multiple sexual partners.
· Previous STIs.
· Commercial sex work.
· Intravenous drug use.
· Unprotected sex.
· Dating violence and sexual assault.
Syphilis Incidence
Syphilis is caused by bacterium Treponema pallidum and
is one of the most reported STIs in both AL and the U.S.:
· The Syphilis rate for males is three times higher
than females in AL.
· The rates were highest in 15-24years old
in 2019, increasing by 21.8 new cases per
100,000persons since 2018.
· AA/black persons with syphilis have case rates
nearly six times higher than white persons with
syphilis in 2019 (75.2 new cases compared to 12.7
new cases per 100,000 persons).
· Hispanic persons with syphilis doubled by case
and rate from 2018 to 2019.

2020 ALABAMA STATE HEALTH ASSESSMENT
44
Table 6.1 – Syphilis Cases, 2018–2019
2018
Count, Rate per
100,000
2019
Count, Rate per
100,000
AL 1,243 25.4 1,483 30.2
U.S. 115,062 35.2 129,813 39.7
Public Health Districts
Northern 214 19.6 288 26.4
Northeastern 83 10.3 108 13.3
West Central 87 20.1 143 33.0
Jeerson 293 44.5 257 39.0
East Central 270 38.1 343 48.4
Southeastern 106 28.0 98 25.9
Southwestern 45 10.9 46 11.2
Mobile 145 35.1 200 48.4
Geographic Variation
N/A - - - -
Sex
Female 290 11.4 392 15.5
Male 953 40.2 1,091 46.0
Race
AA/black 830 64.0 976 75.2
Hispanic or Latino 26 11.6 53 23.7
White 339 10.6 405 12.7
Household Income
N/A - - - -
Age (in years)
15-24 369 58.0 507 79.8
25-34 476 73.5 483 74.6
35-44 196 33.0 269 45.3
45-54 123 19.9 112 18.2
55-64 61 9.3 75 11.4
65+ 17 2.0 9 1.1
Education
N/A - - - -
Gonorrhea Incidence
Gonorrhea, caused by the bacterium Neisseria gonorrhoeae,
is the second most reported STI in both AL and the U.S.:
· The Northeastern Public Health District had the
lowest case rate, while Jeerson County had the
highest rate in 2019.
· Gonorrhea rates are higher in males compared
to females (304.4 new cases compared to 261.0
new cases per 100,000 persons).
· The highest rates of infection are between
ages 15-24 years old in 2019 (1,143.8cases per
100,000persons).
Table 6.2 – Gonorrhea Cases, 2018–2019
2018
Count, Rate per
100,000
2019 Count,
Rate per
100,000
AL 12,954 264.2 13,844 282.3
U.S. 583,405 179.1 616,392 188.4
Public Health Districts
Northern 2,329 217.7 2,270 259.0
Northeastern 1,343 166.7 1,548 191.2
West Central 1,081 248.9 1,082 249.4
Jeerson 2,819 427.6 2,428 368.7
East Central 2,459 347.9 2,461 347.5
Southeastern 1,097 290.0 1,252 330.4
Southwestern 651 160.1 792 192.4
Mobile 1,165 281.4 1,511 365.7
Geographic Variation
N/A - - - -
Sex
Female 6,262 247.2 6,613 261.0
Male 6,655 280.9 7,213 304.4
Race
AA/black 6,222 479.4 6,386 492.1
Hispanic or Latino 133 59.6 117 52.4
White 1,820 56.9 2,007 62.7
Household Income
N/A - - - -
Age (in years)
15-24 7,082 1,114.0 7,271 1,143.8
25-34 3,909 604.0 4,375 676.0
35-44 1,242 209.3 1,415 238.5
45-54 408 66.2 472 76.5
55-64 150 22.8 185 28.1
65+ 39 4.6 38 4.5
Education
N/A - - - -
Chlamydia Incidence
Chlamydia, caused by the bacterium chlamydia
trachomatis, is the most reported STI in both AL and the U.S.:
· AL ranks eighth nationally in chlamydia
transmission, which is an improvement from its
previous rank of third in 2014. Within the state,
chlamydia cases are still on the rise.
· AA/blacks have the higher rates of disease
compared to white (908.6 new cases compared
to 124.7 new cases per 100,000 persons).
· Females have higher rates of disease compared
to males.

2020 ALABAMA STATE HEALTH ASSESSMENT
45
· Young adults aged 15-24 years old have the
highest rates of disease compared to other age
groups (3,255.6 new cases per 100,000 persons).
Table 6.3 – Chlamydia Cases, 2018–2019
2018
Count, Rate per
100,000
2019
Count, Rate per
100,000
AL 29,396 599.5 30,042 612.7
U.S. 1.758M 537.5 1.809M 552.8
Public Health Districts
Northern 4,911 459.1 5,479 512.2
Northeastern 3,163 392.5 3,674 453.9
West Central 3,070 706.8 2,713 625.3
Jeerson 5,298 803.7 4,659 707.4
East Central 5,602 792.6 5,437 767.7
Southeastern 2,434 643.3 2,567 677.4
Southwestern 1,867 459.0 2,153 523.0
Mobile 3,029 731.7 3,359 812.9
Geographic Variation
N/A - - - -
Sex
Female 20,285 800.6 20,562 811.6
Male 9,013 380.4 9,418 397.5
Race
AA/black 12,157 936.8 11,791 908.6
Hispanic or Latino 556 249.0 651 291.6
White 3,997 124.9 3,992 124.7
Household Income
N/A - - - -
Age (in years)
15-24 20,677 3,252.6 20,696 3,255.6
25-34 6,668 1,030.2 7,064 1,091.4
35-44 1,244 209.7 1,456 245.4
45-54 347 56.3 407 66.0
55-64 103 15.7 107 16.3
65+ 30 3.5 24 2.8
Education
N/A - - - -
Human Immunodeficiency Virus
Incidence
While male-to-male sexual activity continues to be the
predominant mode of exposure for HIV infection, heterosexual
contact is the second most common mode of exposure.
There are persons living with HIV in every county in AL, and the
number continues to increase each year. In 2019, Jeerson
County accounted for 20 percent of all new cases (128 cases).
AL is experiencing a downward shift in the age
distribution of newly diagnosed HIV infections as young
adults (ages 25-34 years old) emerged as the most
aected age group:
· At the end of 2019, 14,345 AL residents were
known to be living with HIV and 6,432 residents
(44.8percent) had progressed to acquired
immunodeficiency syndrome (AIDS).
· Rural AL HIV incidence rate is 5.2cases per
100,000persons. Urban AL HIV incidence rate
is 16.9cases per 100,000 persons. Some cases
could not be confirmed to an individual’s county,
but the case was confirmed within the district.
· AA/blacks continue to be disproportionately
aected by HIV in AL. Nearly 72percent of newly
diagnosed HIV infections occurred in AA/blacks
in 2019.
· AA/black individuals were nearly 3times more likely
to be diagnosed with HIV than white individuals
(456compared to 152 individuals, respectively).
Table 6.4 – HIV Incidence, 2019
Count Rate (per 100,000)
AL 635 13.1
U.S. 36,801 12.6
Public Health Districts
Northern 80 7.5
Northeastern 39 4.8
West Central 55 12.7
Jeerson 128 19.4
East Central 159 22.5
Southeastern 45 11.9
Southwestern 23 5.7
Mobile 106 25.6
Geographic Variation
Rural 110 5.2
Urban 472 16.9
Sex
Female 136 5.4
Male 499 21.1
Race
AA/black 456 35.1
White 152 4.7
Multi-racial 12 13.8
Household Income
N/A - -
Age (in years)
15-24 166 26.1
25-34 220 34.0
35-44 119 20.1

2020 ALABAMA STATE HEALTH ASSESSMENT
46
45-54 75 12.2
55-64 46 7.0
65+ 12 1.4
Education
N/A - -
A Closer Look into Sexually
Transmitted Infections
HIV aects over one million people in the U.S. per year.
In AL, there were 13,723current diagnosed cases of HIV
and 635 newly diagnosed HIV infections in 2019. About
65percent of individuals living with HIV were virally
suppressed.
2
Early detection and follow-up of an HIV-
positive result can reduce patient mortality and prevent
future transmissions. The Oce of HIV Prevention and
Care partnered with a variety of community partners,
including AIDS service organizations, community-based
organizations, and faith-based organizations, to create
the End HIV AL (EHA) committee.
3
End HIV Assessment
The purpose of the EHA committee is to identify
community members and develop a plan to reduce new
HIV infections in AL. Provider interviews, focus groups,
surveys, and community meetings helped shape the
EHA team’s work. Listening sessions with community
members were critical to the process. The sessions
prompted the workgroup to:
· Convene focus groups in rural areas throughout
the state.
· Set up recruitment booths at health fairs and
conferences.
· Gain access to college campuses and other
public institutions.
· Establish an EHA planning group.
Through the EHA committee’s direction, the team
expanded its reach to rural areas by providing a telephone
interview survey and an online focus group. The finalized
community needs survey tailored sensitive questions
towards SDOHs and allowed for a deeper understanding
of the impact of health issues for persons living with HIV.
The prioritized population for this community health
assessment included persons who identify as transgender;
cisgender women, especially AA/black women; people
who inject drugs; and gay and bisexual men (GBM) and
other men who have sex with men, especially AA/black
and Hispanic/Latinx GBM. Other vulnerable populations
included clients with unstable housing or homelessness.
The committee also wanted to include underrepresented
populations such as Hispanic/Latinx individuals; therefore,
a translator was hired to attend program meetings and
interpret documents, surveys, and emails.
Quantitative data responses were collected through an
online survey between March and July 2020 to address
the disparities in HIV incidence. Over 400 individuals
participated in the process. Four overarching themes were
identified as barriers to HIV care: stigma, education, lack of
resources, and cultural considerations. These were further
explained to include fear of discrimination, lack of insurance,
lack of transportation to services, and inadequate income.
The prioritized population identified six needs for HIV
care listed below. This section provides further discussion
on testing sites and partner services with supporting
quantitative statistics and qualitative stakeholder feedback.
The identified needs in the priority population are:
· HIV testing.
· STI testing.
· Hepatitis C testing.
· Partner services.
· Health education.
· Prevention services.
HIV and STI Testing Sites
Education about safe sexual health practices (including
regular condom use, regular STI testing, and open
communication with partners) is one preventative
measure to spreading STIs. Provider interviews
highlighted reoccurring themes about improving access
to accurate, culturally appropriate, and timely sexual
health information. Additionally, regular testing can also
prevent unknowingly spreading disease. Since STIs can
increase the risk of spreading HIV, surveillance data can
inform the public about high-risk sexual behavior.
2
In the
2019 ADPH STI report:
· There were 319 chlamydia cases co-infected
with HIV.
4
· There were 331 gonorrhea cases co-infected
with HIV.
4
· There were136 primary and secondary syphilis
cases were co-infected with HIV.
4
· Chlamydia was the most common STI in 2019.
The most vulnerable populations were AA/black
persons and individuals aged 15-24 years old.
4
HIV and STI testing sites can be located at health
departments and some medical oces. While most
individuals living with HIV live in more urban counties,

2020 ALABAMA STATE HEALTH ASSESSMENT
47
rural counties often are medical care deserts without
adequate access to standard medical care or specialized
HIV care.
3
In 2010, ADPH increased the number of
location sites for disproportionate populations aected
by HIV, such as people who use injection drugs, AA/black
GBM, and Hispanic/Latinx GBM. Survey participants
reported that the community is still unsure where HIV
and STI testing sites are located, noting that rural areas
are underserved by testing sites.
Partner Services
Of the 637 individuals living with HIV linked to care in
2019,77 percent were linked within 30days of care. The
Northeastern Public Health District had the highest
percent link to care (87 percent).
3
Community members
reported that most individuals received an appointment
or were directed to locations that suited their needs:
· An appointment with a health department or
clinic was given to 45 individuals.
· Information on where to receive HIV care was
given to 45 individuals.
· Clinical sta or peers went with 11 individuals to
their appointment.
Cost of services was a significant barrier to care among
survey respondents (59.8 percent), noting that almost
40 percent of individuals living with HIV had no insurance
at the time of diagnosis. The insurance status of Spanish-
speaking clients improved over the interval between
diagnosis and survey completion (72.0 percent to 91.7
percent). Additionally, Spanish-speaking clients found
that access was less accommodating than English-
speaking clients, specifically for insurance assistance
(64.4percent and 36.8 percent) and emergency financial
assistance (64.3 percent and 0.0 percent).
3
Data Sources
Table 6.1 – Syphilis Cases, 2018-2019. ADPH, Division
of Sexually Transmitted Diseases (STD) Prevention and
Control, 2019. Data requested July 2021.
Table 6.2 – Gonorrhea Cases, 2018-2019. ADPH,
Division of STD Prevention and Control, 2019. Data
requested July 2021.
Table 6.3 – Chlamydia Cases, 2018-2019. ADPH,
Division of STD Prevention and Control, 2019. Data
requested July 2021.
Table 6.4 – HIV Incidence, 2019. ADPH, Division of STD
Prevention and Control, 2019. Data requested July 2021.
Written Sources
1. ADPH, Division of STD Prevention and Control, 2019.
2. CDC, STIs and HIV Fact Sheet, 2020.
3. ADPH Oce of HIV Prevention and Care, Ending the
HIV Epidemic, 2020.
4. ADPH Division of STD Prevention and Control, STD
Annual Report 2019, 2020.
Community Resources
1917 Clinic
Location: Jeerson County, AL
Type: Non-profit Organization
Act Against AIDS
Location: Nationwide
Type: CDC Program
AL Health Education Center
Location: Statewide
Type: Education Center
AIDS AL
Location: Washington, DC
Type: Non-profit Organization
Birmingham AIDS Organization
Location: Jeerson County, AL
Type: Non-profit Organization
CDC
Location: Atlanta, GA
Type: Federal Government Organization
Choices Pregnancy Clinic
Location: Tuscaloosa County, AL
Type: Health Clinic Facility
Housing Opportunities for Persons with AIDS
Location: Statewide
Type: Federally Funded Program
Magic City Acceptance Center
Location: Jeerson County, AL
Type: Non-profit Organization
National HIV, STD, and Viral Hepatitis Testing Resources
Location: Nationwide
Type: CDC Program
Planned Parenthood
Location: Mobile County, AL
Type: Non-profit Organization
Thrive AL
Location: Madison County, AL
Type: Health Clinic Facility

2020 ALABAMA STATE HEALTH ASSESSMENT
48
7. Geriatrics
Ranked AL’s Seventh Health Indicator
Geriatrics is a specialty that focuses on the health of
individuals over 65 years old. With the elderly population
rising nationally, health concerns regarding geriatrics
increased from the tenth to the seventh leading health
indicator in AL. The Baby Boom generation has the
largest population influx in the history of the U.S. As
subsequent generations enter retirement age, it is
projected that almost 25percent of the U.S. population
will be 65 years or older by 2060.
1
Elderly people often
need more health resources and spend more of their
income on healthcare.
2
The aging population can experience numerous
health issues due to multiple chronic diseases. A
multigenerational health plan helps older adults
remain at home, maintain control of their health, and
continue their routines without much interruption.
Elderly populations with regular connections to their
family consistently report much less depression, better
physical health, and higher life satisfaction.
3
Vulnerable Populations
Elderly citizens who need extra support may need
additional care by an in-home nurse or relocated
to a nursing home. There may be additional factors
preventing a person from getting access to care, such as
the inability to drive, forgetting their scheduled provider
appointment(s), and having mobility problems.
2,3
Geographic Variation
Nursing homes, assisted living facilities, and other
long-term care facilities are the primary location for
elderly individuals who cannot independently take care
of themselves. However, rurality still plays a role in the
number of long-term care facilities open and the doctors’
availability for routine specialized care for chronic
disease management.
Topics Addressed for This Indicator are:
· Adult abuse cases.
· Alzheimer’s disease among Medicare recipients.
Highlights
Data are retrieved from the AL Department of Human
Resources (DHR) and the Centers for Medicare and Medicaid.
· Alzheimer’s disease is the sixth leading cause of
death in AL with 54.2 deaths per 100,000people
in 2019.
· In AL, rural areas have a higher rate of adult
abuse cases (19.2cases per 10,000persons),
than urban areas for 2019 (17.3cases per
10,000persons).
Risk Factors:
· Age.
· Family history.
· High blood pressure.
· Stroke history.
· Low physical activity.
· Geography/rural residents.
· Social isolation.
· Unable to provide self-care.
Adult Abuse Cases
The risk for elder abuse occurs more if a patient cannot
take care of themselves, has a cognitive disorder (such as
dementia and Alzheimer’s disease), or is socially isolated:
· In 2019, 8,789adult abuse, neglect, and exploitation
cases were opened and investigated by the DHR.
The most impacted group was white females.
· The top five counties with the highest case
numbers were Jeerson, Mobile, Houston,
Montgomery, and Madison.
· The Southeastern Public Health District had the
highest rate of adult abuse per 10,000persons
in2019.
· In AL, rural areas have a higher rate of adult
abuse cases (19.2cases per 10,000persons),
than urban areas for 2019 (17.3cases per
10,000persons).
The demographic data (sex, race/ ethnicity) pertains to
the number of clients. The geographic data (public health
districts and geographic variation) refers to the number
of cases.
Table 7.1 – Adult Abuse Cases, 2018-2019
2018
Count, Rate
per 10,000
2019
Count, Rate
per 10,000
AL 8,862 24.1 8,789 23.0
U.S. - - - -
Public Health Districts
Northern 1,971 19.0 1,799 17.4
Northeastern 1,712 21.6 1,566 19.8
West Central 562 13.2 585 13.8
Jeerson 967 14.7 917 13.9
East Central 1,293 18.8 1,220 17.7

2020 ALABAMA STATE HEALTH ASSESSMENT
49
Southeastern 1,188 31.7 1,401 37.4
Southwestern 522 13.2 470 11.9
Mobile 647 15.7 691 16.8
Geographic Variation
Rural 4,203 20.0 4,035 19.2
Urban 4,729 16.9 4,827 17.3
Sex
Female 5,460 - 5,216 -
Male 3,697 - 3,749 -
Race/Ethnicity
White 6,180 - 5,999 -
AA/black 2,473 - 2,504 -
Hispanic or Latino 47 - 41 -
Asian 0 - 11 -
Native Hawaiian 26 - 24 -
Other/unknown 480 - 433 -
Household Income
N/A - - - -
Age (in years)
N/A - - - -
Education
N/A - - - -
Alzheimer’s Disease Among
Medicare Recipients
Alzheimer’s disease aects adults over the age of 50
years old, and 2,659 individuals in AL died with this
co-morbidity listed on their death certificate in 2019.
Alzheimer’s disease is the sixth leading cause of death in
AL, and it is the most common cause of dementia.
5
The
disease often causes loss of functioning and interferes
with daily activities:
· In 2018, Perry County had the highest prevalence
of Medicare recipients diagnosed with
Alzheimer’s disease in AL (13.6percent).
· The historical trend of Alzheimer’s disease-
related deaths between 2010-2018 rose
proportionately in elderly populations. In 2019,
the AL rate of Alzheimer’s disease-related deaths
was 54.2 per 100,000 persons, compared to the
U.S. rate of 37.0deaths per 100,000 persons.
3
Long-term care services, including home and
community-based services, assisted living, and nursing
home care, may be cost-prohibitive since disease
progression is very long. Alzheimer’s disease is closely
linked to access to care, because adequate care is
closely related to payor source.
6
Most individuals over
65years old are on Medicare or private insurance.
Additional demographic information is not available at
this time.
Figure 7.1 – The distribution of Alzheimer’s disease
prevalence by county in 2018. Source: Centers for
Medicare and Medicaid Services.
Lauderdale
Colbert
Franklin
Marion
Winston
Walker
Limestone
Lawrence
Morgan
Cullman
Madison
Jackson
12.3
9.3
10.7
10.3
11.4
12.2
9.9
11.2
11.8
10.6
9.8
11.4
11.1
10.9
10.8
11.3
9.9
13.5
11.5
11.0
11.6
11.1
10.4
12.3
10.9
11.4
11.8
10.5
10.5
10.6
11.0
13.6
19.5
10.5
9.5
11.4
11.4
10.1
12.4
10.9
12.7
11.8
11.8
12.3
12.5
10.8
9.7
12.6
13.0
12.3
11.5
11.5
10.4
12.1
13.1
9.2
12.3
11.1
10.6
10.6
12.7
10.9
9.2
12.6
11.3
12.3
12.5
Marshall
DeKalb
Cherokee
Etowah
Blount
St. Clair
Calhoun
Cleburne
Clay
Talladega
Randolph
Chambers
Tallapoosa
Coosa
Jeerson
Lamar
Fayette
Tuscaloosa
Bibb
Hale
Sumter
Perry
Dallas
Marengo
Choctaw
Washington
Clarke
Monroe
Conecuh
Butler
Crenshaw
Pike
Barbour
Henry
Dale
Coee
Geneva
Prevalence (%)
Houston
Covington
Escambia
Baldwin
Mobile
Wilcox
Lowndes
Montgomery
Autauga
Chilton
Elmore
Macon
Bullock
Russell
Lee
Greene
Pickens
Shelby
15.0%5.0%
Data Sources
Table 7.1 – Adult Abuse Cases, 2018-2019. DHR,
Division of Adult Protective Services, 2018. Data
requested July 2020.
Figure 7.1 – Alzheimer’s Disease Among Medicare
Recipients, 2018. Centers for Medicare and Medicaid
Services, Alzheimer’s Disease, 2019. Data requested
January 2021.
Written Sources
1. U.S. Census Bureau, Projected Age Statistics, 2020.
2. CDC, Promoting Health for Older Adults, 2020.

2020 ALABAMA STATE HEALTH ASSESSMENT
50
2. ADPH, Center for Health Statistics Alzheimer’s
Mortality, 2019.
3. CDC, Geriatrics, 2020.
4. CDC National Center for Health Statistics, Age
Adjusted Leading Causes of Death, 2019.
5. Alzheimer’s Association, New Alzheimer’s
Association Report Reveals Sharp Increases in
Alzheimer’s Prevalence, Death, Cost of Care, 2018.
Community Resources
ADPH Home Health
Location: Montgomery County, AL
Type: State Government Organization
AL Department of Senior Services
Location: Montgomery County, AL
Type: State Government Organization
AL Disabilities Advocacy Program
Location: Statewide
Type: Advocacy Organization
AL Nursing Home Association
Location: Montgomery County, AL
Type: Non-profit Organization
American Association of People with Disabilities
Location: Nationwide
Type: Advocacy Organization
ARC of AL
Location: Statewide
Type: Non-profit Organization
Extendicare Health and Rehab
Location: Etowah County, AL
Type: Health Facility
National Institute on Aging
Location: Washington, DC Metro
Type: Federal Government Organization
National Institutes of Health (NIH) Senior Health
Location: Washington, DC Metro
Type: Federal Government Organization
Redstone Military Retirement Residence Association
Location: Madison County, AL
Type: Non-profit Organization
Ruth and Naomi Senior Outreach
Location: Jeerson County, AL
Type: Non-profit Organization
Social Security Administrative Oce
Location: Montgomery County, AL
Type: Federal Government Association
U.S. Department of Labor’s Oce of Disability
Employment Policy
Location: Washington, DC Metro
Type: Federal Government Organization

2020 ALABAMA STATE HEALTH ASSESSMENT
51
8. Cardiovascular Diseases
Ranked AL’s Eighth Health Indicator
CVDs are identified as the eighth most prominent health
indicator in AL. It refers to a group of serious health
conditions which can result in death and disability.
1
CVD
was the leading cause of death in AL for 2019.
2
CVDs are caused by plaque buildup in an individual’s
arteries. This causes the arteries to narrow over time,
partially or totally blocking the blood flow. The four most
common CVDs are coronary artery disease, heart failure,
heart attacks, and stroke.
1
While the other three conditions
aect the heart, a stroke aects the brain and occurs
when there is a lack of blood flow to an area of the brain.
Stroke was the fourth leading cause of death in AL in 2019.
2
Another common CVD condition that aects many
American adults is hypertension (also called high
blood pressure). According to CDC, an individual can
be considered to have pre-hypertension based on the
following: family history, weight, level of physical activity,
diet, smoking, and having other co-existing diseases,
such as diabetes.
1
Many people in AL have hypertension
or high cholesterol but are not aware of their condition.
Unfortunately for many individuals, chest pain is the first
reason for visiting the doctor.
Vulnerable Populations
CVDs are considered an aging disease, which means your
risk of receiving the diagnosis increases with age. White
males have the highest risk of developing CVDs, followed
by AA/black males, AA/black females, and Asian males.
1
Individuals that live in food deserts (i.e., places with
limited access to healthy and aordable food choices)
and low-income neighborhoods with little green space
have higher rates of CVD morbidity.
3
Geographic Variation
AL is within the CDC designated “Stroke Belt” that
includes most of the southeast U.S. (i.e.,Arkansas,
Georgia, Indiana, Kentucky, Louisiana, Mississippi, North
Carolina, South Carolina, Tennessee, and Virginia.) These
states had an age-adjusted stroke mortality rate that
exceeded the national rate by 34 percent in 2018.
1
Topics Addressed for This Indicator are:
· Adults told they have high blood pressure.
· Hypertension diagnosis in Medicaid recipients.
· Hypertension among Medicare recipients.
· Hyperlipidemia among Medicare recipients.
· Stroke among Medicare recipients.
· BCBS members who had cardiovascular-related
claims.
· Heart disease and stroke mortality.
Highlights
Indicator data are collected from Blue Cross Blue Shield
of AL (BCBS) Claims, Centers for Medicare and Medicaid
Services, AL Medicaid Agency, BRFSS, and the ADPH
Center for Health Statistics Mortality Files.
· AL’s stroke mortality rate was 64.0 deaths per
100,000 persons in 2019.
· Shelby County, located in the Northeastern
Public Health District, had the highest stroke rate
with 142.1deaths per 100,000 persons.
· According to BRFSS data, hypertension diagnosis
is higher in populations with low income and low
education attainment.
Risk Factors:
· Family history of CVD.
· Overweight/obesity.
· High sodium and high-fat diet.
· Reduced outdoor recreational access.
· Lack of education.
· Poor access to healthy foods.
· Minority racial groups (particularly AA/blacks and
Asian males).
· Smoking and second-hand smoke.
· Co-morbid diabetes diagnosis.
Adults Told They Have High Blood
Pressure
The statewide prevalence for adults who have been told
they have high blood pressure was 10.2 percent higher
than the national median:
· The risk of being diagnosed with hypertension
increases with age. Twothirds of individuals
over 65 years old have been told they have high
blood pressure.
· According to BRFSS data, males have a similar
prevalence of high blood pressure compared
to females. AA/black individuals have a 5.4
percent higher prevalence of high blood pressure
compared to white individuals.

2020 ALABAMA STATE HEALTH ASSESSMENT
52
· Individuals with a household income of less than
$15,000 and have less than a high school education
have the highest prevalence of hypertension.
Table 8.1 – Percentage of Adults Told
They Have High Blood Pressure, 2019
% 95% CI
AL 42.5 (41.0-44.0)
U.S. Median 32.3 -
Public Health Districts
Northern 42.0 (38.2-45.8)
Northeastern 43.0 (39.3-46.6)
West Central 43.4 (39.3-47.6)
Jeerson 40.0 (36.2-43.8)
East Central 42.4 (38.1-46.7)
Southeastern 47.8 (43.3-52.4)
Southwestern 43.2 (39.2-47.3)
Mobile 40.0 (36.1-43.9)
Geographic Variation
N/A - -
Sex
Male 44.3 (42.0-46.6)
Female 40.8 (38.9-42.7)
Race
White 42.4 (40.6-44.1)
AA/black 47.8 (44.7-50.9)
Household Income
Less than 15,000 54.4 (49.2-59.6)
$15,000-24,999 49.3 (45.2-53.5)
$25,000-34,999 43.7 (38.2-49.1)
$35,000-49,999 38.2 (34.0-42.5)
$50,000+ 35.9 (33.6-38.2)
Age (in years)
25-34 19.4 (15.8-23.0)
35-44 32.7 (28.9-36.5)
45-54 46.9 (43.3-50.4)
55-64 60.1 (57.1-63.2)
65+ 68.8 (66.6-71.0)
Education
Less than high school 53.2 (48.0-58.4)
High school or GED 43.6 (40.9-46.3)
Some college 39.2 (36.6-41.8)
College graduate or higher 38.3 (35.9-40.8)
Hypertension Diagnosis in Medicaid
Recipients
Medicaid covers children and adults under the age of 65
years old. In AL, 7.4percent of Medicaid recipients were
diagnosed with hypertension in 2018:
· The county with the highest hypertension
prevalence is Sumter County (16.9 percent).
Sumter County is located in the West Central
Public Health District.
· The West Central Public Health District had
the highest prevalence of Medicaid recipients
diagnosed in 2018 (9.1percent).
· In the Medicaid population, the number of white
and AA/black diagnosed with hypertension is
similar in AL in 2018.
· Rural areas have a higher percentage of Medicaid
recipients diagnosed with hypertension
compared to urban areas (8.3 percent compared
to 6.0 percent, respectively).
For the district level, only confirmed county diagnoses
were included in the calculation.
Table 8.2 – Percentage of Medicaid Recipients
Diagnosed with Hypertension in AL, 2018
Count %
AL 89,108
7.4
U.S. - -
Public Health Districts
Northern 17,092 7.2
Northeastern 13,577 7.0
West Central 10,972 9.1
Jeerson 8,666 5.4
East Central 11,950 6.3
Southeastern 10,512 9.0
Southwestern 9,712 8.6
Mobile 6,403 5.4
Geographic Variation
Rural 49,096 8.3
Urban 40,012 6.0
Sex
Male 59,346 -
Female 29,762 -
Race
White 38,686 -
AA/black 40,618 -
Hispanic 595 -
Other/not provided 9,210 -
Household Income
N/A - -
Age (in years)
Under 21 2,143 -
21 and Over 86,965 -
Education
N/A - -

2020 ALABAMA STATE HEALTH ASSESSMENT
53
Hypertension Among Medicare
Recipients
Hypertension (high blood pressure) can increase your
risk of myocardial infarction, stroke, and other CVDs.
1
Hypertension increases dramatically with age:
· The prevalence of Alabamians on Medicare with
hypertension was 65.5percent in 2018. In the
2015 CHA, the state prevalence was 61.0 percent.
· Rural areas had 66.5 percent of Medicare
recipients with hypertension, while urban areas
had 63.9 percent of Medicare recipients with
hypertension.
· Choctaw County had the highest percentage
of individuals on Medicare with a hypertension
diagnosis in 2018, 74.0 percent.
Additional demographic information is not available at
this time.
Figure 8.1 – This map represents the percentage of
Medicare recipients with hypertension throughout the
state. Source: Centers for Medicare and Medicaid Services.
Lauderdale
Colbert
Franklin
Marion
Winston
Walker
Limestone
Lawrence
Morgan
Cullman
Madison
Jackson
68.2
66.9
65.4
68.0
71.5
69.2
70.0
65.6
65.3
65.5
63.4
66.8
64.7
66.2
70.3
68.1
67.5
68.6
71.7
66.5
66.1
65.3
66.8
66.0
63.4
62.2
67.6
72.9
73.0
69.7
68.4
72.4
68.6
64.6
62.0
64.5
67.2
64.2
66.8
66.3
68.3
68.0
67.9
63.9
69.8
66.5
73.0
66.2
72.6
68.5
66.3
67.8
66.8
67.5
61.6
62.3
62.1
60.7
62.3
65.0
68.3
69.5
66.9
67.3
62.5
74.0
61.0
Marshall
DeKalb
Cherokee
Etowah
Blount
St. Clair
Calhoun
Cleburne
Clay
Talladega
Randolph
Chambers
Tallapoosa
Coosa
Jeerson
Lamar
Fayette
Tuscaloosa
Bibb
Hale
Sumter
Perry
Dallas
Marengo
Choctaw
Washington
Clarke
Monroe
Conecuh
Butler
Crenshaw
Pike
Barbour
Henry
Dale
Coee
Geneva
Prevalence (%)
Houston
Covington
Escambia
Baldwin
Mobile
Wilcox
Lowndes
Montgomery
Autauga
Chilton
Elmore
Macon
Bullock
Russell
Lee
Greene
Pickens
Shelby
80.0%20.0%
Hyperlipidemia Among Medicare
Recipients
Hyperlipidemia is an abnormally high concentration of
fats or lipid in the blood. The increase of fat deposits
in the veins can lead to arteriosclerosis, which is the
hardening of the blood vessels.
1
In 2018, 51.3percent of AL Medicare recipients had
hyperlipidemia, compared to the U.S. prevalence of
47.7percent. In the 2015 CHA, 45.1percent of Medicare
recipients had hyperlipidemia in AL:
· The Northern Public Health District had the
highest prevalence of hyperlipidemia.
· In 2018, Colbert County had the highest prevalence,
with 59.6percent of the Medicare recipients having
hyperlipidemia, followed by Pickens County at
58.5percent, and Coee County at 58.3percent.
· In 2018, Clarke County had the lowest
prevalence, with 37.0percent.
Figure 8.2 – This map represents the percentage of
Medicare recipients with hyperlipidemia throughout the
state. Source: Centers for Medicare and Medicaid Services.
Lauderdale
Colbert
Franklin
Marion
Winston
Walker
Limestone
Lawrence
Morgan
Cullman
Madison
Jackson
54.1
53.8
56.9
55.5
59.6
51.9
56.9
52.5
49.0
50.1
52.8
52.6
53.8
52.3
53.0
53.4
48.8
53.0
57.7
50.8
51.7
48.9
52.9
50.1
46.2
50.9
56.5
58.5
51.2
46.7
46.8
49.3
57.4
49.4
41.2
46.2
43.4
51.6
47.5
54.0
44.8
57.9
50.3
48.8
47.2
39.7
49.7
42.5
57.5
58.3
50.6
54.2
57.5
55.5
37.0
42.9
49.0
52.6
48.6
52.4
43.5
46.8
38.6
44.2
45.4
48.5
45.7
Marshall
DeKalb
Cherokee
Etowah
Blount
St. Clair
Calhoun
Cleburne
Clay
Talladega
Randolph
Chambers
Tallapoosa
Coosa
Jeerson
Lamar
Fayette
Tuscaloosa
Bibb
Hale
Sumter
Perry
Dallas
Marengo
Choctaw
Washington
Clarke
Monroe
Conecuh
Butler
Crenshaw
Pike
Barbour
Henry
Dale
Coee
Geneva
Prevalence (%)
Houston
Covington
Escambia
Baldwin
Mobile
Wilcox
Lowndes
Montgomery
Autauga
Chilton
Elmore
Macon
Bullock
Russell
Lee
Greene
Pickens
Shelby
60.0%30.0%

2020 ALABAMA STATE HEALTH ASSESSMENT
54
Additional demographic information is not available at
this time.
Stroke Among Medicare Recipients
AL is within the CDC designated “Stroke Belt” that
includes most of the states within the southeast,
such as Arkansas, Georgia, Indiana, Kentucky,
Louisiana, Mississippi, North Carolina, South Carolina,
Tennessee, and Virginia. These states had an age-
adjusted stroke mortality rate that dramatically
exceeds the overall national rate in 2018.
1
· The AL Medicare stroke prevalence was 4.2
percent for 2018. In the 2015CHA, the state
prevalence was 4.1percent.
· Covington County had the highest stroke
prevalence among Medicare recipients with
9.8percent, followed by Conecuh with 6.5percent.
· Bullock County had the lowest prevalence at
2.8 percent of Medicare recipients who had a
stroke diagnosis.
Additional demographic information was not available at
this time.
Blue Cross and Blue Shield
Members with Cardiovascular
Disease-related Claims
CDC estimates that heart disease costs the U.S. about
$219 billion each year.
1
The data presented in Table 8.3 refers to BCBS CVD-
related claims. BCBS is one of the largest private
insurance companies in AL.
CVDs include heart failure, high blood pressure, and
coronary artery disease. The claims are either based
on medication usage or therapy that was administered
during a physician visit:
· The percentage of AL BCBS members who had
CVD-related claims has increased every year but
dramatically increased from 2018-2019.
· In 2019, Bullock County had the highest
prevalence of BCBS members with CVD-related
claims (44.1 percent). Bullock County is located
in the East Central Public Health District.
Table 8.3 – Percentage of AL BCBS Members with
Cardiovascular Disease-related Claims, 2016-2019
2016 2017 2018 2019
AL 18.0 20.2 21.4 26.0
U.S. - - - -
Public Health Districts
Northern 16.0 17.5 18.9 22.7
Northeastern 17.4 19.4 20.1 24.6
West Central 20.7 23.6 25.7 30.5
Jeerson 18.3 19.9 20.1 24.1
East Central 18.9 22.3 24.1 29.4
Southeastern 19.4 22.0 23.6 28.6
Southwestern 17.6 20.5 21.6 26.9
Mobile 18.4 20.8 22.3 27.4
Geographic Variation
Rural 18.6 21.2 22.6 27.5
Urban 17.5 19.5 20.6 24.8
Sex
N/A - - - -
Figure 8.3 – This map represents the percentage of
Medicare recipients with strokes throughout the state.
Source: Centers for Medicare and Medicaid Services.
Lauderdale
Colbert
Franklin
Marion
Winston
Walker
Limestone
Lawrence
Morgan
Cullman
Madison
Jackson
4.1
3.8
4.6
4.0
4.3
3.7
3.4
3.5
4.9
3.5
2.9
4.3
4.1
4.4
3.9
3.7
3.8
4.5
4.0
4.0
3.8
3.6
3.5
3.8
4.3
4.0
4.2
3.7
3.4
4.0
3.7
4.1
4.9
4.3
4.0
4.2
3.6
4.2
4.9
5.2
2.8
4.6
3.8
5.0
4.5
5.0
6.5
4.5
9.8
4.8
4.6
4.2
4.4
5.0
3.7
3.6
4.1
3.8
4.1
4.2
4.2
3.1
3.3
4.9
4.3
4.5
3.9
Marshall
DeKalb
Cherokee
Etowah
Blount
St. Clair
Calhoun
Cleburne
Clay
Talladega
Randolph
Chambers
Tallapoosa
Coosa
Jeerson
Lamar
Fayette
Tuscaloosa
Bibb
Hale
Sumter
Perry
Dallas
Marengo
Choctaw
Washington
Clarke
Monroe
Conecuh
Butler
Crenshaw
Pike
Barbour
Henry
Dale
Coee
Geneva
Prevalence (%)
Houston
Covington
Escambia
Baldwin
Mobile
Wilcox
Lowndes
Montgomery
Autauga
Chilton
Elmore
Macon
Bullock
Russell
Lee
Greene
Pickens
Shelby
10.0%0.0%

2020 ALABAMA STATE HEALTH ASSESSMENT
55
Race
N/A - - - -
Household Income
N/A - - - -
Age (in years)
N/A - - - -
Education
N/A - - - -
Heart Disease and Stroke Mortality
CVD is the number one cause of death in AL and across
most of the U.S. AL had a rate of 274.2 heart disease-
related deaths per 100,000 persons in 2019.
· The Southeastern Public Health District
had the highest heart disease mortality rate
(304.5deaths per 100,000 persons).
· Rural areas had 313.8 heart disease deaths per
100,000 persons, compared to urban areas with
244.4 heart disease deaths per 100,000 persons.
· White individuals had 319.1 heart disease deaths
per 100,000 persons, compared to AA/black
individuals with 239.5 heart disease deaths per
100,000 persons.
· Age increased the risk of heart disease mortality
with individuals over age 65 years old experiencing
1,201.8 deaths per 100,000 persons.
· Shelby County, located in the Northeastern
Public Health District, had the highest stroke rate
with 142.1deaths per 100,000 persons.
· Rural areas had 73.0 stroke deaths per 100,000
persons, compared to urban areas with
58.4stroke deaths per 100,000 persons.
Data Sources
Table 8.1 – Percentage of Adult Told They Have
High Blood Pressure, 2019. ADPH, BRFSS, 2019. Data
requested March 2021.
Figure 1.1 – Hypertension Among Medicare
Recipients, 2018. Centers for Medicare and Medicaid
Services, 2019. Data requested March 2021.
Table 8.2 – Percentage of Medicaid Recipients
Diagnosed with Hypertension in AL, 2018. AL Medicaid
Agency, 2019. Data requested July 2020.
Figure 8.2 – Hyperlipidemia Among Medicare
Recipients, 2018. Centers for Medicare and Medicaid
Services, 2019. Data requested March 2021.
Figure 8.3 – Stroke Among Medicare Recipients,
2018. Centers for Medicare and Medicaid Services, 2019.
Data requested March 2021.
Table 8.3 – Percentage of AL BCBS Members with
Cardiovascular Disease-Related Claims, 2016-19.
BCBS Claims Data, 2019. Data requested October 2020.
Figure 8.4 – Heart Disease and Stroke Mortality Rate
in AL, 2019. ADPH, Center for Health Statistics Mortality
Files, 2019. Data requested March 2021.
Written Sources
1. CDC, Heart Disease, 2019.
2. Americas Health Rankings, Cardiovascular Diseases,
2018.
3. AHA, Food Deserts and Adverse Cardiovascular
Outcomes, 2019.
4. AL Medicaid Agency, Hypertension, 2019.
Figure 8.4 – Heart disease and stroke mortality rate
in AL by public health district. Source: ADPH Center
for Health Statistics.
Alabama Total
Northern
Northeastern
West Central
Jeerson
East Central
Southeastern
Southwestern
Mobile
■Heart Disease ■Stroke Per 100,000 residents
274.2
64.0
290.0
59.2
279.3
63.6
301.5
60.6
235.2
76.1
222.0
62.8
304.5
59.1
295.2
62.4
296.9
69.9

2020 ALABAMA STATE HEALTH ASSESSMENT
56
Community Resources
ADPH Blood Pressure Monitoring Stations Program
Location: Statewide
Type: State Coordinated Program
ADPH Home Health Biomonitoring Program
Location: Marengo County, AL
Type: State Coordinated Program
AHA
Location: Nationwide
Type: Non-profit Organization
American Journal of Cardiovascular Disease
Location: Nationwide
Type: Research Institution
American Lung Association
Location: Nationwide
Type: Non-profit Organization
CDC
Location: Atlanta, GA
Type: Federal Government Organization
USDHHS Oce of Minority Health
Location: Washington, DC Metro
Type: Research Institution
Healthy People 2030
Location: Nationwide
Type: Advocacy Organization
Million Hearts
Location: Nationwide
Type: Advocacy Group
Wellness Coalition
Location: Montgomery County, AL
Type: Non-profit Organization
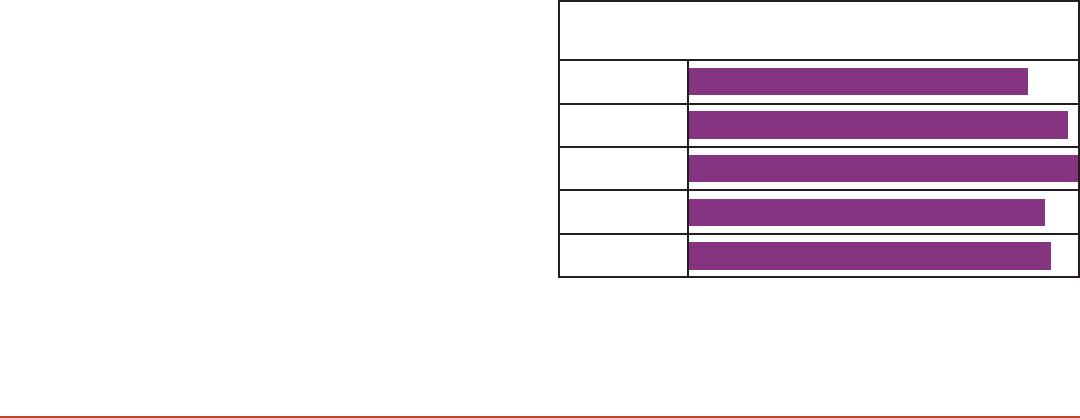
2020 ALABAMA STATE HEALTH ASSESSMENT
57
9. Child Abuse/Neglect
Ranked AL’s Ninth Health Indicator
Child abuse and neglect (also referred to as child
maltreatment) are important health issues for AL
and were identified as the ninth health indicator.
Unfortunately, instances of child abuse and neglect are
often underreported. In AL, healthcare professionals,
schoolteachers, law enforcement oces, social workers,
daycare employees, and clergy are required by law to report
suspected or known instances of child abuse or neglect.
Physical abuse, sexual abuse, emotional abuse, and
neglect are the four most common types of child abuse.
Chronic abuse may result in increasing inflammatory
stress markers. Adverse childhood experiences
can lead to a higher risk for mental health disorders,
chronic diseases, and a poorer socioeconomic status
in adulthood.
1
All forms of abuse could lead to impaired
psychosocial relationships and heightened anxiety.
2
Vulnerable Populations
A combination of individual, familial, community,
and societal factors contribute to child abuse and
neglect outcomes. According to CDC, “rates of child
abuse and neglect are five times higher for children in
families with low socioeconomic status compared to
children in families with higher socioeconomic status.”
1
Communities that experience high rates of violence and
crime, communities with high unemployment rates, and
caregivers with unstable housing are also risk factors for
child abuse and neglect.
1
Geographic Variation
To protect children’s identities, data regarding geographic
variation has not been reported. On the state level, child
abuse cases have been steadily increasing throughout
the years. There were 8,466child maltreatment victims
in 2015, and the number increased to 12,158 new victims
in 2018.
Also, there were 23.3 child abuse calls per 1,000
children under age 18 years old in 2019.
4
Topics Addressed for This Indicator are:
· Child abuse calls.
· Maltreatment types of child victims.
Highlights
In AL, the Oce of Child Protective Services (OCPS)
within the Family Services Division of the AL DHR is
responsible for collecting child abuse and neglect
reports. Data are retrieved from the AL DHR and the
National Child Abuse and Neglect Data System:
· Child abuse calls have increased between 2015-
2017, with the highest call rate in 2017 (25.1calls
per 1,000 children).
· Most maltreatment calls were made by adults
concerned for children under 12 years old, with
16.7 percent of the calls being children under one
year old in 2018.
Risk Factors:
· Domestic violence.
· Parents are going or have gone through a divorce.
· Multiple caretakers.
· Long, unsupervised hours.
Child Abuse Calls
Child abuse and negligent death calls include those
which result from apparent lack of care, abusive head
injury/trauma, and other forms of physical violence. Child
abuse education and training for parents, educators, and
caregivers are aimed at decreasing the number of deaths
attributable to abuse and neglect.
In 2019, there were 1,088,306 children less than 18 years
old in AL.
5
According to the AL DHR, these call rates were
calculated by using the number of unique reported
victims, not confirmed. A child may have been the victim
of more than one type of maltreatment or reported the
same type of maltreatment more than once:
· Child abuse calls increased between 2015-2017,
with the highest call rate in 2017 (25.1calls per
1,000 children).
· In 2019, the child abuse call rate was 23.3 calls
per 1,000 children.
Data by demographic groups were not available.
21.8
24.4
25.1
22.9
23.3
Figure 9.1 – Child Abuse Calls Per Year, 2015-2019. The
figure displays the rates per 1,000 children. Source: AL DHR.
2015
2016
2017
2018
2019

2020 ALABAMA STATE HEALTH ASSESSMENT
58
Maltreatment Types of Child Victims
Maltreatment encompasses emotional abuse, medical
neglect, physical abuse, sexual abuse, and general neglect.
A child maltreatment victim is a child who is the subject of
a substantiated or indicated maltreatment report. In 2018,
there were 11.1 maltreatment victims per 1,000 children:
· Physical abuse was the most prevalent
maltreatment type (53.3 percent), followed by
neglect (42.9 percent) and sexual abuse (16.6
percent) in 2018.
· In 2018, there were 5,055unique incidents of
confirmed maltreatment. The calls came from 2.4
percent of children having repeated occurrences.
4
· Most maltreatment calls were made by adults
concerned for children under 12, with 16.7percent of
the calls being children under one year old in 2018.
Some columns may be greater than 100percent, as an
individual victim may be counted twice.
Table 9.1 – Percentage of Child Victims, 2017-2018
2017 2018
AL 10,847 12,158
U.S. - -
Type of Maltreatment
Emotional abuse 0.4 0.3
Medical neglect 0.9 0.6
Neglect 43.9 42.9
Physical abuse 53.6 53.3
Sexual abuse 14.9 16.6
Ethnicity of Victim
White 64.3 62.8
AA/black 26.6 28.6
Hispanic 4.5 3.8
Other 4.6 4.8
Age (in years)
0-12 79.2 79.7
13-19 20.6 19.9
Unknown 0.3 0.5
Data Sources
Figure 9.1 - Child Abuse Calls per Year, 2015-2019.
AL DHR, Division of Child Protective Services, 2019. Data
requested July 2020.
Table 9.1 – Percentage of Child Victims, 2017-2018.
National Child Abuse and Neglect Data System, 2017-
2018. Data requested January 2021.
Written Sources
1. CDC, Child Abuse and Neglect, 2020.
2. ADPH, Injury Prevention Child Abuse and Neglect, 2021.
3. USDHHS Child Welfare Information Gateway, Cultural
Responsiveness: Child Abuse and Neglect, 2020.
4. National Child Abuse and Neglect, Child
Maltreatment, 2019.
5. U.S. Census Bureau, American Community Survey, 1
Year Estimate, 2019.
Community Resources
ADPH Maternal Child Health Services (MCH) Program
Location: Montgomery County, AL
Type: State Government Organization
AL DHR
Location: Montgomery County, AL
Type: State Government Organization
Child Protect
Location: Montgomery County, AL
Type: Advocacy Program
Child Safety Learning Collaborative
Location: Atlanta, GA
Type: Federal Funded Program
Children’s Advocacy Center
Location: Shelby County, AL
Type: Non-profit Organization
Family Guidance Center – AL
Location: Jeerson County, AL
Type: Non-Profit Organization
Heart Gallery AL
Location: Jeerson County, AL
Type: Nonprofit Organization
National Child Abuse and Neglect Data System
Location: Washington, DC Metro
Type: Federal Government Organization

2020 ALABAMA STATE HEALTH ASSESSMENT
59
10. Environmental Health
Ranked AL’s Tenth Health Indicator
Environmental health is a new addition to the SHA
and is currently ranked as tenth AL’s health indicator.
Environmental health is focused on the natural and man-
made environments for the benefit of human health.
The environment directly aects the quality of life and is
impacted by socioeconomic disparities.
1
Environmental health can start within an individual’s
home with proper ventilation, using non-lead-based
paint, properly treated tap water for consumption, and
removing electrical hazards.
2
Maintaining healthy homes
and communities helps keep an individual healthy.
Vulnerable Populations
Anyone can be exposed to environmental health concerns,
but certain populations are more vulnerable. For example,
individuals with cardiovascular or respiratory conditions
may be more susceptible to heat-related illness,
3
and
lead exposure in children can cause underperformance in
school and slowed growth and development.
Geographic Variation
Data by geographic region has not been reported for this
indicator.
Topics Addressed for This Indicator are:
· Drought and hot weather hazards.
· Public water systems.
· Water quality lead testing at schools.
Highlights
Indicator data are retrieved from the ADPH Bureau of
Environmental Services, Environmental Protection Agency
(EPA), ALDOT, ALSDE, and local community ocials.
· In 2019, there were 510 community water
systems throughout AL.
· Lead in water detection tests were conducted at
most schools throughout AL in 2017-2019.
Risk Factors:
· Low income housing.
· Exposure to chemicals.
· Poor indoor ventilation.
· Drinking unsafe water.
· Unsafe cooking sanitation.
· Climate change.
Droughts and Hot Weather Hazards
AL has a humid subtropical climate, and the seasonal highs
have been steadily increasing over time. A heatwave is a
period of excessively hot weather that typically lasts two or
more days and may be accompanied by high humidity.
4
In
the 1980s, there was an average of four recorded days with
heat waves per year. By the 2010s, there were at least 20-
30 recorded days a year.
4
Heat waves are also associated
with increased hospital admissions for cardiovascular,
kidney, and respiratory disorders.
5
Heat-related illnesses occur when the body is unable to
control its temperature. Heat exhaustion can develop
after several days of exposure to high temperatures
and inadequate or unbalanced replacement of
fluids.Vulnerable populations for heat-related illnesses
include individuals with chronic medical conditions,
infants, older adults, and outdoor workers:
5
Figure 10.1 – A map of the highest impacted areas of
drought between April 2016, to April 2017. Most of the state
was at least in one class degradation away from stable
water tables. Source: National Drought Mitigation Center.
Lauderdale
Colbert
Franklin
Marion
Winston
Walker
Limestone
Lawrence
Morgan
Cullman
Madison
Jackson
Marshall
DeKalb
Cherokee
Etowah
Blount
St. Clair
Calhoun
Cleburne
Clay
Talladega
Randolph
Chambers
Tallapoosa
Coosa
Jeerson
Lamar
Fayette
Tuscaloosa
Bibb
Hale
Sumter
Perry
Dallas
Marengo
Choctaw
Washington
Clarke
Monroe
Conecuh
Butler
Crenshaw
Pike
Barbour
Henry
Dale
Coee
Geneva
Houston
Covington
Escambia
Baldwin
Mobile
Wilcox
Lowndes
Montgomery
Autauga
Chilton
Elmore
Macon
Bullock
Russell
Lee
Greene
Pickens
Shelby
1 Class Degradation 2 Class Degradation 3 Class Degradation

2020 ALABAMA STATE HEALTH ASSESSMENT
60
· Between 2010-2019, there were 379 days of
reported heat waves in AL.
· There were 86physical injuries and 10deaths
due to heat illness in the same period.
5
· High temperatures can also lead to water
shortages. AL has had two statewide severe
drought seasons since 2012. This impacts
agriculture, fishing, and river wildlife maintenance.
· Figure 10.1 is a map showing how widespread the
impact of the 2016 severe droughts was in AL.
There were no reported deaths or injuries related
to this event.
Summer is the driest time of the year, which can lead to
fire hazards. In the past 10 years, there have been nine
wildfires, with no injuries or deaths.
6
Public Water Systems
The Safe Drinking Water Act (SDWA) ensures Americans’
drinking water quality by regulating public water
systems (PWS).
7
Under SDWA, EPA sets standards for
drinking water quality and oversees the programs for
states, federally recognized tribes, and territories that
implement the drinking water program. A key component
of water quality is fluoridation.
CDC recognized community water fluoridation as one
of the ten greatest public health achievements of the
20thCentury.
7
CDC recommends water fluoridation as
one of the most practical, cost-eective, equitable, and
safe measures a community can take to prevent tooth
decay and improve oral health as well.
In 2019, CDC rewarded 56 AL PWS for their consistent
and professional adjustment of fluoride content to the
recommended level for oral health:
8
· In 2019, there were 510 community water
systems, 22non-transient, non-community
water systems, and 48transient, non-community
water systems in AL.
· Since 2014, AL has conducted at least 542site
visits per year. Less than 22percent of those PWS
had any violations, and no more than 7sites had
a serious violation.
· In Figures 10.2a and 10.2b, there were unusually
high amount of violations in 2019 compared to the
previous years, but this may have been associated
with changes in environmental regulation.
Figure 10.2a – The public water systems by calendar year
that had any environmental violations. Source: U.S. EPA.
2014
2015
2016
2017
2018
2019
118
86
60
74
75
117
Figure 10.2b – The public water systems by calendar
year that had any serious environmental violations.
Source: U.S. EPA.
2014
2015
2016
2017
2018
2019
4
4
3
2
3
7
Water Quality Lead Testing at Schools
Lead is a highly toxic metal that was commonly used in
household paint (banned in 1978), gasoline (banned for on-
road vehicles in 1995), and plumbing pipes and fixtures.
9
According to CDC, lead is a multi-system toxicant and
can cause learning diculties, digestive problems,
kidney damage, anemia, and high blood pressure. Since
the body and nervous system are not fully developed
in children under 6years old, high lead exposure can
potentially be life-threatening.
9
Lead levels from blood tests are reportable to ADPH, and
it is recommended to test children at 12to24 months
of age. There is currently no AL regulatory requirement
for testing lead levels in the drinking water at schools.
10
However, because school-aged children are especially
vulnerable to the adverse health eects of elevated lead
levels, the AL Department of Environmental Management
(ADEM) and ALSDE joined together in March of 2016, to
develop a voluntary school testing program. Testing was
held between April 2017 to November 2019.
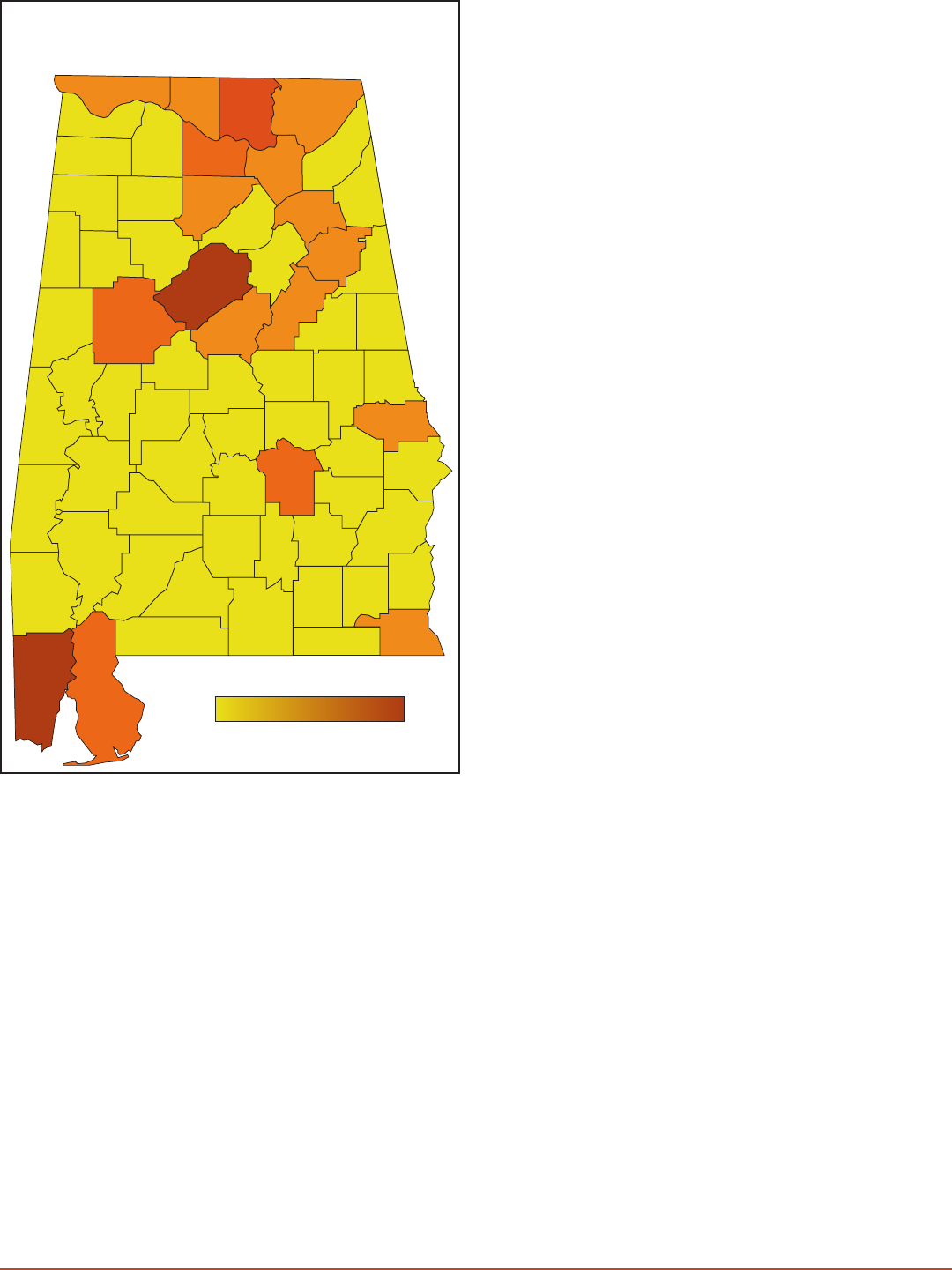
2020 ALABAMA STATE HEALTH ASSESSMENT
61
Site selection was based on plumbing fixture type, age,
and accessibility to students and sta, with at least one
water cooler and one kitchen sink, tested at each school.
More information about this process is detailed on the
ADEM website:
· In Figure 10.3, the map indicates over 1,100public
schools have been tested.
· Detectable lead levels were in 33 schools in AL,
which required aected plumbing fixtures to be
taken out of service, replaced, and resampled.
Data Sources
Figure 10.1 – U.S. Drought Monitor Class Change – AL,
1 year. USDA National Drought Mitigation Center, 2016-
2018. Data requested July 2020.
Figure 10.2a – PWS with At Least One Violation. U.S.
EPA, Enforcement and Compliance History Online, 2019.
Data requested July 2020.
Figure 10.2b – PWS with Serious Violations. U.S. EPA,
Enforcement and Compliance History Online, 2019. Data
requested July 2020.
Figure 10.3 – Schools Participating in the Lead Program,
2017-2019. ADEM, 2019. Data requested March 2021.
Written Sources
1. Healthy People 2030, Environmental Health, 2020.
2. ADPH Bureau of Environmental Services, Indoor Air
Quality and Lead, 2019.
3. CDC, Warning Signs and Symptoms of Heat-
Related Illness, 2020.
4. U.S. EPA, Health Eects of Residence near
hazardous Waste, 2000.
5. CDC WONDER, Environment: Heat Wave Days May -
September 2018.
6. National Oceanic and Atmospheric Administration,
AL Weather Events, 2020.
7. CDC, Community Water Fluoridation, 2020.
8. U.S. EPA, Drinking Water Dashboard, 2019.
9. CDC, Lead Levels in Children, 2020.
10. ADEM, Lead Testing in Schools Final Update, 2019.
Figure 10.3 – A map of the school water lead testing
across AL. No data reported for Butler, Dallas, Perry,
and Macon counties. Source: ADEM.
Lauderdale
Colbert
Franklin
Marion
Winston
Walker
Limestone
Lawrence
Morgan
Cullman
Madison
Jackson
22
21
68
22
15
4
14
44
29
17
8
39
19
36
11
13
8
6
10
8
35
8
3
2
21
38
59
8
5
3
6
0
11
14
3
5
3
27
0
19
4
10
9
3
0
7
8
15
11
11
9
12
5
12
9
8
98
47
17
13
0
7
7
5
55
4
99
Marshall
DeKalb
Cherokee
Etowah
Blount
St. Clair
Calhoun
Cleburne
Clay
Talladega
Randolph
Chambers
Tallapoosa
Coosa
Jeerson
Lamar
Fayette
Tuscaloosa
Bibb
Hale
Sumter
Perry
Dallas
Marengo
Choctaw
Washington
Clarke
Monroe
Conecuh
Butler
Crenshaw
Pike
Barbour
Henry
Dale
Coee
Geneva
Total Schools
Houston
Covington
Escambia
Baldwin
Mobile
Wilcox
Lowndes
Montgomery
Autauga
Chilton
Elmore
Macon
Bullock
Russell
Lee
Greene
Pickens
Shelby
1001

2020 ALABAMA STATE HEALTH ASSESSMENT
62
Community Resources
ADPH Indoor Air Quality Lead Branch
Location: Montgomery County, AL
Type: State Government Organization
ADEM
Location: Montgomery County, AL
Type: State Government Organization
AL Rivers Alliance
Location: Jeerson County, AL
Type: Non-profit Organization
Black Warrior River Keeper
Location: Jeerson County, AL
Type: Non-profit Organization
Cahaba River Society
Location: Jeerson County, AL
Type: Non-profit Organization
Children’s Environmental Health Network
Location: Washington, DC Metro
Type: Non-profit Organization
Conservation AL
Location: Montgomery County, AL
Type: Conservation Area
Emergency Management Agency
Location: Chilton County, AL
Type: State Government Organization
Land Trust of North AL
Location: Madison County, AL
Type: Conservation Area
Red Mountain Search Dog Association
Location: Shelby County, AL
Type: Nonprofit Organization

2020 ALABAMA STATE HEALTH ASSESSMENT
63
11. Violence
Ranked AL’s Eleventh Health Indicator
Alabamians identified violence as the eleventh most
significant current health indicator in AL. Violence aects an
individual long after the initial incident occurs. A community
approach to help prevent violence and understand the risk
and protective factors of violence is essential for the health,
safety, and well-being of that population.
1
Vulnerable Populations
Women and minority groups are more vulnerable to acts
of violence against them. According to CDC, 1in5 women
and nearly 1in 7men in the U.S. have experienced some
form of intimate partner violence during their lifetime.
1
The Federal Bureau of Investigation’s (FBI) Uniform Crime
Reporting (UCR) system reports that the motivation for
single-bias hate crime incidents across the U.S. targeted
victims for their race (57.6 percent), religion (20.1percent),
and sexual orientation (16.7 percent) in 2019.
2
Geographic Variation
Crime statistics are considered a valuable indicator for
neighborhood safety, particularly firearm violence. Rural
areas typically have higher death rates due to longer
emergency transport times after any accident.
Topics Addressed for This Indicator are:
· Violent crimes.
· Violent deaths.
· Firearm-related deaths.
Highlights
The AL Violent Death Reporting System (AVDRS) is a
statewide surveillance program within ADPH and funded
by CDC. AVDRS collects detailed information on deaths
resulting from violence across the state. Death statistics
include suicides, homicides, unintentional firearm deaths,
and legal intervention deaths. Data are also retrieved from
ADPH Center for Health Statistic Mortality Files:
· In 2019, firearms contributed to most of the
suicides/intentional self-harm-related deaths
(51.2percent) and homicides (45.4 percent) in AL.
5
· In AL, males are four times more likely to die
from violent deaths than females (49.8deaths
compared 12.0deaths per 100,000 persons).
Risk Factors:
· Low income housing.
· Presence of neighborhood crime.
Violent Crimes
Violent crimes include assaults, robberies, rapes, and
homicides. AL had 22,927 reports for violent crime and
117,379reports for property crime in 2019:
3
· Larceny, which is theft of personal property, was
the most prominent violent crime in the state
during 2019, followed by burglary and assault.
3
· Domestic violence was indicated in 4,207
oenses for 2018. Of these oenses, 80percent
of the victims were female, 48percent were AA/
black, and 49percent were white individuals.
3
· In 2019, Russell County had the highest homicide
rate of 34.5 per 100,000 persons. Tallapoosa
County had the highest assault rate of 720.9
per 100,000 persons. Jeerson County had the
highest rate of robberies with 171.0 per 100,000
persons. Russell County had the highest rate of
rapes with 77.6 per 100,000 persons.
3
Figure 11.1 – The breakdown of firearm-related violent
deaths by cause of death for 2019. Source: AL Law
Enforcement Agency UCR.
Larceny
Burglary
Assault
Robbery
Rape
Homicide
83,178
22,689
17,329
3,282
430
1,886
Violent Deaths
Violent death is defined as a death that results
from the intentional use of physical force or power
(threatened or actual) against oneself, another
person, group, or community.
4
In 2019, over 73,000 people died from violent deaths in
the U.S., and over 1,400 died in AL:
· In AL, males are four times more likely to die
from violent deaths than females (49.8 deaths
compared to 12.0deaths per 100,000 persons).
· In 2019, young adults under 45were more likely
to die than older adults.
· More white individuals died from violence in
2019; however, AA/black individuals had a higher
violent death rate.

2020 ALABAMA STATE HEALTH ASSESSMENT
64
· Lowndes and Wilcox counties had the highest
rate with 92.5deaths and 77.1 deaths per
100,000 persons, respectively.
5
Table 11.1 – Violent Death Rates, 2019
Count
Rate per
100,000
AL 1,483 30.2
U.S. 73,484 22.4
Public Health Districts
Northern 284 26.1
Northeastern 228 28.2
West Central 112 25.8
Jeerson 270 41.0
East Central 223 31.5
Southeastern 109 28.8
Southwestern 129 31.3
Mobile 128 31.0
Geographic Variation
N/A - -
Sex
Male 1,179 49.8
Female 304 12.0
Race
White 927 29.0
AA/black 505 38.9
Hispanic 34 15.2
Other/not provided 11 14.7
Household Income
N/A - -
Age (in years)
Under 18 73 6.7
18-24 210 46.9
25-34 297 45.9
35-44 292 49.2
45-54 220 35.7
55-64 176 26.8
65+ 215 25.3
Education
Less than high school 406 -
High school or GED 649 -
Some college 263 -
College graduate or higher 152 -
Firearm-Related Deaths
In 2019, AVDRS identified 1,050 deaths involving a firearm
or 21.4 per 100,000 persons:
· Of these deaths, 45.4 percent were homicides,
and 51.2 percent were suicides.
· Firearms were the cause of death for 82.4
percent of all homicides and 67.1 percent of all
suicides observed in AL during 2019.
· Over 690 firearm deaths occurred at homes,
farms, or residential areas. Other common
locations for firearm fatalities were motor vehicle-
related locations such as in vehicles, parking lots,
or streets and highways with over 170 deaths.
7
· In Figure 11.2, the data shows that firearms
contributed to more suicides/intentional self-
harm deaths (51.2 percent) than homicides (45.4
percent) in 2019.
· Firearm injuries inflicted by law enforcement
agents acting in the line of duty, unintentional
firearm deaths, and firearm deaths with
undetermined intent, constituted 3.4 percent of
all firearm deaths in 2019.
7
· According to CDC, 6 out of 10 firearm-related
deaths in AL were suicides, and 3 out of
10firearm deaths were homicides, and more
people suer non-fatal firearm-related injuries
than fatal injuries.
6
This data does not include non-fatal firearm-related injuries,
long-term eects of injury, or socioeconomic impacts.
Figure 11.2 – The breakdown of firearm-related violent
deaths by cause of death for 2019. Source: AVDRS.
Suicide or
Intentional Self-Harm
Homicide
Unintentional Firearm
Discharge
Legal Intervention/Death
of Undetermined Intent
51.2%
45.4%
2.5%
0.9%
Data Sources
Figure 11.1 – AL Violent Crimes, 2019. AL Law Enforcement
Agency, UCR, 2019. Data requested March 2021.
Table 11.1 – Violent Death Rates, 2019. ADPH, Center
for Health Statistics Mortality Files, 2019. Data requested
March 2021.
Figure 11.2 – Firearm-related Violent Deaths, 2019.
ADPH, AVDRS, 2019. Data requested March 2021.
Written Sources
1. CDC, Preventing Intimate Partner Violence, 2020.
2. FBI, UCR, 2019.

2020 ALABAMA STATE HEALTH ASSESSMENT
65
3 AL Law Enforcement Agency, UCR / Domestic
Violence in AL, 2019.
4. CDC, Violence Prevention, 2019
5. ADPH, Center for Health Statistics, 2019.
6. CDC, Firearm Violence Prevention, 2020.
7. ADPH, AVDRS, 2019.
Community Resources
2nd Chance, INC
Location: Etowah County, AL
Type: Domestic Violence Shelter
AL Appleseed Center for Law and Justice
Location: Montgomery County, AL
Type: Advocacy Program
AL Child Death Review System
Location: Statewide
Type: State Government Organization
AL Law Enforcement Agency
Location: Statewide
Type: State Government Organization
AVDRS
Location: Statewide
Type: State Government Organization
CDC Injury Center
Location: Atlanta, GA
Type: Federal Government Organization
Crisis Center of Russell County
Location: Russell County, AL
Type: Domestic Violence Shelter
Hope Place
Location: Madison County, AL
Type: Domestic Violence Shelter
Occupational Safety and Health Administration
Location: Washington, DC Metro
Type: Federal Government Organization
National Institute of Justice
Location: Washington, DC Metro
Type: Federal Government Organization
SafeHouse of Shelby County
Location: Shelby County, AL
Type: Domestic Violence Shelter
University of AL at Birmingham Injury Control
Research Center
Location: Jeerson County, AL
Type: Research Institution

2020 ALABAMA STATE HEALTH ASSESSMENT
66
12. Cancer
Ranked AL’s Twelfth Health Indicator
Alabamians identified cancer as the twelfth health
indicator in AL. Cancer, characterized by uncontrolled
growth and spread of abnormal cells, is the second
leading cause of death in AL. According to the American
Cancer Society
®
, an estimated 30,830 Alabamians will be
diagnosed with cancer in 2021, and an estimated 10,590
Alabamians will die from cancer in 2021.
1
The top four cancers in AL are colorectal, female breast,
lung/bronchus, and prostate cancers.
2
These cancers
represent more than 52 percent of all new tumors reported
to the AL Statewide Cancer Registry (ASCR) in 2018.
Additionally, the burden of each of these cancers could be
reduced through behavior modifications such as smoking
cessation, weight loss, exercise, and improved nutrition.
2
According to CDC, regular screening examinations by a
healthcare professional can help detect cancers early.
2
It is
recommended to follow-up with a doctor during annual visits
for mammograms, prostate screenings, and colonoscopies.
Vulnerable Populations
In AL, males have slightly less than a 1 in 2 risk of developing
any cancer over the course of a lifetime. For women, the
risk is a little more than 1 in 3 for developing any cancer
over the course of a lifetime.
2
The risk of being diagnosed
with cancer increases with age, and more than three-
fourths of all cancers are diagnosed in persons 55 years
of age and older. Family history and lifestyle choices
can aect the frequency and age at which someone
may need to be screened for cancer. For example, CDC
recommends yearly lung cancer screenings if you formerly
were or currently are a heavy smoker.
2
Geographic Variation
Physical access to cancer centers for the initial and
follow-up appointments is a barrier for at-risk and new
cancer patients.
3
Rural areas have a higher lung cancer
incidence, colorectal cancer incidence, cervical cancer
incidence, and overall cancer mortality rates compared
to urban areas between 2014-2018.
Topics Addressed for This Indicator are:
· Overall cancer mortality.
· Colorectal cancer incidence.
· Breast cancer incidence.
· Lung and bronchus cancer incidence.
· Prostate cancer incidence.
· Cervical cancer incidence.
Highlights
Data are retrieved from ASCR for all cancer cases
diagnosed or treated in AL. Mortality statistics are from
ADPH Center for Health Statistics Mortality Files:
· Although the overall cancer mortality rate for AL
declined for the past few years, Alabamians have
higher overall cancer mortality rates than the U.S.
· In AL, lung cancer incidence rates are significantly
higher than the U.S. average.
· In AL, AA/black females have significantly higher rates
of breast cancer incidence than white females.
· Prostate cancer is the most common cancer
in men. Prostate cancer incidence in AL has
declined over the past few years most likely due
to changes in screening guidelines resulting in
fewer men screened.
· In AL, prostate cancer occurs significantly more
in AA/black males than white males.
· The West Central Public Health District has the
highest rates of cervical cancer between 2014-2018.
Risk Factors:
· Age over 60 years old.
· Family history.
· Immune system deficiency.
· Genetics.
· Alcohol use.
· Smoking.
Overall Cancer Mortality
In 2019, the AL age-adjusted cancer mortality rate was
209.3 deaths per 100,000 persons and was higher
than the national average of 182.7 deaths per 100,000
persons. In the 2015 CHA, the AL rate was 184.5deaths
per 100,000persons:
· Although the overall cancer mortality rate for AL
declined for the past few years, Alabamians have
higher overall cancer mortality rates than the U.S.
· AL’s Southwestern Public Health District had the
highest cancer mortality rate.
· Rural areas had drastically increased rates
from the previous CHA to 2019 (188.8 deaths
compared to 233.4deaths per 100,000persons).
· Males had a higher mortality rate than females
(236.5 deaths compared to183.8deaths per
100,000 persons).

2020 ALABAMA STATE HEALTH ASSESSMENT
67
· In the previous CHA, there was a larger disparity
between males and females. The rate for
males was 237.2deaths per 100,000persons,
compared to females with 147.0deaths per
100,000persons.
· White individuals had a higher mortality rate than
AA/black individuals (239.7 deaths compared to
189.9deaths per 100,000persons).
Table 12.1 – Cancer Mortality Rate, 2019
Count
Rate per
100,000
AL 10,263 209.3
U.S. 599,601 182.7
Public Health Districts
Northern 2,220 203.8
Northeastern 1,740 215.0
West Central 859 198.0
Jeerson 1,334 202.6
East Central 1,425 201.2
Southeastern 835 220.4
Southwestern 969 235.4
Mobile 881 213.2
Geographic Variation
Rural 4,916 233.4
Urban 5,347 191.2
Sex
Male 5,605 236.5
Female 4,658 183.8
Race
White 7,671 239.7
AA/black 2,464 189.9
Household Income
N/A - -
Age (in years)
18-24 - -
25-34 57 8.8
35-44 167 28.1
45-54 626 101.5
55-64 2,093 318.2
65+ 7,292 858.0
Education
Less than high school 2,307 -
High school or GED 4,346 -
Some college 1,925 -
College graduate or higher 1,605 -
Colorectal Cancer Incidence
Colorectal cancer is the third leading cancer occurring
in white males, white females, and AA/black males.
Colorectal cancer was the second leading cancer in AA/
black females in 2018:
4
· Alabamians had higher incidence rates of
colorectal cancer than the U.S.
· Colorectal cancer occurred significantly more
frequently in males than females.
· Colorectal cancer occurred more frequently in
AA/black individuals than in white individuals.
Regular screenings allow for early detection, removal
of colorectal polyps before they become cancerous,
and detect cancer at an early stage where survival is
more likely. Screenings could potentially lower both the
incidence and mortality of this disease.
Table 12.2 – Colorectal Cancer, 2014-2018
Rate per 100,000
AL 42.9
U.S. 38.0
Public Health Districts
Northern 41.6
Northeastern 44.0
West Central 45.1
Jeerson 38.1
East Central 42.5
Southeastern 41.1
Southwestern 45.4
Mobile 45.9
Geographic Variation
Rural 44.4
Urban 41.1
Sex
Female 37.6
Male 49.3
Race
AA/black 48.2
Asian or Pacific Islander 28.4
White 41.0
Household Income
N/A -
Age (in years)
Under 50 10.1
50-64 86.7
65+ 178.6
Education
N/A -

2020 ALABAMA STATE HEALTH ASSESSMENT
68
Breast Cancer Incidence
Breast cancer is the most common cancer in females
and occurs far more frequently in females than males:
5
· The Northeastern Public Health District had the
lowest breast cancer incidence rate in AL (113.5
per 100,000 persons).
· In AL, AA/black females had higher incidence
rates than white females.
6
· Asian/Pacific Islander females in AL had
significantly lower breast cancer rates than white
or AA/black females. This is consistent with the
U.S. average.
6
Mammography can detect breast cancer early when
treatment is more eective, and a cure is more likely.
5
Table 12.3 – Breast Cancer, 2014-2018
Rate per 100,000
AL 121.4
U.S. 127.4
Public Health Districts
Northern 122.9
Northeastern 113.5
West Central 121.6
Jeerson 131.1
East Central 114.0
Southeastern 121.7
Southwestern 128.4
Mobile 118.4
Geographic Variation
Rural 119.6
Urban 122.3
Sex
Female 121.4
Male 1.6
Race
AA/black 126.3
Asian or Pacific Islander 70.6
White 118.9
Household Income
N/A -
Age (in years)
Under 50 43.7
50-64 256.9
65+ 405.5
Education
N/A -
Lung and Bronchus Cancer Incidence
Lung cancer is the second most common cancer in white
males, white females, and AA/black males. Lung cancer is
the third most common cancer in AA/black females:
7
· Alabamians have significantly higher incidence
rates for lung cancer than the U.S.
· Rural areas have higher incidence rates of lung
cancer compared to urban areas (68.9 new cases
compared to 59.0 new cases per 100,000 persons).
Smoking is the leading cause of developing lung cancer
(see Health Indicator 14: Tobacco and Vaping):
7
· Alabamians have a higher prevalence of smoking
than the U.S.
8
· Males have significantly higher lung cancer rates
and smoking prevalence than females.
8
Radon is the second leading cause of lung cancer and the
number one cause of lung cancer among non-smokers:
7
· In AL, 15counties have been designated as Zone1
Radon counties, meaning they have the highest
potential for elevated radon levels.
9
For more
information on radon levels, visit the ADPH website.
Table 12.4 – Lung Cancer, 2014-2018
Rate per 100,000
AL 63.7
U.S. 51.4
Public Health Districts
Northern 64.9
Northeastern 65.3
West Central 66.3
Jeerson 58.9
East Central 60.6
Southeastern 66.8
Southwestern 63.1
Mobile 63.6
Geographic Variation
Rural 68.9
Urban 59.0
Sex
Female 49.6
Male 81.9
Race
AA/black 55.9
Asian or Pacific Islander 35.6
White 66.2

2020 ALABAMA STATE HEALTH ASSESSMENT
69
Household Income
N/A -
Age (in years)
Under 50 3.8
50-64 121.6
65+ 338.0
Education
N/A -
Prostate Cancer Incidence
Prostate cancer is the most common cancer in males.
10
In 2018, prostate cancer occurred approximately
75percent more frequently in AA/black males than
white males in the U.S.:
· Jeerson County Health District has the highest
rate of prostate cancer incidence (157.5 cases
per 100,000 persons).
· In AL, most prostate cancer cases are diagnosed
in males older than 65 years old population
(597.2 cases per 100,000 persons).
11
· In AL, prostate cancer occurs significantly more
in AA/black males than white males.
Prostate cancer incidence in AL has declined over the
past few years most likely due to changes in screening
guidelines resulting in fewer men screened.
10
Table 12.5 – Prostate Cancer, 2014-2018
Rate per 100,000
AL 122.0
U.S. 108.2
Public Health Districts
Northern 97.6
Northeastern 116.3
West Central 136.8
Jeerson 157.5
East Central 134.5
Southeastern 121.1
Southwestern 107.5
Mobile 96.6
Geographic Variation
Rural 109.3
Urban 128.1
Sex
Female -
Male 122.0
Race
AA/black 186.4
Asian or Pacific Islander 64.3
White 97.8
Household Income
N/A -
Age (in years)
Under 50 6.1
50-64 280.8
65+ 597.2
Education
N/A -
Cervical Cancer Incidence
Although all females are at risk for cervical cancer, it
occurs most often in women over 30 years old.
12
Cervical
cancer is routinely screened during primary care visits:
13
· The West Central and Southwestern Public
Health districts have the highest incidence rates
of cervical cancer between 2014-2018.
· Rural areas have higher rates of cervical cancer
than urban areas (10.1 new cases compared to
8.8 new cases per 100,000).
· The age group with the highest incidence was
ages 50-64 years old.
A pap smear screening test is recommended to be
completed every three years and can help detect early
stages of cervical cancer. The HPV vaccine can help
prevent cervical cancer.
12
Table 12.6 – Cervical Cancer, 2014-2018
Rate per 100,000
AL 9.4
U.S. 7.6
Public Health Districts
Northern 8.5
Northeastern 10.1
West Central 10.9
Jeerson 7.6
East Central 10.1
Southeastern 9.5
Southwestern 10.7
Mobile 9.0

2020 ALABAMA STATE HEALTH ASSESSMENT
70
Geographic Variation
Rural 10.1
Urban 8.8
Sex
Female 9.4
Male -
Race
AA/black 9.8
Asian or Pacific Islander 7.9
White 9.2
Household Income
N/A -
Age (in years)
Under 50 8.3
50-64 13.5
65+ 10.8
Education
N/A -
Data Sources
Table 12.1 – Cancer Mortality Rate, 2019. ADPH, Center
for Health Statistics Mortality Files, 2019. Data requested
March 2021.
Table 12.2 – Colorectal Cancer, 2014-2018. ADPH, Cancer
Epidemiology Division, 2021. Data requested July 2021.
Table 12.3 – Breast Cancer, 2014-2018. ADPH, Cancer
Epidemiology Division, 2021. Data requested July 2021.
Table 12.4 – Lung Cancer, 2014-2018. ADPH, Cancer
Epidemiology Division, 2021. Data requested July 2021.
Table 12.5 – Prostate Cancer, 2014-2018. ADPH, Cancer
Epidemiology Division, 2021. Data requested July 2021.
Table 12.6 – Cervical Cancer, 2014-2018. ADPH, Cancer
Epidemiology Division, 2021. Data requested July 2021.
Written Sources
1. American Cancer Society, Cancer Facts – Incidence,
2018.
2. CDC, Cancer Data and Statistics, 2021.
3. Rural Health Information Hub, Healthcare Access in
Rural Community, 2020.
4. CDC, Colorectal Cancer, 2020.
5. CDC, Breast Cancer, 2020.
6. National Cancer Institute, Surveillance, Epidemiology,
and End Results Program, Recent Trends in SEER Age-
Adjusted Incidence Rates, 2000-2018, 2021.
7. CDC, Lung and Bronchus Cancer, 2020.
8. CDC, BRFSS Smoking Module, 2019.
9. ADPH, Radon in AL, 2019.
10. CDC, Prostate Cancer, 2020.
11. ADPH, Prostate Cancer Risk Factors, 2020.
12. CDC, Basic Information about Cervical Cancer, 2021.
13. NIH Surveillance, Epidemiology, and End Results
Program, Cervix Uteri Recent Trends in Age-Adjusted
Incidence Rates, 2018.
Community Resources
AL Breast and Cervical Cancer Early Detection Program
Location: Montgomery County, AL
Type: Advocacy Program
American Cancer Society
®
Location: Jeerson County, AL
Type: Non-profit Organization
American Association for Cancer Research
Location: Philadelphia, PA
Type: Research Institution
American Lung Association Central Branch
Location: Jeerson County, AL
Type: Advocacy Program
Bullock County Community Health Advisors
Location: Bullock County, AL
Type: Non-profit Organization
Steel Magnolias Breast Cancer
Location: Calhoun County, AL
Type: Non-profit Organization
Susan G. Komen Breast Cancer
Location: Dallas, TX
Type: Non-profit Organization

2020 ALABAMA STATE HEALTH ASSESSMENT
71
13. Diabetes
Ranked AL’s Thirteenth Health Indicator
Diabetes is a serious health condition and was AL’s
seventh leading cause of death in 2019. Diabetes can
be classified into three main types – Type 1, Type2, and
gestational. The majority of individuals with diabetes
have Type 2 diabetes (90-95percent).
1
Type 2 diabetes,
means an individual’s body cannot make enough insulin
to control the body’s blood sugar levels.
Individuals most at-risk for Type 2 diabetes are those
diagnosed with prediabetes.
1
Prediabetes is when an
individual’s blood sugar is chronically higher than normal,
but not severe enough for a diabetes diagnosis.
1
People
with prediabetes can still reverse the condition with
lifestyle changes. Gestational diabetes develops during
pregnancy and could pose a health risk to the infant.
1
Many people with diabetes can manage their condition
with a consistent, healthy diet and regular exercise, if
the condition is detected early.
2
Due to low screening
rates and access to health services, diabetes is
often diagnosed when it begins to have serious
health consequences.
1
Diabetes is highly linked to
obesity and lack of exercise and has many associated
comorbidities, including heart disease and some eye
conditions. The disease can result in limb amputation
and the need for dialysis.
1
Vulnerable Populations
According to CDC, “more than 34 million people in the
U.S. have diabetes, and 1 in 5 of [those individuals] don’t
know they have it.”
1
Diabetes takes a heavy toll in the AA/
black population and in older adults. Almost one-fifth of
AA/black individuals and one-fourth of elderly people
have diabetes in AL.
3
Geographic Variation
Diabetes was especially prevalent in rural areas. Most
of the central AL counties were considered as part of
the U.S. Diabetes Belt, an area with considerably high
diabetes occurrence among adults.
Topics Addressed for This Indicator are:
·
Alabamians ever told they have diabetes.
·
Diabetes among Medicare recipients.
·
Diabetes diagnosis in Medicaid recipients.
·
BCBS members with diabetes-related claims.
·
Diabetes-related mortality.
Highlights
Data are retrieved from BCBS Claims, the Centers for
M
edicare and Medicaid Services, AL Medicaid Agency, BRFSS,
and the ADPH Center for Health Statistics Mortality Files:
·
According to BRFSS, 13.9 percent of AL’s adult
population report they have been told they
have diabetes.
·
There was an increase in self-reported
prevalence among AA/black individuals when
compared to white individuals.
·
The Southwestern Public Health District had the
highest percentage of diabetes diagnoses among
their Medicaid recipients at 5.8 percent.
·
The rate of diabetes mortality in rural areas was
30.4 deaths per 100,000 persons, compared to
urban areas 20.8 deaths per 100,000persons.
Risk Factors:
·
Age.
·
Family history.
·
Overweight.
·
Physical inactivity.
·
High blood pressure/low high-density
lipoprotein/high triglycerides.
·
Minority race/ethnicity.
·
Pregnancy.
Adults Ever Told They Have Diabetes
The statewide prevalence of persons who report they
have been told they have diabetes was 13.9 percent
compared to the U.S. prevalence of 10.8percent:
·
There was a higher prevalence among AA/black
individuals (17.3 percent) when compared to
white individuals (13.3percent).
·
Geographically, data suggests that areas in the
southern part of AL had a higher prevalence of
reported diabetes. For example, 12.2 percent of
adults in the Northeastern Public Health District
reported being diagnosed with diabetes; however,
16.4 percent of Southeastern Public Health District
reported being diagnosed with diabetes.
·
Individuals within lower income brackets and
lower education status are increasingly more at
risk for diabetes.
·
In 2019, 25.9 percent of Alabamians 65years or
older were told they had diabetes.
Adults told they had pre-diabetes and women who had
diabetes only during pregnancy were excluded from
being classified as diagnosed.

2020 ALABAMA STATE HEALTH ASSESSMENT
72
Table 13.1 – Percentage of Adults Ever
Told They Have Diabetes, 2019
% 95% CI
AL 13.9 (13.0-14.9)
U.S. 10.8 -
Public Health Districts
Northern 13.5 (11.1-15.9)
Northeastern 12.2 (10.0-14.3)
West Central 13.3 (10.7-16.0)
Jeerson 12.4 (10.1-14.7)
East Central 17.1 (14.2-20.1)
Southeastern 16.4 (13.6-19.3)
Southwestern 14.4 (11.8-17.0)
Mobile 13.5 (11.1-15.9)
Geographic Variation
N/A - -
Sex
Male 14.1 (12.6-15.6)
Female 13.8 (12.6-15.1)
Race
White 13.3 (12.2-14.4)
AA/black 17.3 (15.3-19.3)
Household Income
Less than $15,000 21.2 (17.5-24.9)
$15,000-24,999 17.4 (14.7-20.1)
$25,000-34,999 17.2 (13.4-21.0)
$35,000-49,999 11.5 (9.2-13.9)
$50,000-74,999 10.8 (9.5-12.2)
Age (in years)
35-44 6.5 (4.5-8.6)
45-54 14.7 (12.1-17.2)
55-64 25.3 (22.5-28.2)
65+ 25.9 (23.8-27.9)
Education
Less than high school 19.3 (15.7-22.8)
High school or GED 15.2 (13.5-17.0)
Some college 12.5 (11.0-14.0)
College graduate or higher 11.0 (9.6-12.4)
Diabetes Among Medicare
Recipients
Diabetes is an age-related disease, meaning the risk
of being diagnosed increases in elderly populations.
1
The state prevalence for diabetes in AL Medicare
recipients was 30.2percent for 2018. In the 2015 CHA, the
prevalence was 29.7 percent:
· Perry County had the highest diabetes prevalence
(38.7percent) in Medicare recipients for 2018,
followed by Marengo County (38.6percent), and
Conecuh County (38.0percent).
· Baldwin County had the lowest diabetes
diagnosis prevalence, with 23.5 percent of
Medicare recipients having been diagnosed.
Additional demographic information was not available.
Figure 13.1 – This map displays the percent of diabetes
recipients by county. Medicare provides insurance to
persons over the age of 65 years old. Source: Centers
for Medicare and Medicaid Services..
Lauderdale
Colbert
Franklin
Marion
Winston
Walker
Limestone
Lawrence
Morgan
Cullman
Madison
Jackson
28.7
31.1
29.0
34.2
32.9
32.4
37.0
31.9
28.9
30.3
29.8
31.5
28.7
30.5
30.4
31.5
32.6
32.4
34.7
29.7
30.6
30.7
33.4
28.2
30.5
25.9
29.7
33.9
36.1
37.9
33.0
38.7
32.6
29.5
30.7
28.1
35.0
29.3
35.9
35.1
38.0
32.6
31.8
32.7
36.8
33.1
38.0
34.4
33.1
31.1
32.0
32.0
30.3
30.9
31.2
29.6
28.0
23..5
28.8
31.0
34.9
38.6
36.5
34.7
29.2
34.4
26.7
Marshall
DeKalb
Cherokee
Etowah
Blount
St. Clair
Calhoun
Cleburne
Clay
Talladega
Randolph
Chambers
Tallapoosa
Coosa
Jeerson
Lamar
Fayette
Tuscaloosa
Bibb
Hale
Sumter
Perry
Dallas
Marengo
Choctaw
Washington
Clarke
Monroe
Conecuh
Butler
Crenshaw
Pike
Barbour
Henry
Dale
Coee
Geneva
Prevalence (%)
Houston
Covington
Escambia
Baldwin
Mobile
Wilcox
Lowndes
Montgomery
Autauga
Chilton
Elmore
Macon
Bullock
Russell
Lee
Greene
Pickens
Shelby
40.020.0
Diabetes Diagnosis in Medicaid
Recipients
AL’s Medicaid adult and adolescent populations had 4.1
percent of recipients with diabetes-related diagnoses in
AL in 2018:

2020 ALABAMA STATE HEALTH ASSESSMENT
73
· The Southwestern public health District had the
highest percentage of diabetes diagnoses among
their Medicaid recipients at 5.8 percent.
· Of those claims, females were twice as likely to
have a diabetes diagnosis compared to males.
· The prevalence of white and AA/black individuals
with a diabetes diagnosis, although lower, was
similar to 2017.
For the district level, only confirmed county diagnoses
were included in the calculation.
Table 13.2 – Percentage of Diabetes Among
Medicaid Recipients, 2018
Count %
AL 48,908 4.1
U.S. - -
Public Health Districts
Northern 9,616 4.1
Northeastern 7,184 3.7
West Central
5,862 4.8
Jeerson
4,388 2.7
East Central 6,643 3.5
Southeastern 5,590 4.8
Southwestern 5,508 5.8
Mobile 3,685 3.1
Geographic Variation
N/A - -
Sex
Female 33,934 -
Male 14,968 -
Race
White 21,167 -
Asian or Pacific Islander 292 -
AA/black 22,318 -
American Indian/Alaska
Native
112 -
Hispanic 497 -
Unknown or other 4,522 -
Household Income
N/A - -
Age (in years)
Under 21 2,899 -
21 and over 46,009 -
Education
N/A - -
Blue Cross and Blue Shield Members
with Diabetes-related Claims
In 2017, the total direct medical expenses for diagnosed
diabetes in AL were estimated at 4.2 billion dollars.
4
BCBS
is the largest private insurance providers for AL. Roughly,
10percent of BCBS members had claims related to
diabetes management or hospitalizations each year
between 2016 and 2019.
The BCBS claim usage has increased steadily since 2016.
Diabetes claims include eye exams, statin therapy, lipid
test, and A1C testing:
· The West Central Public Health District had the
highest percent of BCBS members who had
diabetes claims, followed by East Central and
Southeastern public health districts in 2019.
Table 13.3 – Percentage of BCBS Members
with Diabetes-related Claims, 2016-2019
2016 2017 2018 2019
AL 9.4 10.2 10.2 10.4
U.S. - - - -
Public Health Districts
Northern 8.4 9.1 9.2 9.6
Northeastern 8.7 9.5 9.4 9.6
West Central 10.9 11.2 11.7 11.9
Jeerson 9.0 9.8 9.4 9.4
East Central 10.5 11.4 11.6 11.7
Southeastern 10.4 11.3 11.4 11.7
Southwestern 9.9 10.6 10.7 11.2
Mobile 9.8 10.6 10.7 10.8
Geographic Variation
Rural 10.0 10.8 11.0 11.3
Urban 9.0 9.7 9.7 9.8
Sex
N/A - - - -
Race
N/A - - - -
Household Income
N/A - - - -
Age (in years)
N/A - - - -
Education
N/A - - - -

2020 ALABAMA STATE HEALTH ASSESSMENT
74
Diabetes-related Mortality
Diabetes mortality was defined as death due to
a diabetes-related illness, not necessarily as an
underlying disease. In AL, the diabetes mortality rate was
24.9deaths per 100,000 persons in 2019:
· East Central Public Health District had
the highest rate of diabetes mortality with
43.2deaths per 100,000 persons.
· Wilcox County (Southwestern Public Health
District) had the highest rate of diabetes
mortality with 86.8deaths per 100,000persons.
· The rate of diabetes mortality in rural areas was
30.4 deaths per 100,000persons, compared to
urban areas 20.8 deaths per 100,000persons.
· After age of 65 years old, the diabetes crude
mortality rate almost triples from the previous
age bracket to 92.8 deaths per 100,000persons.
Table 13.4 – Diabetes-related Mortality, 2019
Count
Rate per
100,000
AL 1,223 24.9
U.S. 87,647 26.7
Public Health Districts
Northern 226
20.7
Northeastern 138 17.0
West Central 74 17.1
Jeerson 140 21.3
East Central 306 43.2
Southeastern 124 32.7
Southwestern 121 29.4
Mobile 94 22.7
Geographic Variation
Rural 641 30.4
Urban 582 20.8
Sex
Male 705 29.8
Female 518 20.4
Race
White 747 23.3
AA/black 458 35.3
Hispanic 8 3.6
Household Income
N/A - -
Age (in years)
25-35 22 3.4
35-44 45 7.6
45-54 110 17.8
55-64 253 38.5
65+ 789 92.8
Education
Less than high school 296 -
High school or GED 524 -
Some college 225 -
College graduate or higher 162 -
Data Sources
Table 13.1 – Percentage of Adults Ever Told They Have
Diabetes, 2019. ADPH, BRFSS, 2019. Data requested
March 2021.
Figure 13.1 – Diabetes Among Medicare Recipients,
2018. Centers for Medicare and Medicaid Services, 2019.
Data requested December 2020.
Table 13.2 – Percentage of Diabetes Among Medicaid
Recipients, 2018. AL Medicaid Agency, 2018. Data
requested July 2020.
Table 13.3 – Percentage of BCBS Members with
Diabetes–related Claims, 2016-2019. BCBS, Members
Diabetes Claims, 2019. Data requested October 2020.
Table 13.4 – Diabetes–related Mortality, 2019. ADPH,
Center for Health Statistics Mortality Files, 2019. Data
requested March 2021.
Written Sources
1. CDC, Diabetes Prevention, 2020.
2. ADPH, Diabetes General Information, 2021.
3. CDC, BRFSS Diabetes Module, 2019.
4. American Diabetes Association,
®
Economic Cost of
Diabetes in the U.S. in 2017, 2018.
Community Resources
AL Safe at School Diabetic Curriculum
Location: Montgomery County, AL
Type: Educational Resource
American Diabetes Association
®
Location: Washington, DC Metro
Type: Non-profit Organization
Association of Diabetes Care and Education Specialists
Location: Chicago, IL
Type: Educational Resource
CDC National Diabetes Prevention Program
Location: Atlanta, GA
Type: Federal Government Program
Diabetes Research Institute Foundation
Location: Miami, FL
Type: Non-profit Organization
Juvenile Diabetes Federation
Location: New York, NY
Type: Non-profit Organization

2020 ALABAMA STATE HEALTH ASSESSMENT
75
14. Tobacco Usage and Vaping
Ranked AL’s Fourteenth Health Indicator
Tobacco usage and vaping was ranked AL’s fourteenth
health indicator and has consistently been a public
health concern since the 1960s. Smoking is the leading
cause of preventable disease and death.
1
While the
67 percent national decrease in current cigarette
smokers since 1965 is considered a great public health
achievement, tobacco-related disparities persist.
2
Emerging vaping tobacco products, such as JUUL,
led to increased youth initiation and exposure to
harmful chemicals, such as heavy metals, volatile
organic compounds, diacetyl, and nicotine.
4
Electronic
cigarettes or vaping products can also contain
tetrahydrocannabinol and other drugs. The long-term
eects of e-cigarettes are still unknown.
In August 2019, ADPH began receiving reports from
healthcare providers of suspected lung injury cases related
to e-cigarette, or vaping products. ADPH began working with
CDC and the Food and Drug Administration (FDA) as part of
a multistate outbreak investigation related to e-cigarette or
vaping use-associated lung injury (EVALI).
5
Vulnerable Populations
According to CDC, nicotine can harm adolescent and
young adult brain development. Minority populations
suer disproportionally from smoke-related diseases
such as CVDs, cancer, diabetes, and pulmonary diseases.
Nicotine is also a health danger for pregnant adults and
their developing infants.
Geographic Variation
In the U.S., current cigarette smoking is the highest in the
Midwest (16.4 percent) and the South (15.4 percent).
Smoking is banned in many public settings in major
cities, but vaping may still be allowed. The full impact of
secondhand smoke eects remains unknown.
Topics Addressed for This Indicator are:
· Current adult tobacco smokers.
· Adult nicotine product use.
· Current high school student smokers.
· High school students vaping.
Highlights
Data are retrieved from BRFSS, the AL Adult Tobacco
Survey, and the Youth Risk Behavioral Surveillance
System (YRBSS):
· Individuals who have less than a high school
education and individuals who have an income
less than $15,000 per year are more likely to be
current smokers.
· Currently, the prevalence of AL high school
students using cigarettes is 7.1percent, and the
prevalence of those using smokeless tobacco
products is 8.9 percent.
· According to YRBSS, over half of AL high school
students tried using a vaping device in 2019.
· The percentage of AL high school students who
ever used electronic vapor products was higher
among whites and Hispanics students than AA/
black students.
Risk Factors:
· High-stress atmosphere.
· Family usage.
· Race/ethnicity.
· Socioeconomic factors/education.
Current Adult Cigarette Smokers
While the statewide prevalence for current smokers
remains consistently higher than the U.S. average, the
overall prevalence decreased. In 2019, the percentage
of current adult smokers was 20.2percent compared to
23.8percent in the 2015CHA. Two criteria define current
smokers: (1) all adults that have ever smoked at least 100
cigarettes or 5packs in their lifetime, and (2) individuals
that smoke now, every day or some days:
· In 2019, AL had the ninth highest adult smoking
prevalence rate in the U.S. (20.2percent),
contributing to 8,600adult deaths.
· Males are more likely to self-report smoking than
females (22.4compared to18.4 percent in 2019).
· Individuals with less than a high school education
and individuals with an income less than $15,000per
year are more likely to be current smokers.
Since 2011, the percent of adults who currently smoke
has declined in AL.
Table 14.1 – Percentage of Adults
Who Are Current Smokers, 2019
% 95% CI
AL 20.2 (18.9-21.6)
U.S. 16.0 -
Public Health Districts
Northern 19.1 (15.8-22.5)
Northeastern 22.9 (19.4-26.4)
West Central 21.3 (17.6-24.9)
Jeerson 18.6 (15.0-22.3)

2020 ALABAMA STATE HEALTH ASSESSMENT
76
East Central 17.7 (14.2-21.2)
Southeastern 24.3 (20.0-28.7)
Southwestern 20.3 (16.5-24.2)
Mobile 19.7 (16.2-23.2)
Geographic Variation
N/A - -
Sex
Male 22.4 (20.3-24.5)
Female 18.4 (16.6-20.1)
Race
White 19.8 (18.2-21.4)
AA/black 20.3 (17.6-23.0)
Household Income
Less than $15,000 33.1 (28.3-37.9)
$15,000-24,999 31.5 (27.3-35.6)
$25,000-34,999 21.9 (17.1-26.7)
$35,000-49,999 18.8 (15.0-22.6)
$50,000-74,999 13.2 (11.4-15.0)
Age (in years)
18-24 12.6 (8.5-16.7)
25-34 28.4 (24.1-32.7)
35-44 28.3 (24.5-32.1)
45-54 20.6 (17.6-23.7)
55-64 22.8 (19.8-25.7)
65+ 10.8 (9.3-12.4)
Education
Less than high school 35.1 (30.1-40.2)
High school or GED 24.3 (21.8-26.8)
Some college 18.4 (16.2-20.6)
College graduate or higher 8.0 (6.6-9.3)
Adult Nicotine Product Use
In 2019, the state law was updated to set the minimum
age to purchase any tobacco products to 21years old.
7
Most individuals bought their electronic tobacco devices
at specific vape shops, convenience stores, online/
internet, and tobacco smoke shop/specialty stores. A
significant number of individuals received products from
a friend or family member:
· The highest percent of nicotine product use was
cigarettes (56.7 percent), followed by cigars (35.1
percent) and smokeless tobacco (22.8 percent).
· Nearly 7 percent of e-cigarette users reported
using in the past 30 days. The Adult Tobacco
Survey reported that 13.6 percent of AL adults
are curious about vaping. One-third of adults
described the main reason for trying e-cigarettes
was to stop using other nicotine products.
Current High School Students
Smokers
Smoking at an early age can have a severe and adverse
impact on an individual’s health later in life. The 2019
YRBSS included questions about cigarettes, cigars,
smokeless tobacco, shisha/hookah, and electronic vapor
products usage for high school students. Since 1995, the
overall prevalence of current smokers among high school
students declined by more than half since 2013:
· In 2019, the prevalence of AL high school
students using cigarettes is 7.1percent, and the
prevalence of those using smokeless tobacco
products was 8.9 percent.
7
Table 14.2 – Summary of Nicotine Product Use, 2019
Percent of total
who ever used
If ever used,
percent who use
every day
Percent of total
who used in past
30 days
If used in past
30 days, percent
who used
flavored product
If used in past
30 days, percent
who tried to quit
in past 12 months
Cigarettes 56.7 27.2 19.4 1.5 42.3
Cigars 35.1 3.2 5.5 59.0 57.9
E-cigarettes 21.6 3.0 6.9 59.5 30.6
Smokeless
tobacco
22.8 19.9 4.6 66.2 27.2
Regular pipe 9.6 10.4 0.9 70.1 81.5
Water pipe 8.6 8.2 1.1 77.5 75.0

2020 ALABAMA STATE HEALTH ASSESSMENT
77
· Marketing and flavoring of tobacco products
make them more appealing to youth. About
16.5percent of AL high school students reported
seeing tobacco products advertised when they
use the internet.
7
· New formulations of these products contain
higher levels of nicotine. Nicotine is a highly
addictive substance. Almost half (48.2 percent)
of AL high school students tried to quit using any
tobacco products in the past year.
7
Figure 14.1 – The figure displays the percentage of AL
high school students who currently smoke cigarettes.
AL obtained weighted data every year it administered
the survey except for 2007 and 2017. Source: YRBSS.
1995
1997
1999
2001
2003
2005
2007 *
2009
2011
2013
2015
2017 *
2019
31.0
32.8
36.6
23.7
24.7
24.4
20.8
22.9
18.0
14.0
7.1
High School Students Vaping
Vaping includes e-cigarettes, e-cigars, e-pipes, vape
pipes, vaping pens, e-hookahs, and hookah pens (blue,
NJOY, or Starbuzz):
· Approximately 54 percent of high school students
reported ever using electronic vapor products at
least once, a significant increase from the 41 percent
in 2015. No dierence was reported between the
percentage of male and female vapers.
· Twelfth graders were most likely to have ever
used electronic vapor products. Trying electronic
vapor products was more prevalent among both
Hispanic and White high school students.
· No significant dierence was reported with high
school students who currently use electronic
vapor products between 2015-2019.
7
· In 2019, over 10 percent of high school students
obtained their own electronic vapor products by
purchasing them in a local store.
7
Figure 14.2 – The figure displays the percentage of AL
high school students who ever used an electronic vapor
product. Abbreviated words are African American/black
(AA/B), white (W), and Hispanic (H). Source: YRBSS.
Total
Male
Female
9th
10th
11th
12th
AA/B
W
H
57.5
57.3
48.3
60.3
56.7
50.3
53.8
54.4
54.4
51.0
Data Sources
Table 14.1 – Percentage of Adults Who Are Current
Smokers, 2019. ADPH, BRFSS, 2019. Data requested
March 2021.
Table 14.2 – Summary of Nicotine Product Use, 2019.
AL Adult Tobacco Survey, 2019. Data requested July 2020.
Figure 14.1 –AL High School Students who Currently
Smoked Cigarettes, 1995-2019. ADPH, YRBSS, 2019.
Data requested July 2020.
Figure 14.2 –AL High School Students Using
Electronic Vapor Products, 2019. ADPH, YRBSS, 2019.
Data requested July 2020.
Written Sources
1. CDC, Smoking and Tobacco Use Health Eects, 2020.
2. CDC Newsroom, Cigarette Smoking Among U.S. Adults
Lowest Ever Recorded: 14 Percent in 2017, 2018.
3. CDC, Youth Tobacco Prevention, 2019.
4. CDC, Electronic Cigarettes, 2021.

2020 ALABAMA STATE HEALTH ASSESSMENT
78
5. CDC, Outbreak of Lung Injury Associated with the Use
of E-Cigarette, or Vaping, Products, 2020.
6. CDC, Secondhand Smoke, 2021.
7. ADPH, AL Tobacco Laws, 2020.
8. CDC, Online High School Youth Risk Behavior
Survey, 2019.
Community Resources
ADPH Tobacco Prevention and Control Program
Location: Montgomery County, AL
Type: State Government Organization
American Lung Association
®
Location: Jeerson County, AL
Type: Advocacy Program
Coalition for a Tobacco-Free AL
Location: Montgomery County, AL
Type: Non-profit Organization
CDC Smoking & Tobacco Use Surveys
Location: Atlanta, GA
Type: Federal Government Organization
FDA Tobacco Compliance Check
Location: Washington, DC Metro
Type: Federal Government Organization
National Quitline (1-800-QUIT-NOW)
Location: Nationwide
Type: Advocacy Program
River of Hope Ministries
Location: Autauga County, AL
Type: Non-profit Organization
Truth Initiative
Location: Montgomery County, AL
Type: Advocacy Program

2020 ALABAMA STATE HEALTH ASSESSMENT
79
Appendix
Additional tables and data sources can be
found in the Appendix. Health indicator data
are broken down by county level.

2020 ALABAMA STATE HEALTH ASSESSMENT
80
Detailed Alabama Economic and Demographic Data
AL’s Economic and Demographic Data, 2004-2020
Age (in years) 2005 2013 2019
0-17 1,113,083 (24.7%) 1,113,526 (23.0%) 1,085,597 (22.1%)
18-24 456,549 (10.1%) 483,673 (10.0%) 457,530 (9.3%)
25-34 583,109 (12.9%) 620,984 (12.8%) 637,403 (13.0%)
35-44 655,351 (14.6%) 607,139 (12.6%) 605,739 (12.4%)
45-54 639,357 (14.2%) 664,435 (13.7%) 609,391 (12.4%)
55-64 465,670 (10.3%) 622,799 (12.9%) 653,213 (13.4%)
65 or more 590,372 (13.1%) 721,166 (14.9%) 854,312 (17.4%)
Sex 2005 2013 2019
Female 2,324,069 (51.6%) 2,488,375 (51.5%) 2,533,574 (51.7%)
Male 2,179,422 (48.4%) 2,345,348 (48.5%) 2,369,611 (48.3%)
Rurality 2005 2013 2019
Rural county residents 1,824,813 (40.5%) 1,898,220 (39.3%) 2.106,245 (43.0%)
Urban county residents 2,678,678 (59.5%) 2,935,502 (60.7%) 2,796,940 (57.0%)
Racial Identification 2005 2013 2019
AA/Black 1,178,398 (26.2%) 1,284,102 (26.6%) 1,319,551 (26.9%)
American Indian/Alaska Native 25,920 (0.6%) 33,581 (0.7%) 23,265 (0.5%)
Asian 37,929 (0.8%) 61,859 (1.3%) 66,129 (1.3%)
Native Hawaiian and other Pacific Islander 2,625 (0.1%) 5,136 (0.1%) 1,892 (0.04%)
White 3,215,079 (71.4%) 3,376,295 (69.8%) 3,326,375 (67.8%)
Two or more races 43,540 (1.0%) 72,528 (1.5%) 91,522 (1.9%)
Ethnicity Identification 2005 2013 2019
Hispanic 103,472 (2.3%) 198,019 (4.1%) 219,296 (4.5%)
Non-Hispanic 4,400,019 (97.7%) 4,635,703 (97.7%) 4,683,889 (95.5%)
Education Status 2005 2013 2019
Less than 9th grade 187,473 (6.4%) 158,191 (4.9%) 130,320 (3.9%)
Did not complete high school, no diploma or GED 393,433 (13.4%) 340,457 (10.6%) 302,753 (9.0%)
Completed high school or GED 941,983 (32.0%) 1,001,134 (31.0%) 1,039,241 (30.9%)
Post high school 791,137 (26.9%) 968,712 (30.0%) 1,002,387 (29.8%)
College graduate 630,608 (21.4%) 756,953 (23.5%) 885,357 (26.3%)
Marital Status 2005 2013 2019
Never married 882,167 (24.9%) 1,184,204 (30.3%) 1,244,176 (31.1%)
Married 2,006,739 (567%) 1,948,025 (49.8%) 1,990,220 (49.7%)
Widowed 253,388 (7.2%) 289,224 (7.4%) 272,304 (6.8%)
Divorced 399,440 (11.3%) 489,545 (12.5%) 500,559 (12.5%)
Poverty Level 2006 2013 2019
Below the poverty level 742,064 (16.6%) 883,371 (18.7%) 739,108 (15.5%)
Above the poverty level 3,740,108 (83.4%) 3,832,734 (81.3%) 3,024,148 (84.5%)
Disability Diculties 2008 2013 2019
With a disability 744,472 (16.3%) 757,829 (15.9%) 765,018 (15.9%)
With a hearing diculty 199,230 (4.4%) 197,873 (4.2%) 212,724 (4.4%)
With a vision diculty 153,597 (3.4%) 143,177 (3.0%) 150,989 (3.1%)
With a cognitive diculty 293,533 (6.9%) 272,517 (6.1%) 284,282 (6.3%)
With an ambulatory diculty 438,988 (10.3%) 438,611 (9.8%) 421,440 (9.3%)
With a self-care diculty 160,221 (3.8%) 154,635 (3.5%) 147,580 (3.3%)
With an independent living diculty 288,205 (8.3%) 267,866 (7.3%) 275,237 (7.4%)

2020 ALABAMA STATE HEALTH ASSESSMENT
81
Detailed Alabama Economic and Demographic Data
AL’s Economic and Demographic Data, 2004-2020
Education Status 2005 2013 2019
Less than 9th grade 187,473 (6.4%) 158,191 (4.9%) 130,320 (3.9%)
Did not complete high school, no diploma or GED 393,433 (13.4%) 340,457 (10.6%) 302,753 (9.0%)
Completed high school or GED 941,983 (32.0%) 1,001,134 (31.0%) 1,039,241 (30.9%)
Post high school 791,137 (26.9%) 968,712 (30.0%) 1,002,387 (29.8%)
College graduate 630,608 (21.4%) 756,953 (23.5%) 885,357 (26.3%)
Marital Status 2005 2013 2019
Never married 882,167 (24.9%) 1,184,204 (30.3%) 1,244,176 (31.1%)
Married 2,006,739 (567%) 1,948,025 (49.8%) 1,990,220 (49.7%)
Widowed 253,388 (7.2%) 289,224 (7.4%) 272,304 (6.8%)
Divorced 399,440 (11.3%) 489,545 (12.5%) 500,559 (12.5%)
Poverty Level 2006 2013 2019
Below the poverty level 742,064 (16.6%) 883,371 (18.7%) 739,108 (15.5%)
Above the poverty level 3,740,108 (83.4%) 3,832,734 (81.3%) 3,024,148 (84.5%)
Disability Diculties 2008 2013 2019
With a disability 744,472 (16.3%) 757,829 (15.9%) 765,018 (15.9%)
With a hearing diculty 199,230 (4.4%) 197,873 (4.2%) 212,724 (4.4%)
With a vision diculty 153,597 (3.4%) 143,177 (3.0%) 150,989 (3.1%)
With a cognitive diculty 293,533 (6.9%) 272,517 (6.1%) 284,282 (6.3%)
With an ambulatory diculty 438,988 (10.3%) 438,611 (9.8%) 421,440 (9.3%)
With a self-care diculty 160,221 (3.8%) 154,635 (3.5%) 147,580 (3.3%)
With an independent living diculty 288,205 (8.3%) 267,866 (7.3%) 275,237 (7.4%)
Home Ownership 2005 2013 2019
Own 3,219,052 (72.5%) 3,248,599 (68.8%) 3,373,391 (68.8%)
Rent 1,223,506 (27.5%) 1,470,091 (31.1%) 1,529,794 (31.2%)
Employment Status 2004 2014 2019
Labor force 2,136,458 2,150,118 2,322,591
Employed 2,014,889 2,003,910 2,190,444
Unemployed 121,569 (5.7%) 146,208 (6.8%) 147,898 (4.9%)
Travel Time to Work 2005 2013 2019
Under 20 minutes 880,746 (46.0%) 856,564 (44.3%) 888,542 (43.1%)
20-35 minutes 739,125 (38.6%) 768,790 (39.8%) 729,800 (35.4%)
35 minutes or more 295,603 (15.4%) 307,501 (15.9%) 443,240 (21.5%)
Citizenship Status 2005 2013 2019
U.S. citizen by birth 4,297,870 (96.7%) 4,637,681 (95.9%) 4,686,864 (95.6%)
U.S. citizen born abroad to American parents 23,915 (0.5%) 33,815 (0.7%) 33,204 (0.7%)
U.S. citizen by naturalization 36,514 (0.8%) 59,782 (1.2%) 76,963 (1.6%)
Not a U.S. citizen 84,259 (1.9%) 102,444 (2.1%) 97,989 (2.0%)
Veteran Status 2005 2013 2019
Veteran 403,950 (12.1%) 355,396 (9.6%) 318,254 (8.4%)
Non-Veteran 2,940,771 (87.9%) 3,357,045 (90.4%) 3,482,441 (91.6%)
Voter Registration 2004 2014 2020
Active registration 2,617,418 2,881,612 3,512,630
Inactive registration 236,790 108,921 71,625
Data sourced from the U.S. Census Bureau 2019, USDHHS, HRSA, and the AL Secretary of State Voter Registration Statistics.

2020 ALABAMA STATE HEALTH ASSESSMENT
82
Health Indicator 1 - Mental Health and Substance Abuse by County
County
Suicide Mortality Rate
per 100,000 Persons,
2019
Depression Among
Medicaid Recipients,
2018
Substance Abuse
Among Medicaid
Recipients, 2018
Schizophrenia Among
Medicare Recipients,
2018
Rank Rate Count % Count % Count %
Autauga 42 14.3 328 2.6 134 1.1 830 2.5
Baldwin 27 17.5 1,842 4.6 535 1.3 4,241 1.9
Barbour 33 16.2 246 2.5 114 1.1 567 4.3
Bibb 46 13.4 209 3.3 87 1.4 456 3.8
Blount 7 27.7 363 2.7 181 1.3 1,097 2.3
Bullock 56 9.9 69 1.7 25 0.6 85 4.6
Butler 54 10.3 164 2.2 41 0.5 497 3.7
Calhoun 31 16.7 1,152 3.4 803 2.4 3,546 2.7
Chambers 18 21.1 383 3.5 118 1.1 869 3.6
Cherokee 5 30.5 264 3.7 136 1.9 931 2.6
Chilton 36 15.8 459 3.5 232 1.8 728 2.7
Choctaw 66 0.0 161 3.7 45 1.0 438 3.0
Clarke 1 38.1 217 2.6 73 0.9 417 3.1
Clay 6 30.2 155 3.8 33 0.8 413 3.1
Cleburne 3 33.5 153 3.8 61 1.5 375 2.1
Coee 60 7.6 436 3.4 141 1.1 1,514 2.8
Colbert 11 23.5 520 3.6 283 2.0 2,147 2.5
Conecuh 32 16.6 111 2.3 68 1.4 331 3.5
Coosa 58 9.4 98 3.7 28 1.0 217 2.6
Covington 53 10.8 507 4.2 156 1.3 1,405 4.5
Crenshaw 61 7.3 165 3.2 40 0.8 304 4.0
Cullman 20 20.3 742 3.7 286 1.4 2,350 2.3
Dale 26 18.3 651 4.6 234 1.7 1,525 3.2
Dallas 34 16.1 632 3.4 164 0.9 735 5.6
DeKalb 2 35.0 712 3.1 270 1.2 1,984 3.7
Elmore 19 20.9 378 2.1 150 0.9 1,319 2.8
Escambia 21 19.1 291 2.4 157 1.3 767 2.4
Etowah 15 21.5 1,180 3.9 720 2.4 3,404 4.3
Fayette 4 30.7 164 3.0 102 1.9 691 4.0
Franklin 35 15.9 370 3.6 223 2.2 1,147 2.9
Geneva 13 22.8 357 4.1 134 1.5 961 3.2
Greene 9 24.7 100 2.5 64 1.6 248 4.1
Hale 43 13.7 183 2.7 59 0.9 469 3.7
Henry 28 17.4 164 3.4 66 1.4 499 2.9
Data sourced from the ADPH Center for Health Statistics,
the AL Medicaid Agency, and the Center for Medicare and Medicaid Services.

2020 ALABAMA STATE HEALTH ASSESSMENT
83
Health Indicator 1 - Mental Health and Substance Abuse by County
County
Suicide Mortality Rate
per 100,000 Persons,
2019
Depression Among
Medicaid Recipients,
2018
Substance Abuse
Among Medicaid
Recipients, 2018
Schizophrenia Among
Medicare Recipients,
2018
Rank Rate Count % Count % Count %
Houston 22 18.9 1,343 4.2 472 1.5 3,071 3.4
Jackson 44 13.6 360 2.8 158 1.2 1,583 2.5
Jeerson 37 15.5 4,086 2.5 2,366 1.5 9,782 4.1
Lamar 41 14.5 170 3.9 92 2.1 500 2.6
Lauderdale 47 12.9 820 4.0 380 1.9 2,854 2.6
Lawrence 16 21.3 316 3.5 171 1.9 1,062 2.4
Lee 40 14.6 855 2.9 231 0.8 2,147 2.8
Limestone 63 7.1 528 2.9 279 1.5 2,086 2.1
Lowndes 54 10.3 109 2.3 32 0.7 137 4.6
Macon 64 5.5 163 2.5 63 0.9 227 4.2
Madison 24 18.5 1,688 2.7 898 1.4 7,401 2.1
Marengo 17 21.2 277 3.7 215 2.8 558 4.7
Marion 45 13.5 236 2.8 219 2.6 991 2.3
Marshall 51 11.4 821 2.8 467 1.6 2,794 3.1
Mobile 37 15.5 5,423 4.6 1,565 1.3 4,971 3.9
Monroe 66 0.0 190 2.8 83 1.2 356 3.6
Montgomery 50 11.5 1,557 2.2 649 0.9 2,575 3.0
Morgan 12 23.4 930 3.2 486 1.7 3,550 2.9
Perry 52 11.2 142 3.1 38 0.8 263 5.7
Pickens 65 5.0 186 3.0 77 1.2 586 3.1
Pike 39 15.1 382 4.1 98 1.0 546 4.8
Randolph 14 22.0 254 3.6 59 0.8 650 3.3
Russell 29 17.3 519 2.8 123 0.7 1,222 3.3
Shelby 8 25.7 813 2.9 414 1.5 3,288 2.6
St. Clair 61 7.3 565 3.0 377 2.0 1,662 2.4
Sumter 59 8.0 112 2.1 75 1.4 286 3.9
Talladega 23 18.8 1,003 4.0 305 1.2 1,779 2.8
Tallapoosa 49 12.4 419 3.3 158 1.3 1,006 2.3
Tuscaloosa 47 12.9 1,477 3.2 655 1.4 3,853 4.5
Walker 10 23.6 706 3.7 536 2.8 1,936 3.7
Washington 25 18.4 182 4.0 46 1.0 336 2.0
Wilcox 57 9.6 179 3.1 37 0.6 261 4.0
Winston 30 16.9 204 3.0 168 2.5 758 2.2
Data sourced from the ADPH Center for Health Statistics
the AL Medicaid Agency, and the Center for Medicare and Medicaid Services.

2020 ALABAMA STATE HEALTH ASSESSMENT
84
Health Indicator 2 - Access to Care by County
Adults Who Receive an
Annual Checkup, 2018
HPSA and Scores, 2019
County % Designation
Number of Full-time
Employees (FTEs)
Needed to Reach Optimal
HPSA
Score
Autauga 78.4 Low Income Population HPSA 21.87 12
Baldwin 78.6 Low Income Population HPSA 6.35 15
Barbour 80.3 High Needs Geographic HPSA 6.08 20
Bibb 77.5 Geographic HPSA 2.75 16
Blount 76.6 Geographic HPSA 7.21 15
Bullock 81.0 High Needs Geographic HPSA 2.38 21
Butler 80.6 High Needs Geographic HPSA 1.31 15
Calhoun 78.8 Low Income Population HPSA 4.24 13
Chambers 80.6 Geographic HPSA 0.82 3
Cherokee 78.5 Geographic HPSA 2.75 15
Chilton 76.5 High Needs Geographic HPSA 3.83 13
Choctaw 81.5 High Needs Geographic HPSA 3.45 20
Clarke 81.2 High Needs Geographic HPSA 3.15 18
Clay 78.6 Geographic HPSA 0.16 12
Cleburne 76.7 Geographic HPSA 3.24 18
Coee 78.4 Not Designated - -
Colbert 78.4 Low Income Population HPSA 7.27 14
Conecuh 81.5 High Needs Geographic HPSA 0.01 15
Coosa 80.4 Geographic HPSA 1.13 14
Covington 78.1 Low Income Population HPSA 2.36 16
Crenshaw 78.6 Geographic HPSA 2.42 15
Cullman 76.5 Low Income Population HPSA 5.45 13
Dale 78.6 High Needs Geographic HPSA 7.66 15
Dallas 82.4 High Needs Geographic HPSA 1.53 15
DeKalb 76.0 High Needs Geographic HPSA 7.14 14
Elmore 78.0 High Needs Geographic HPSA 5.45 18
Escambia 78.5 High Needs Geographic HPSA 0.19 11
Etowah 77.9 Low Income Population HPSA 6.93 15
Fayette 78.2 High Needs Geographic HPSA 6.00 15
Franklin 76.2 High Needs Geographic HPSA 0.40 10
Geneva 78.2 High Needs Geographic HPSA 0.40 14
Greene 84.4 High Needs Geographic HPSA 2.32 23
Hale 82.1 High Needs Geographic HPSA 2.03 20
Henry 80.2 High Needs Geographic HPSA 3.59 11
Data sourced from the CDC BRFSS and ADPH Oce of Primary Care and Rural Health.

2020 ALABAMA STATE HEALTH ASSESSMENT
85
Health Indicator 2 - Access to Care by County
Adults Who Receive an
Annual Checkup, 2018
HPSA and Scores, 2019
County % Designation
Number of FTEs Needed
to Reach Optimal
HPSA
Score
Houston 79.2 Not Designated - -
Jackson 77.6 Low Income Population HPSA 1.06 9
Jeerson 80.3 Low Income Population HPSA 20.49 15
Lamar 78.5 High Needs Geographic HPSA 6.00 15
Lauderdale 78.7 Low Income Population HPSA 7.27 14
Lawrence 78.2 Geographic HPSA 4.83 15
Lee 77.6 Low Income Population HPSA 10.45 16
Limestone 77.3 Geographic HPSA 9.64 15
Lowndes 83.1 High Needs Geographic HPSA 2.61 22
Macon 83.9 High Needs Geographic HPSA 5.45 18
Madison 78.9 Not Designated - -
Marengo 81.3 High Needs Geographic HPSA 1.97 17
Marion 77.8 Low Income Population HPSA 2.41 15
Marshall 76.2 High Needs Geographic HPSA 0.31 10
Mobile 79.4 Low Income Population HPSA 21.70 13
Monroe 81.3 High Needs Geographic HPSA 2.64 18
Montgomery 81.1 Low Income Population HPSA 21.87 16
Morgan 77.4 Low Income Population HPSA 6.81 11
Perry 81.9 High Needs Geographic HPSA 1.15 19
Pickens 80.1 High Needs Geographic HPSA 0.12 13
Pike 78.0 Low Income Population HPSA 0.25 11
Randolph 79.2 High Needs Geographic HPSA 4.38 17
Russell 79.0 High Needs Geographic HPSA 14.47 19
Shelby 77.6 Not Designated - -
St. Clair 77.3 High Needs Geographic HPSA 11.00 9
Sumter 82.1 High Needs Geographic HPSA 2.27 18
Talladega 79.4 High Needs Geographic HPSA 5.93 13
Tallapoosa 79.6 Low Income Population HPSA 2.40 20
Tuscaloosa 77.8 Low Income Population HPSA 14.79 15
Walker 77.9 Low Income Population HPSA 3.10 16
Washington 79.2 Geographic HPSA 2.83 14
Wilcox 82.9 High Needs Geographic HPSA 0.83 18
Winston 77.9 High Needs Geographic HPSA 2.99 15
Data sourced from the CDC BRFSS and ADPH Oce of Primary Care and Rural Health.

2020 ALABAMA STATE HEALTH ASSESSMENT
86
Health Indicator 3 –Pregnancy Outcomes by County
County
Infant Mortality Rate Per 1,000 Persons,
2019
Teen Pregnancy Rate Per 1,000 Persons,
2019
Rank Rate Rank Rate
Autauga 55 4.5 65 8.2
Baldwin 46 5.2 61 10.2
Barbour 16 10.8 29 15.7
Bibb 6 20.3 45 12.7
Blount 60 1.6 53 12.0
Bullock 61 0.0 3 25.0
Butler 55 4.5 5 21.4
Calhoun 39 6.5 21 17.0
Chambers 45 5.3 26 16.1
Cherokee 29 8.2 40 13.5
Chilton 49 5.1 15 18.7
Choctaw 61 0.0 18 17.8
Clarke 61 0.0 13 18.9
Clay 37 6.7 30 15.6
Cleburne 12 12.9 39 13.9
Coee 55 4.5 43 13.2
Colbert 52 4.8 33 14.9
Conecuh 4 21.1 11 19.2
Coosa 1 26.3 34 14.4
Covington 52 4.8 27 16.0
Crenshaw 61 0.0 23 16.6
Cullman 46 5.2 36 14.2
Dale 26 9.0 6 21.2
Dallas 39 6.5 16 17.9
DeKalb 21 10.0 38 14.1
Elmore 14 11.6 57 10.6
Escambia 37 6.7 18 17.8
Etowah 43 5.7 11 19.2
Fayette 19 10.2 7 20.8
Franklin 54 4.7 8 20.2
Geneva 9 14.8 22 16.7
Greene 2 23.3 2 25.8
Hale 5 20.7 48 12.5
Henry 7 16.8 50 12.2
Data sourced from the ADPH Center for Health Statistics.

2020 ALABAMA STATE HEALTH ASSESSMENT
87
Health Indicator 3 –Pregnancy Outcomes by County
County
Infant Mortality Rate Per 1,000 Persons,
2019
Teen Pregnancy Rate Per 1,000 Persons,
2019
Rank Rate Rank Rate
Houston 32 7.5 32 15.4
Jackson 25 9.2 40 13.5
Jeerson 21 10.0 56 10.9
Lamar 29 8.2 47 12.6
Lauderdale 46 5.2 51 12.1
Lawrence 61 0.0 23 16.6
Lee 58 4.2 64 8.5
Limestone 34 7.1 59 10.5
Lowndes 10 13.9 59 10.5
Macon 12 12.9 51 12.1
Madison 35 7.0 63 8.9
Marengo 3 21.8 62 10.1
Marion 42 5.8 16 17.9
Marshall 44 5.6 9 19.3
Mobile 36 6.9 35 14.3
Monroe 28 8.5 4 22.6
Montgomery 20 10.1 18 17.8
Morgan 41 6.3 25 16.2
Perry 24 9.4 14 18.8
Pickens 17 10.7 36 14.2
Pike 18 10.4 45 12.7
Randolph 8 16.4 42 13.4
Russell 23 9.7 28 15.8
Shelby 51 4.9 57 10.6
St. Clair 59 4.1 67 4.8
Sumter 32 7.5 55 11.6
Talladega 31 8.1 53 12.0
Tallapoosa 50 5.0 66 7.2
Tuscaloosa 15 11.0 47 12.6
Walker 27 8.8 9 19.3
Washington 61 0.0 44 12.9
Wilcox 61 0.0 1 32.1
Winston 11 13.6 31 15.5
Data sourced from the ADPH Center for Health Statistics.

2020 ALABAMA STATE HEALTH ASSESSMENT
88
Health Indicator 4 – Nutrition and Physical Activity by County
County
Prevalence of Obesity, 2018 Prevalence of No Physical Activity, 2018
Rank % Rank %
Autauga 50 35.8 62 27.2
Baldwin 67 29.7 66 24.9
Barbour 19 40.7 10 38.1
Bibb 26 38.7 45 32.1
Blount 60 34.0 47 31.4
Bullock 2 45.8 5 39.2
Butler 16 41.2 12 37.3
Calhoun 18 40.9 54 30.3
Chambers 23 39.1 27 34.2
Cherokee 23 39.1 36 33.2
Chilton 21 40.4 28 34.1
Choctaw 12 42.9 14 36.5
Clarke 20 40.5 11 37.5
Clay 49 35.9 26 34.4
Cleburne 35 37.1 45 32.1
Coee 45 36.0 52 30.8
Colbert 29 38.0 49 31.2
Conecuh 10 43.2 4 40.8
Coosa 17 41.0 15 35.6
Covington 32 37.6 30 33.4
Crenshaw 39 36.6 33 33.3
Cullman 62 33.4 42 32.3
Dale 9 43.4 50 31.0
Dallas 13 42.2 3 41.0
DeKalb 51 35.4 24 34.6
Elmore 51 35.4 61 28.1
Escambia 31 37.7 21 35.1
Etowah 36 37.0 42 32.3
Fayette 57 34.8 25 34.5
Franklin 45 36.0 29 33.7
Geneva 11 43.0 13 36.9
Greene 4 45.6 1 41.4
Hale 4 45.6 9 38.3
Henry 45 36.0 40 32.8
Data sourced from BRFSS.

2020 ALABAMA STATE HEALTH ASSESSMENT
89
Health Indicator 4 – Nutrition and Physical Activity by County
County
Prevalence of Obesity, 2018 Prevalence of No Physical Activity, 2018
Rank % Rank %
Houston 55 34.9 38 33.1
Jackson 37 36.9 20 35.2
Jeerson 58 34.5 60 28.2
Lamar 42 36.3 36 33.2
Lauderdale 59 34.4 57 28.6
Lawrence 45 36.0 47 31.4
Lee 66 32.1 65 25.0
Limestone 62 33.4 58 28.5
Lowndes 2 45.8 8 38.8
Macon 1 46.0 15 35.6
Madison 64 33.1 63 26.2
Marengo 7 44.6 19 35.3
Marion 53 35.0 30 33.4
Marshall 25 38.9 42 32.3
Mobile 37 36.9 56 29.9
Monroe 14 42.1 7 38.9
Montgomery 39 36.6 54 30.3
Morgan 34 37.4 58 28.5
Perry 8 44.1 2 41.2
Pickens 15 41.9 17 35.5
Pike 32 37.6 53 30.4
Randolph 43 36.1 33 33.3
Russell 28 38.3 33 33.3
Shelby 65 32.7 67 23.5
St. Clair 29 38.0 51 30.9
Sumter 21 40.4 22 34.8
Talladega 26 38.7 17 35.5
Tallapoosa 53 35.0 39 32.9
Tuscaloosa 60 34.0 64 25.4
Walker 39 36.6 41 32.5
Washington 55 34.9 22 34.8
Wilcox 6 45.3 6 39.1
Winston 43 36.1 30 33.4
Data sourced from BRFSS.

2020 ALABAMA STATE HEALTH ASSESSMENT
90
Health Indicator 5 - Social Determinants of Health by County
County
Individuals Below Poverty Line by Education Level, 2019
Total Below
Poverty
< 12 Grade
High School
Graduate/GED
AAS/Some
College
BS or higher
Autauga 4,436 1,439 1,919 694 384
Baldwin 13,382 3,198 4,910 3,564 1,710
Barbour 3,275 1,369 1,352 475 79
Bibb 1,734 502 1,013 96 123
Blount 4,715 1,851 1,578 1,128 158
Bullock 1,552 528 724 298 2
Butler 2,594 670 1,285 489 150
Calhoun 11,587 3,575 4,132 3,224 656
Chambers 3,376 1,284 1,287 694 111
Cherokee 2,568 1,153 801 488 126
Chilton 4,920 1,639 2,135 889 257
Choctaw 1,684 641 569 394 80
Clarke 3,708 1,123 1,816 598 171
Clay 1,442 755 433 223 21
Cleburne 1,493 453 584 326 130
Coee 3,881 1,180 1,237 1,199 265
Colbert 5,234 1,376 2,084 1,480 294
Conecuh 1,587 518 753 216 100
Coosa 930 329 367 206 28
Covington 4,003 1,235 1,387 1,189 192
Crenshaw 1,329 512 537 234 46
Cullman 7,928 2,481 2,841 1,983 623
Dale 4,939 1,420 1,849 1,354 316
Dallas 6,366 1,909 2,594 1,680 183
DeKalb 8,695 4,161 2,512 1,613 409
Elmore 5,199 1,608 2,219 861 511
Escambia 4,734 1,237 222 1,105 170
Etowah 9,153 3,211 2,952 2,511 479
Fayette 1,897 611 711 546 29
Franklin 3,040 1,194 1,096 530 220
Geneva 3,437 1,313 1,332 674 118
Greene 1,764 541 910 285 28
Hale 2,164 726 1,143 278 17
Henry 1,442 489 538 360 55
Data sourced from the U.S. Census Bureau and County Health Statistics.

2020 ALABAMA STATE HEALTH ASSESSMENT
91
Health Indicator 5 - Social Determinants of Health by County
County
Individuals Below Poverty Line by Education Level, 2019
Total Below
Poverty
< 12 Grade
High School
Graduate/GED
AAS/Some
College
BS or higher
Houston 10,116 2,876 3,851 2,701 688
Jackson 6,489 2,003 2,732 1,461 293
Jeerson 60,121 13,345 21,661 18,348 6,767
Lamar 1,623 535 647 413 28
Lauderdale 7,481 2,507 2,474 1,892 608
Lawrence 3,244 1,233 1,424 501 86
Lee 12,125 2,541 3,818 3,723 2,043
Limestone 6,939 2,579 2,343 1,370 647
Lowndes 1,605 597 779 181 48
Macon 2,489 745 697 767 280
Madison 24,029 6,507 7,434 6,979 3,109
Marengo 2,649 623 1,455 515 56
Marion 3,030 1,069 1,081 654 226
Marshall 10,241 3,879 3,234 2,478 650
Mobile 40,670 10,845 15,557 11,282 2,986
Monroe 4,057 843 2,404 685 125
Montgomery 22,588 7,323 7,750 5,429 2,086
Morgan 10,104 4,047 3,123 2,421 513
Perry 1,874 552 908 343 71
Pickens 2,434 939 811 557 127
Pike 3,033 1,158 812 674 389
Randolph 2,316 777 951 400 188
Russell 6,246 1,888 2,486 1,445 427
St. Clair 7,139 2,871 2,445 1,468 355
Shelby 9,916 2,523 2,602 2,933 1,858
Sumter 2,030 512 905 413 200
Talladega 8,650 3,244 2,902 2,232 272
Tallapoosa 4,343 1,579 1,352 1,174 238
Tuscaloosa 15,014 3,631 5,815 3,699 1,869
Walker 7,331 2,625 2,845 1,745 116
Washington 2,016 690 839 375 112
Wilcox 1,794 655 634 438 67
Winston 2,307 879 772 613 43
Data sourced from the U.S. Census Bureau and County Health Statistics.

2020 ALABAMA STATE HEALTH ASSESSMENT
92
Health Indicator 6 – Sexually Transmitted Infections by County
County
Syphilis Case Rate Per
100,000 Persons, 2019
Gonorrhea Case Rate Per
100,000 Persons, 2019
Chlamydia Case Rate Per
100,000 Persons, 2019
Rank Rate Rank Rate Rank Rate
Autauga 38 14.3 39 234.5 33 581.7
Baldwin 50 8.1 61 104.4 55 336.4
Barbour 7 48.6 3 563.1 10 899.3
Bibb 48 8.9 33 259.0 39 540.3
Blount 60 3.5 53 148.7 46 408.1
Bullock 28 19.8 6 504.9 19 742.5
Butler 56 5.1 17 344.5 6 1,064.4
Calhoun 32 16.7 19 329.2 21 732.4
Chambers 6 51.1 18 339.8 22 721.7
Cherokee 58 3.8 51 156.5 61 282.5
Chilton 52 6.8 58 126.0 54 339.9
Choctaw 10 47.7 37 238.3 40 492.5
Clarke 39 12.7 31 270.9 17 778.9
Clay 67 0.0 30 272.0 34 574.2
Cleburne 53 6.7 60 107.3 65 234.7
Coee 43 11.5 32 263.7 27 634.3
Colbert 4 68.8 22 316.8 32 584.7
Conecuh 34 16.6 34 256.9 30 596.7
Coosa 67 0.0 7 478.3 11 844.0
Covington 62 2.7 44 205.1 45 429.2
Crenshaw 67 0.0 29 275.9 14 798.7
Cullman 42 11.9 64 89.5 66 231.6
Dale 15 38.6 15 357.9 35 569.4
Dallas 24 24.2 14 365.6 9 932.9
DeKalb 61 2.8 66 75.5 58 300.6
Elmore 23 25.9 27 279.5 36 560.3
Escambia 62 2.7 40 226.6 24 696.1
Etowah 45 10.8 26 280.6 28 613.1
Fayette 55 6.1 41 220.8 44 429.4
Franklin 19 31.9 55 143.5 50 389.0
Geneva 58 3.8 42 217.0 47 407.3
Greene 16 37.0 8 468.5 4 1,171.2
Hale 17 34.1 1 668.9 3 1,194.5
Henry 31 17.4 25 284.8 31 587.0
Data sourced from the ADPH Division of STD Prevention and Control.

2020 ALABAMA STATE HEALTH ASSESSMENT
93
Health Indicator 6 – Sexually Transmitted Infections by County
County
Syphilis Case Rate Per
100,000 Persons, 2019
Gonorrhea Case Rate Per
100,000 Persons, 2019
Chlamydia Case Rate Per
100,000 Persons, 2019
Rank Rate Rank Rate Rank Rate
Houston 11 42.5 16 352.3 25 692.3
Jackson 51 7.75 65 85.2 64 255.7
Jeerson 14 39.0 12 368.7 23 707.4
Lamar 37 14.5 62 94.2 51 354.9
Lauderdale 5 58.6 38 237.6 42 460.0
Lawrence 18 33.4 49 173.1 57 303.7
Lee 20 31.0 48 175.6 43 446.1
Limestone 36 15.2 46 195.1 52 342.7
Lowndes 13 41.1 20 329.0 8 945.9
Macon 2 83.0 5 531.3 2 1,228.7
Madison 22 28.4 10 398.2 18 766.1
Marengo 35 15.9 24 302.2 15 795.2
Marion 46 10.1 52 151.5 59 296.2
Marshall 44 11.4 56 131.2 53 340.0
Mobile 8 48.4 13 365.7 13 812.9
Monroe 67 0.0 36 246.0 37 554.7
Montgomery 1 86.5 4 543.1 5 1,140.5
Morgan 32 16.7 43 208.1 49 396.9
Perry 25 22.4 21 325.0 12 829.3
Pickens 3 70.2 47 190.7 29 602.1
Pike 21 30.2 9 419.8 7 954.3
Randolph 26 22.0 45 202.4 38 554.5
Russell 12 41.4 23 312.3 16 788.5
Shelby 30 17.9 63 89.6 62 275.6
St. Clair 41 12.3 59 125.1 56 336.3
Sumter 57 4.8 67 42.6 67 108.6
Talladega 27 21.3 11 376.4 26 690.2
Tallapoosa 40 12.4 54 148.6 48 406.3
Tuscaloosa 9 48.2 28 277.5 20 736.5
Walker 54 6.3 57 129.1 60 284.9
Washington 29 18.4 35 251.1 41 471.6
Wilcox 47 9.6 2 636.3 1 1,349.7
Winston 49 8.5 50 169.3 63 275.1
Data sourced from the ADPH Division of STD Prevention and Control.
2020 ALABAMA STATE HEALTH ASSESSMENT
94
Health Indicator 7 - Geriatrics by County
County
Alzheimer’s Disease Among
Medicare Recipients, 2018
County
Alzheimer’s Disease Among
Medicare Recipients, 2018
Count % Count %
Autauga 536 10.6 Houston 1713 12.1
Baldwin 2885 11.1 Jackson 901 10.3
Barbour 401 11.8 Jeerson 6291 12.5
Bibb 261 12.6 Lamar 303 9.9
Blount 585 11.1 Lauderdale 1822 12.3
Bullock 122 12.7 Lawrence 505 9.9
Butler 438 12.5 Lee 1372 10.1
Calhoun 2075 11.6 Limestone 1021 9.3
Chambers 673 11.4 Lowndes 133 12.6
Cherokee 427 9.8 Macon 257 12.4
Chilton 372 10.5 Madison 4350 10.7
Choctaw 365 12.3 Marengo 433 10.9
Clarke 429 13.1 Marion 602 11.3
Clay 272 12.3 Marshall 1621 11.8
Cleburne 282 11.1 Mobile 3887 12.3
Coee 910 12.3 Monroe 389 10.8
Colbert 1107 11.4 Montgomery 2149 11.3
Conecuh 245 9.7 Morgan 1932 11.2
Coosa 146 9.5 Perry 250 13.6
Covington 961 13.0 Pickens 386 10.5
Crenshaw 222 10.9 Pike 404 11.8
Cullman 1232 10.9 Randolph 413 10.4
Dale 830 11.5 Russell 730 10.9
Dallas 666 12.7 Shelby 1842 11.4
DeKalb 1063 10.6 St. Clair 817 11.0
Elmore 891 10.6 Sumter 244 10.5
Escambia 640 12.6 Talladega 1040 10.9
Etowah 1594 11.4 Tallapoosa 768 11.4
Fayette 450 13.5 Tuscaloosa 2221 11.8
Franklin 622 12.2 Walker 931 11.5
Geneva 533 11.5 Washington 253 9.2
Greene 177 10.6 Wilcox 217 9.2
Hale 311 11.0 Winston 427 10.8
Henry 276 10.4
Data sourced from the Center for Medicare and Medicaid Services.

2020 ALABAMA STATE HEALTH ASSESSMENT
95
Health Indicator 8 - Cardiovascular Diseases by County
County
Heart Disease- related
Mortality Rate Per
100,000 Persons, 2019
Stroke-related
Mortality Rate Per
100,000 Persons, 2019
Hypertension Among
Medicaid Recipients,
2018
BCBS Cardiovascular
Diseases-related
Claims, 2019
Rank Rate Rank Rate Count % Count %
Autauga 60 234.5 48 55.8 685 5.5 7,054 27.2
Baldwin 55 248.6 33 65.6 1,426 3.6 23,334 23.2
Barbour 6 441.5 23 72.3 902 9.0 2,639 34.4
Bibb 29 330.4 25 71.4 594 9.3 3,051 32.4
Blount 45 287.1 65 32.8 614 4.6 6,774 26.0
Bullock 54 257.4 10 88.8 379 9.4 1,115 44.1
Butler 58 236.5 16 81.3 798 10.7 2,968 33.8
Calhoun 23 345.9 8 91.0 2,755 8.1 11,983 23.9
Chambers 48 279.7 55 47.6 1,016 9.2 3,360 33.0
Cherokee 25 339.7 45 57.6 498 6.9 2,072 26.0
Chilton 44 290.4 28 67.9 637 4.9 5,137 27.0
Choctaw 8 421.0 39 62.3 689 15.7 1,353 34.3
Clarke 37 304.8 26 71.1 782 9.3 3,366 31.8
Clay 16 392.9 29 67.8 312 7.7 2,032 29.6
Cleburne 3 449.4 17 80.1 341 8.5 1,238 24.0
Coee 32 324.8 62 36.6 1,140 8.8 5,213 26.4
Colbert 14 405.5 43 58.4 1,532 10.6 5,881 27.1
Conecuh 4 447.5 22 73.3 596 12.3 1,808 40.0
Coosa 20 356.4 7 93.3 226 8.4 1,258 33.1
Covington 10 413.0 6 97.3 1,339 11.2 4,675 31.1
Crenshaw 33 319.5 12 86.8 411 8.0 2,048 29.5
Cullman 21 355.7 37 63.5 1,478 7.3 9,894 23.7
Dale 53 262.3 58 44.9 1,321 9.4 4,762 28.8
Dallas 15 400.6 13 83.5 2,192 11.7 4,374 36.7
DeKalb 43 292.3 40 60.2 1,510 6.6 6,554 24.6
Elmore 52 263.5 46 57.4 882 5.0 12,516 29.3
Escambia 40 303.0 14 81.6 782 6.4 3,466 26.0
Etowah 28 331.5 41 59.5 2,800 9.3 10,967 26.2
Fayette 34 312.8 3 103.5 583 10.7 2,461 29.9
Franklin 31 325.2 54 47.8 807 7.9 2,956 25.6
Geneva 38 304.5 52 53.2 816 9.4 2,686 26.8
Greene 35 308.2 63 36.4 550 13.5 1,132 43.3
Hale 5 443.7 15 81.5 800 11.8 2,641 36.7
Henry 36 308.0 56 46.5 416 8.5 2,029 27.7
Data sourced from the ADPH Center for Health Statistics, the AL Medicaid Agency, and the BCBS Member Claims.

2020 ALABAMA STATE HEALTH ASSESSMENT
96
Health Indicator 8 - Cardiovascular Diseases by County
County
Heart Disease- related
Mortality Rate Per
100,000 Persons, 2019
Stroke-related
Mortality Rate Per
100,000 Persons, 2019
Hypertension Among
Medicaid Recipients,
2018
BCBS Cardiovascular
Diseases-related
Claims, 2019
Rank Rate Rank Rate Count % Count %
Houston 50 272.9 61 38.2 2,472 7.8 11,021 26.2
Jackson 17 391.3 11 87.0 1,112 8.8 5,234 27.3
Jeerson 59 235.2 18 75.5 8,666 5.4 73,036 24.1
Lamar 22 347.7 64 36.1 381 8.7 1,184 26.0
Lauderdale 51 267.4 21 73.6 1,685 8.3 8,528 24.1
Lawrence 39 303.7 44 57.7 829 9.2 3,653 28.0
Lee 66 149.5 60 41.5 1,809 6.2 13,723 23.1
Limestone 56 246.7 47 57.2 1,145 6.3 8,767 21.1
Lowndes 18 390.7 2 130.3 455 9.5 1,651 37.8
Macon 12 409.6 5 97.6 533 8.0 2,531 38.9
Madison 61 233.0 49 54.8 3,453 5.5 34,616 20.2
Marengo 30 328.7 27 68.2 1,173 15.5 2,615 32.9
Marion 11 410.6 32 67.2 822 9.8 2,909 25.9
Marshall 47 281.1 33 65.6 1,904 6.5 9,496 23.4
Mobile 41 296.9 36 63.6 6,403 5.4 43,478 27.4
Monroe 46 284.6 9 90.2 748 11.0 2,543 30.0
Montgomery 64 200.9 29 67.8 3,855 5.4 30,710 31.9
Morgan 27 331.7 51 53.7 1,745 6.1 11,502 22.8
Perry 63 212.9 65 32.8 721 15.7 1,206 42.3
Pickens 13 406.4 19 75.2 959 15.3 2,654 34.6
Pike 57 244.6 53 51.0 897 9.5 3,763 30.9
Randolph 7 431.3 59 44.0 696 9.9 1,831 28.5
Russell 65 176.0 42 58.8 1,147 6.3 2,442 25.9
Shelby 9 413.4 1 142.1 982 3.5 26,902 22.1
St. Clair 67 95.5 67 17.2 1,049 5.6 11,613 26.7
Sumter 49 273.6 38 63.0 885 16.9 1,489 40.0
Talladega 26 337.6 31 67.6 2,020 8.1 8,945 26.5
Tallapoosa 19 384.0 35 64.2 963 7.7 5,724 31.3
Tuscaloosa 62 216.4 50 54.6 3,387 7.4 28,718 29.3
Walker 1 517.9 20 73.8 1,475 7.6 8,514 30.8
Washington 42 294.0 23 73.3 487 10.7 2,199 29.7
Wilcox 2 501.3 3 103.5 837 14.5 1,467 38.6
Winston 24 342.8 56 46.5 804 11.9 3,001 27.2
Data sourced from the ADPH Center for Health Statistics, the AL Medicaid Agency, and the BCBS Member Claims.

2020 ALABAMA STATE HEALTH ASSESSMENT
97
Health Indicator 9 – Child Abuse and Neglect by County
County
Total Children Under 18 by County,
2019
County
Total Children Under 18 by County,
2019
Count % Count %
Autauga 12,962 23.2 Houston 24,247 22.9
Baldwin 47,549 21.3 Jackson 10,687 20.7
Barbour 5,085 20.6 Jeerson 150,155 22.8
Bibb 4,546 20.3 Lamar 2,954 21.4
Blount 13,242 22.9 Lauderdale 18,082 19.5
Bullock 2,101 20.8 Lawrence 7,079 21.5
Butler 4,279 22.0 Lee 34,718 21.1
Calhoun 24,425 21.5 Limestone 22,058 22.3
Chambers 6,917 20.8 Lowndes 2,140 22.0
Cherokee 4,951 18.9 Macon 3,090 17.1
Chilton 10,574 23.8 Madison 80,548 21.6
Choctaw 2,480 19.7 Marengo 4,244 22.5
Clarke 5,031 21.3 Marion 6,179 20.8
Clay 2,673 20.2 Marshall 24,290 25.1
Cleburne 3,355 22.5 Mobile 96,278 23.3
Coee 12,405 23.7 Monroe 4,375 21.1
Colbert 11,545 20.9 Montgomery 52,998 23.4
Conecuh 2,474 20.5 Morgan 27,287 22.8
Coosa 1,749 16.4 Perry 1,865 20.9
Covington 8,151 22.0 Pickens 3,866 19.4
Crenshaw 3,140 22.8 Pike 6,292 19.0
Cullman 18,848 22.5 Randolph 4,794 21.1
Dale 11,211 22.8 Russell 13,969 24.1
Dallas 8,667 23.3 Shelby 20,767 23.2
DeKalb 1,7092 23.9 St. Clair 48,983 22.5
Elmore 18,110 22.3 Sumter 2,361 19.0
Escambia 8,242 22.5 Talladega 16,715 20.9
Etowah 21,783 21.3 Tallapoosa 8,235 20.4
Fayette 3,440 21.1 Tuscaloosa 43,965 21.0
Franklin 7,778 24.8 Walker 14,102 22.2
Geneva 5,780 22.0 Washington 3,608 22.1
Greene 1,768 21.8 Wilcox 2,417 23.3
Hale 3,370 23.0 Winston 4,773 20.2
Henry 3,510 20.4
Data sourced from the U.S. Census Bureau.

2020 ALABAMA STATE HEALTH ASSESSMENT
98
Health Indicator 10 – Environmental Health by County
County
Number of Schools Tested
for Lead in the Water
County
Number of Schools Tested
for Lead in the Water
Autauga 13 Houston 32
Baldwin 47 Jackson 22
Barbour 10 Jeerson 99
Bibb 11 Lamar 8
Blount 19 Lauderdale 22
Bullock 4 Lawrence 14
Butler 0 Lee 27
Calhoun 35 Limestone 21
Chambers 3 Lowndes 5
Cherokee 8 Macon 0
Chilton 14 Madison 68
Choctaw 4 Marengo 7
Clarke 9 Marion 13
Clay 2 Marshall 29
Cleburne 8 Mobile 98
Coee 11 Monroe 7
Colbert 15 Montgomery 55
Conecuh 8 Morgan 44
Coosa 3 Perry 0
Covington 11 Pickens 8
Crenshaw 3 Pike 9
Cullman 36 Randolph 3
Dale 12 Russell 19
Dallas 0 Shelby 38
DeKalb 17 St. Clair 8
Elmore 17 Sumter 5
Escambia 15 Talladega 21
Etowah 39 Tallapoosa 5
Fayette 6 Tuscaloosa 59
Franklin 4 Walker 10
Geneva 9 Washington 8
Greene 3 Wilcox 7
Hale 6 Winston 11
Henry 5
Data sourced from ADEM.

2020 ALABAMA STATE HEALTH ASSESSMENT
99
Health Indicator 11 - Violence by County
Ranking of Number of Violent Crimes by County, 2018-2019
Violence
Mortality Rate
Per 100,000
Persons, 2019
County
Homicides Assaults Robbery Rape
Rank Rate
2018 2019 2018 2019 2018 2019 2018 2019
Autauga 35 12 37 36 14 19 31 22 48 23.3
Baldwin 20 9 10 9 10 8 5 5 51 22.0
Barbour 35 11 36 34 27 28 34 25 7 48.6
Bibb 67 15 59 50 41 29 47 26 32 31.3
Blount 35 14 12 15 38 22 25 18 21 36.3
Bullock 67 67 50 48 34 28 54 33 14 39.6
Butler 67 67 29 40 48 22 51 32 54 20.6
Calhoun 11 11 6 10 6 10 8 11 45 27.3
Chambers 26 15 34 35 20 18 21 21 16 39.1
Cherokee 26 15 39 39 41 31 28 24 25 34.4
Chilton 67 14 24 27 41 34 43 20 58 18.0
Choctaw 67 67 64 60 58 34 54 33 67 7.9
Clarke 35 15 42 41 48 30 29 29 7 46.6
Clay 67 67 42 42 58 34 67 33 38 30.2
Cleburne 67 67 66 57 58 67 54 29 5 67.1
Coee 20 14 26 22 22 17 29 11 53 21.0
Colbert 16 14 25 32 25 23 24 23 29 32.6
Conecuh 35 15 55 48 38 34 45 29 27 33.1
Coosa 67 15 47 45 63 33 54 33 43 28.1
Covington 20 14 33 33 36 30 40 21 47 24.3
Crenshaw 67 15 61 51 52 29 54 28 64 14.5
Cullman 26 14 46 44 30 25 17 22 30 32.2
Dale 35 67 21 24 31 27 26 24 36 30.5
Dallas 17 11 17 29 13 21 21 26 18 37.6
DeKalb 26 14 32 26 52 30 13 15 6 48.9
Elmore 12 13 30 25 19 14 11 7 42 28.3
Escambia 67 13 28 31 34 20 38 23 4 71.0
Etowah 13 12 11 14 12 13 6 10 44 27.4
Fayette 67 15 65 57 63 33 47 30 11 42.9
Franklin 35 14 58 28 52 33 34 25 40 28.7
Geneva 35 15 40 38 52 31 38 32 36 30.5
Greene 35 67 42 49 38 32 54 30 20 37.0
Hale 67 67 67 59 67 34 67 67 55 20.5
Henry 67 15 56 50 58 67 47 29 49 23.2
Data sourced from the AL Law Enforcement Agency UCR and the Center for Health Statistics.

2020 ALABAMA STATE HEALTH ASSESSMENT
100
Health Indicator 11 - Violence by County
Ranking of Number of Violent Crimes by County, 2018-2019
Violence
Mortality Rate
Per 100,000
Persons, 2019
County
Homicides Assaults Robbery Rape
Rank Rate
2018 2019 2018 2019 2018 2019 2018 2019
Houston
5 7 7 6 6 6 15 6 39 29.3
Jackson
67 15 22 18 41 31 44 33 56 19.4
Jeerson
1 1 1 1 1 1 1 1 12 41.0
Lamar
67 67 63 58 63 31 53 32 52 21.7
Lauderdale
13 14 23 20 18 12 19 13 59 17.3
Lawrence
67 67 48 46 41 31 34 24 26 33.4
Lee
6 8 5 5 9 7 9 8 46 24.9
Limestone
6 67 31 56 27 25 27 33 60 17.2
Lowndes
20 14 51 52 27 26 51 31 1 92.5
Macon
20 10 35 30 26 20 40 27 3 72.0
Madison
3 4 3 2 4 2 2 2 41 28.4
Marengo
67 13 38 37 36 24 45 32 19 37.1
Marion
67 15 45 45 31 34 31 26 65 13.5
Marshall
26 15 18 19 20 27 20 17 61 15.5
Mobile
2 2 2 3 2 4 3 3 33 31.0
Monroe
20 15 53 56 63 33 67 33 57 19.3
Montgomery
4 3 4 4 3 3 10 14 30 32.2
Morgan
26 11 19 16 11 10 16 16 23 35.1
Perry
35 15 62 54 48 32 67 32 9 44.8
Pickens
67 67 59 55 48 67 54 30 62 15.1
Pike
13 15 16 17 17 25 40 24 15 39.3
Randolph
67 67 51 47 52 33 54 33 34 30.8
Russell
6 5 27 23 8 9 7 6 10 43.1
Saint Clair
26 13 14 11 33 27 23 19 22 35.7
Shelby
17 12 9 8 16 16 12 9 66 10.6
Sumter
35 14 48 45 41 30 62 32 13 40.2
Talladega
9 10 13 12 15 11 18 12 24 35.0
Tallapoosa
26 67 15 13 24 19 34 19 63 14.9
Tuscaloosa
9 6 8 7 5 5 4 4 50 22.9
Walker
35 14 20 21 23 15 14 14 27 33.1
Washington
35 67 56 53 58 34 62 31 35 30.6
Wilcox
17 67 41 52 41 29 47 32 2 77.1
Winston
26 13 54 43 52 34 31 27 17 38.1
Data sourced from the AL Law Enforcement Agency UCR and the Center for Health Statistics.

2020 ALABAMA STATE HEALTH ASSESSMENT
101
Health Indicator 12 - Cancer by County
County
Overall Cancer Mortality Rate Per 100,000 Persons, 2016-2019
2016
Count
2016 Rate
2017
Count
2017 Rate
2018
Count
2018 Rate
2019
Count
2019 Rate
Autauga 106 191.3 95 171.2 89 160.1 108 193.3
Baldwin 461 221.0 489 230.0 546 250.4 480 215.0
Barbour 59 227.2 74 292.8 67 269.3 60 243.1
Bibb 55 242.9 48 211.8 58 258.9 50 223.3
Blount 155 268.6 140 241.3 137 236.9 153 264.6
Bullock 37 357.1 26 252.2 19 187.4 23 227.7
Butler 48 240.0 44 221.9 53 269.3 43 221.1
Calhoun 271 236.5 263 229.2 302 264.3 253 222.7
Chambers 94 277.8 91 269.9 90 267.7 75 225.5
Cherokee 79 307.1 70 270.7 67 257.4 67 255.8
Chilton 87 198.0 97 220.1 79 178.9 99 222.8
Choctaw 24 184.7 31 239.5 27 210.3 38 301.9
Clarke 54 221.4 49 203.5 73 305.2 80 338.7
Clay 36 266.8 31 231.9 40 301.3 37 279.6
Cleburne 36 241.2 28 187.9 29 193.5 35 234.7
Coee 94 183.5 109 210.1 120 231.2 98 187.2
Colbert 140 258.2 132 242.2 154 281.2 151 273.3
Conecuh 33 266.2 39 312.8 38 309.5 32 265.2
Coosa 32 302.4 24 223.2 25 233.3 28 262.6
Covington 88 234.9 130 350.5 107 289.3 104 280.7
Crenshaw 44 316.3 40 288.4 29 209.8 51 370.3
Cullman 172 208.6 180 217.5 185 221.7 188 224.4
Dale 107 217.4 108 219.4 110 224.7 108 219.6
Dallas 116 289.9 86 219.3 104 271.5 92 247.3
DeKalb 132 186.2 148 206.7 160 224.1 152 212.5
Elmore 168 205.4 144 176.3 166 202.7 178 219.2
Escambia 95 251.8 100 267.0 93 253.1 96 262.1
Etowah 238 232.1 261 254.0 265 258.5 256 250.3
Fayette 61 368.7 44 267.2 52 316.4 33 202.4
Franklin 68 215.0 62 196.9 72 229.6 71 226.4
Geneva 76 285.6 80 302.8 84 319.2 60 228.4
Greene 18 213.7 23 276.1 24 291.5 16 197.3
Hale 40 267.5 31 209.3 32 217.3 26 177.5
Henry 40 233.0 51 297.4 50 290.5 50 290.6
Data sourced from the ADPH Cancer Epidemiology Division and the ADPH Center for Health Statistics.

2020 ALABAMA STATE HEALTH ASSESSMENT
102
Health Indicator 12 - Cancer by County
County
Overall Cancer Mortality Rate Per 100,000 Persons, 2016-2019
2016
Count
2016 Rate
2017
Count
2017 Rate
2018
Count
2018 Rate
2019
Count
2019 Rate
Houston 220 211.4 243 232.9 207 197.7 195 184.2
Jackson 151 289.6 141 271.6 143 276.4 144 278.9
Jeerson 1,409 213.6 1,347 204.3 1,353 205.2 1,334 202.6
Lamar 42 301.8 39 279.7 37 267.3 42 304.2
Lauderdale 218 236.1 215 232.3 221 239.2 195 210.3
Lawrence 74 222.6 85 257.2 90 273.1 75 227.8
Lee 216 135.9 266 164.6 259 158.0 257 156.2
Limestone 182 196.2 163 172.7 162 168.4 166 167.8
Lowndes 37 357.2 26 258.0 30 300.8 26 267.3
Macon 58 305.9 46 245.3 58 314.6 56 309.9
Madison 673 188.5 634 175.6 667 182.0 646 173.2
Marengo 53 269.4 48 247.7 60 314.7 52 275.7
Marion 69 230.0 92 308.4 85 285.6 84 282.7
Marshall 227 238.6 216 226.1 207 215.4 177 182.9
Mobile 867 209.0 894 216.0 925 223.6 881 213.2
Monroe 42 195.1 56 262.6 59 280.1 37 178.5
Montgomery 405 178.9 446 196.8 452 200.2 416 183.7
Morgan 260 218.5 283 238.2 258 216.6 262 218.9
Perry 21 219.3 27 289.1 24 262.6 20 224.1
Pickens 46 226.3 34 168.5 32 160.5 57 286.0
Pike 77 231.3 70 210.4 64 192.0 66 199.3
Randolph 55 242.8 71 313.2 44 193.6 56 246.5
Russell 126 216.6 139 243.7 112 193.8 135 232.9
Shelby 323 367.0 291 329.9 336 378.8 336 375.4
St. Clair 195 92.6 193 90.4 182 84.4 203 93.2
Sumter 35 268.4 36 283.8 31 244.3 31 249.5
Talladega 207 258.4 207 258.5 197 246.8 192 240.1
Tallapoosa 132 324.1 116 285.1 103 254.3 123 304.7
Tuscaloosa 323 156.7 301 144.8 354 169.5 316 150.9
Walker 189 290.9 195 304.4 187 293.5 169 266.1
Washington 38 226.8 40 242.0 40 244.2 35 214.4
Wilcox 25 227.6 35 326.5 42 395.2 27 260.3
Winston 60 252.0 52 219.2 63 266.3 61 258.2
Data sourced from the ADPH Cancer Epidemiology Division and the ADPH Center for Health Statistics.

2020 ALABAMA STATE HEALTH ASSESSMENT
103
Health Indicator 13 – Diabetes by County
County
Diabetes Mortality Rate Per 100,000 Persons, 2016 - 2019
2016 Rank 2016 Rate 2017 Rank 2017 Rate 2018 Rank 2018 Rate 2019 Rank 2019 Rate
Autauga 22 34.3 38 23.4 11 52.2 18 46.5
Baldwin 62 9.1 51 16.0 54 11.9 49 19.3
Barbour 27 30.8 59 11.9 61 8.0 32 28.4
Bibb 63 8.8 15 44.1 33 26.8 35 26.8
Blount 66 6.9 58 12.1 49 15.6 52 17.3
Bullock 12 48.3 12 48.5 45 19.7 7 59.4
Butler 2 70.0 5 70.6 7 61.0 2 77.1
Calhoun 57 13.1 57 13.1 53 12.3 61 11.4
Chambers 4 62.1 13 47.5 6 62.5 3 75.2
Cherokee 21 35.0 40 23.2 13 49.9 9 57.3
Chilton 61 11.4 52 15.9 43 20.4 66 6.8
Choctaw 51 15.4 27 30.9 63 7.8 30 31.8
Clarke 11 49.2 42 20.8 9 58.5 15 50.8
Clay 53 14.8 67 0.0 64 7.5 65 7.6
Cleburne 56 13.4 56 13.4 44 20.0 59 13.4
Coee 45 17.6 48 17.3 32 27.0 46 21.0
Colbert 48 16.6 66 7.3 58 9.1 43 21.7
Conecuh 25 32.3 6 64.2 21 40.7 8 58.0
Coosa 44 18.9 63 9.3 16 46.7 63 9.4
Covington 28 29.4 29 27.0 23 37.9 19 45.9
Crenshaw 37 21.6 23 36.0 24 36.2 21 43.6
Cullman 15 40.0 46 18.1 34 26.4 28 33.4
Dale 24 32.5 20 38.6 25 34.7 23 38.6
Dallas 39 20.0 43 20.4 47 18.3 50 18.8
DeKalb 13 42.3 35 23.7 12 50.4 51 18.2
Elmore 38 20.8 28 28.2 28 29.3 40 22.2
Escambia 1 74.2 11 50.7 5 65.3 12 54.6
Etowah 26 31.2 21 37.0 15 46.8 31 30.3
Fayette 33 24.2 8 54.7 18 42.6 25 36.8
Franklin 43 19.0 45 19.1 35 25.5 29 31.9
Geneva 6 56.4 31 26.5 8 60.8 5 68.5
Greene 19 35.6 1 96.0 2 85.0 17 49.3
Hale 30 26.8 14 47.3 26 34.0 47 20.5
Henry 34 23.3 25 35.0 10 52.3 27 34.9
Data sourced from the AL Medicaid Agency and the ADPH Center for Health Statistics.

2020 ALABAMA STATE HEALTH ASSESSMENT
104
Health Indicator 13 – Diabetes by County
County
Diabetes Mortality Rate Per 100,000 Persons, 2016-2019
2016 Rank 2016 Rate 2017 Rank 2017 Rate 2018 Rank 2018 Rate 2019 Rank 2019 Rate
Houston 55 14.4 41 21.1 51 14.3 56 15.1
Jackson 32 24.9 34 25.0 31 27.1 25 36.8
Jeerson 36 22.9 33 25.2 40 21.4 44 21.3
Lamar 10 50.3 4 78.9 17 43.3 16 50.7
Lauderdale 58 13.0 62 9.7 52 14.1 52 17.3
Lawrence 52 15.0 64 9.1 58 9.1 11 54.7
Lee 23 32.7 32 25.4 29 29.3 33 28.0
Limestone 65 7.5 55 13.8 57 9.4 60 13.1
Lowndes 3 67.6 3 79.4 3 70.2 14 51.4
Macon 50 15.8 30 26.7 39 21.7 41 22.1
Madison 42 19.3 47 17.7 49 15.6 57 14.5
Marengo 19 35.6 18 41.3 67 0.0 45 21.2
Marion 67 6.7 44 20.1 48 16.8 24 37.0
Marshall 54 14.7 53 15.7 36 23.9 55 15.5
Mobile 31 25.6 38 23.4 42 21.0 39 22.7
Monroe 29 27.9 9 51.6 14 47.5 36 24.1
Montgomery 14 40.6 16 43.2 19 42.5 13 51.7
Morgan 47 16.8 50 16.8 55 10.9 58 14.2
Perry 8 52.2 17 42.8 38 21.9 20 44.8
Pickens 41 19.7 61 9.9 65 5.0 48 20.1
Pike 18 39.1 10 51.1 22 39.0 34 27.2
Randolph 63 8.8 24 35.3 67 0.0 67 4.4
Russell 5 58.4 2 80.6 4 65.8 4 70.7
Shelby 59 11.9 65 8.9 60 8.8 54 16.8
St. Clair 49 15.9 54 14.7 40 21.4 64 8.3
Sumter 35 23.0 37 23.6 62 7.9 36 24.1
Talladega 16 39.9 35 23.7 46 18.8 38 23.8
Tallapoosa 17 39.3 19 39.3 20 42.0 22 42.1
Tuscaloosa 46 17.0 60 11.5 56 9.6 62 9.6
Walker 39 20.0 49 17.2 37 23.5 42 22.0
Washington 59 11.9 22 36.3 1 85.5 6 61.3
Wilcox 7 54.6 7 56.0 30 28.2 1 86.8
Winston 9 50.4 26 33.7 27 33.8 10 55.0
Data sourced from the AL Medicaid Agency and the ADPH Center for Health Statistics.

2020 ALABAMA STATE HEALTH ASSESSMENT
105
Health Indicator 14 – Tobacco Usage and Vaping by County
County
Adults Currently Smoking by
County, 2018
County
Adults Currently Smoking by
County, 2018
Rank % Rank %
Autauga 57 19.4 Houston 42 21.6
Baldwin 65 17.5 Jackson 25 22.6
Barbour 5 24.5 Jeerson 64 18.0
Bibb 23 22.7 Lamar 25 22.6
Blount 33 22.1 Lauderdale 63 18.4
Bullock 6 24.4 Lawrence 16 23.2
Butler 45 21.4 Lee 62 18.5
Calhoun 52 20.4 Limestone 53 20.2
Chambers 35 22.0 Lowndes 1 25.0
Cherokee 39 21.8 Macon 55 20.1
Chilton 21 22.8 Madison 66 16.7
Choctaw 45 21.4 Marengo 40 21.7
Clarke 21 22.8 Marion 25 22.6
Clay 13 23.6 Marshall 31 22.2
Cleburne 18 22.9 Mobile 53 20.2
Coee 50 20.7 Monroe 9 23.8
Colbert 48 20.8 Montgomery 57 19.4
Conecuh 9 23.8 Morgan 55 20.1
Coosa 18 22.9 Perry 3 24.6
Covington 38 21.9 Pickens 25 22.6
Crenshaw 35 22.0 Pike 57 19.4
Cullman 40 21.7 Randolph 42 21.6
Dale 48 20.8 Russell 31 22.2
Dallas 12 23.7 Shelby 67 14.7
DeKalb 7 24.3 St. Clair 47 21.1
Elmore 60 19.1 Sumter 51 20.5
Escambia 3 24.6 Talladega 17 23.1
Etowah 33 22.1 Tallapoosa 30 22.3
Fayette 23 22.7 Tuscaloosa 60 19.1
Franklin 35 22.0 Walker 14 23.5
Geneva 9 23.8 Washington 18 22.9
Greene 2 24.7 Wilcox 8 24.1
Hale 25 22.6 Winston 15 23.3
Henry 44 21.5
Data sourced from the CDC BFRSS online dashboard.

2020 ALABAMA STATE HEALTH ASSESSMENT
106
ADPH Public Health Districts
Jefferson
Southeastern
Southwestern
Mobile
Lauderdale
Colbert
Franklin
Marion
Winston
Walker
Limestone
Lawrence
Morgan
Cullman
Madison
Jackson
Marshall
DeKalb
Cherokee
Etowah
Blount
St. Clair
Calhoun
Cleburne
Clay
Talladega
Randolph
Chambers
Tallapoosa
Coosa
Jefferson
Lamar
Fayette
Tuscaloosa
Bibb
Hale
Sumter
Perry
Dallas
Marengo
Choctaw
Washington
Clarke
Monroe
Conecuh
Butler
Crenshaw
Pike
Barbour
Henry
Dale
Coffee
Geneva
Houston
Covington
Escambia
Baldwin
Mobile
Wilcox
Lowndes
Montgomery
Autauga
Chilton
Elmore
Macon
Bullock
Russell
Lee
Greene
Pickens
Shelby
East Central
Northeastern
Northern
West Central

2020 ALABAMA STATE HEALTH ASSESSMENT
107
AL Community Health Issues Survey (1 of 2)
11
Appendix 1-Community Health Issues Surveys

2020 ALABAMA STATE HEALTH ASSESSMENT
108
AL Community Health Issues Survey (2 of 2)
12

2020 ALABAMA STATE HEALTH ASSESSMENT
109
Acronym List
Acronym Words
AA African American
ADEM
Alabama Department of Environmental
Management
ADPH Alabama Department of Public Health
AHA American Health Association
AIDS Acquired immunodeficiency syndrome
AL Alabama
ALDOL Alabama Department of Labor
ALDOT Alabama Department of Transportation
ALSDE Alabama State Department of Education
ASCR Alabama Statewide Cancer Registry
ATSDR Agency for Toxic Substances and Disease
AVDRS Alabama Violent Death Reporting System
BCBS Blue Cross Blue Shield
BMI Body Mass Index
BRFSS Behavioral Risk Factor Surveillance System
CDC Centers for Disease Control and Prevention
CHA Community Health Assessment
CHIS Community Health Issues Survey
CI Confidence Interval
CLRD Chronic Lower Respiratory Disease
CVD Cardiovascular Disease
DHR Department of Human Resources
EHA End HIV Alabama
EMS Emergency Medical Services
EPA Environmental Protection Agency
EVALI E-cigarette or vaping, use-associated lung injury
FBI Federal Bureau of Investigation
FDA Food and Drug Administration
FQHC Federally Qualified Health Centers
FTE Full-time Employees
GBM Gay and Bisexual Men
GED General Educational Development
HIV Human Immunodeficiency virus
HPSA Health Professional Shortage Areas
HPV Human Papillomavirus
HRSA Health Resources and Services Administration
LGBTQ+ Lesbian, Gay, Bisexual, Transgender, and Queer
MCH Maternal and Child Health
N/A Not Applicable
NIH National Institute of Health
NPA Nutrition and Physical Activity
OB-GYN Obstetrics and Gynecology
OCPS Oce of Child Protective Services
PRAMS Pregnancy Risk Assessment Monitoring System
PWS Public Water Systems
SAMHSA
Substance Abuse and Mental Health
Services Administration
SDOH Social Determinants of Health
SDWA Safe Drinking Water Act
SHA State Health Assessment
SIDS Sudden Infant Death Syndrome
SNAP Supplemental Nutrition Assistance Program
STD Sexually Transmitted Diseases
STI Sexually Transmitted Infections
SVI Social Vulnerability Index
U.S. United States
UCR Uniformed Crime Reporting
USDA U.S. Department of Agriculture
USDHHS U.S. Department of Health and Human Services
USHUD
U.S. Department of Housing and
Urban Development
WHO World Health Organization
WONDER
Wide-ranging Online Data for
Epidemiologic Research
YMCA Young Men’s Christian Association
YRBSS Youth Risk Behavioral Surveillance System

2020 ALABAMA STATE HEALTH ASSESSMENT
110
Data Definitions and Technical Notes
Age–adjusted Rate – The total number of events,
or counts, divided by the population of interest, and
statistically adjusted for age dierence. Often, rates are
influenced by underlying age distribution, so this method
permits unbiased comparisons between groups. For
example, the cancer incidence data uses age-adjusted
rates for new cases.
Confidence Interval – A range of values defined so
there is a probability that the value falls between the
interval and the observed value. In this assessment, we
assume a 95percent confidence interval.
Crude Rate – The total number of events, or counts,
divided by the total population of interest. The number is
typically multiplied by a population rate of 1,000, 10,000, or
100,000 persons. For example, the leading cause of death
and mortality data use crude rates with 100,000 persons.
Incidence – The number of new cases of a condition,
symptom, death, or injury that develop in the population
during a specific time period.
Prevalence – The total number of individuals in a population
who have a disease or health condition at a specific time
period and is usually expressed as a percentage.
Rank – The appendix includes the ranking of rates by
county from most severe (1) to least severe (67). If
multiple counties had no data provided or a rate less
than 1, a rank of 67 was given to them.
Rural/Urban Status – This is defined at the county
level since most data are not available at the sub-
county levels. The SHA definition considers the
following counties to be urban: Calhoun, Etowah,
Houston, Jeerson, Lauderdale, Lee, Madison, Mobile,
Montgomery, Morgan, Shelby, and Tuscaloosa.
Uninsured – People who are not covered by any of the
following types of health coverage plans: insurance
through a former or current employer, insurance
directly purchased from an insurance company,
Medicare, Medicaid, TRICARE, Indian Health Services,
the Department of Veterans Aairs, and any other
government or military healthcare.
Data Limitations
Sources of the data used in this report were selected
based upon accepted reliability, completeness,
timeliness, and availability of the source. Data in this
publication are generally presented as frequencies, rates,
and percentages confined between the years 2016-2019.
Rounding errors may exist because of the estimation
techniques. Where data are not available, “N/A” or a dash
are indicated. All other assumptions and sources are
included with the data referenced.
BRFSS Data
BRFSS data are a cross-sectional telephone survey
that state health departments conducted monthly
over landline and cellular telephones. Prevalence data
among U.S. adults are used regarding their risk behaviors
and preventative health practices that can aect their
health status. A weighted multiplier is used to get to an
estimated average.
Cancer Data
The AL Statewide Cancer Registry was the primary source
for cancer data. The data are sourced from provider
confirmed incidence cases throughout the state. The
adjusted rates are used over a 5year incidence.
Census Data
The U.S. Census Bureau American Community Survey
1- and 5-year estimates were the primary source for the
state-level population, housing, and economic data.
County-level population statistics are based on vintage
year 07V2019. Dierent vintage years of estimates are
not comparable.
Medicaid Data
The Medicaid data were specially requested to include
the years 2017 and 2018. The numbers used in this
assessment include the total Medicaid population of
children and adults.
Medicare Data
The Centers for Medicare and Medicaid dashboard was
the source for Medicare data for county-level population
statistics. The prevalence data include all Medicare
recipients in the year 2018.
Mortality Data
The AL Center for Health Statistics was the source
for mortality data. The data are provided through
death certificates as the underlying cause of death.
Only diabetes-related mortality uses the primary
cause of death. Deaths are classified according to the
International Classification of Diseases, Tenth Revision,
and follow the National Center for Health Statistics
instructions. The crude rates are given for 2019.
Natality Data
The AL Center for Health Statistics was the primary
source for natality data. The data are provided through
birth certificates. The crude rates are given for 2019.

2020 ALABAMA STATE HEALTH ASSESSMENT
111
Acknowledgements
The SHA team members wish to thank those who gave
their time and expertise to help the team complete the
State Health Assessment (SHA). This report includes
partners from the community, individuals, workgroups
within ADPH, and additional members outside ADPH. The
workgroup recognizes your countless hours, eorts, and
endless analyses to finalize this project.
ADPH Leadership
• Carolyn Bern
• Michele Jones
• Ricky Elliot
Work Group Members and Data Contributors
• Carrie Allison
• Sondra Reese
• Carlene Robinson
• Janice Cook
• Jamey Durham
• Jocole Green
• Nancy Bishop
• Sherry Bradley
• Betsy Cagle
• Lita Chatham
• Danita Crear
• Sherri Davidson
• Maegan Ford
• Justin George
• April Golson
• Debra Grin
• Debra Hodges
• Stuart Hoyle
• Dana Human
• Sarah Khalidi
• Anthony Merriweather
• Carolyn Miller
• Melissa Morrison
• Niko Phillips
• Brandi Pouncey
• Kortnei Scott
• Xuejun Shen
• Gary Varner
• Brandon Williams
• Nancy Wright
Stakeholder Group Members
• AIDS Outreach
• Alabama Academy of Family Physicians
• Alabama Chapter- American Cancer Society
• Alabama Health Education Center
• Alabama Rural Health Association
• Auburn University
• Blue Cross and Blue Shield of Alabama
• University of Alabama at Birmingham, School of
Public Health
• University of Alabama School of Medicine –
Birmingham, Huntsville, Montgomery, and
Tuscaloosa Campuses
• University of South Alabama College of Medicine
• Debra McCallum, PhD, Director of Institute
for Social Science Research, Director of the
Capstone Poll
Alabama State and Local Agencies
• Alabama DHR
• Alabama Department of Labor
• Alabama Department of Mental Health
• Alabama Law Enforcement Agency
• Alabama Medicaid Agency
• Alabama Rural Development Oce
• Alabama Oce of Telehealth
• Jeerson County Health Department
• Mobile County Health Department
• Local County Health Departments

2020 ALABAMA STATE HEALTH ASSESSMENT
112
For more information, contact:
Carlene A. Robinson, M.P.H.
Alabama Department of Public Health
Bureau of Prevention, Promotion, and Support
201 Monroe Street, Montgomery, Alabama 36104
www.alabamapublichealth.gov/accreditation
(334) 206-5051
Acknowledgement of funding source:
This project was supported by funds made
available from the Centers for Disease Control
and Prevention, Oce for State, Tribal, Local,
and Territorial Support.
Disclaimer:
The contents of this article are those of the
authors and do not necessarily represent the
ocial position of or endorsement by the
Centers for Disease Control and Prevention.
